
Abstract
BACKGROUND:
The cup inclination in total hip arthroplasty is key to minimising complications. Stereometric effects (parallax) in two-dimensional projections can alter angle measurements. Even for different approaches, fluoroscopy causes different results in the measurement of inclination. A previous study has introduced a corrective factor for intraoperative radiographic cup inclination measurements compared to the postoperative standing radiographs.
OBJECTIVE:
The aim of this study was to find out whether, first, the correction factor is reproducible and second, whether the correction factor is independent of the surgical approach and C-arm model used.
METHODS:
A series of 377 cases of primary total hip arthroplasty was reviewed. We compared the cup inclination angle in the intraoperative and postoperative radiographic images. Based on this, it was possible to specify a standard of correction factor in defined ranges.
RESULTS:
The mean cup inclination in intraoperative images was 37.47
CONCLUSION:
An added correction factor of 4
Keywords
Introduction
The inclination in primary total hip arthroplasty (THA) is key to minimising complications and guaranteeing an optimal fitting of the arthroplasty into the natural pelvis. In general, cup inclination is oriented from the trajectory of both tear-drop figures of the pelvis. The targeted cup positioning is within the so called Lewinnek’s safe zone with an inclination of 40
The use of fluoroscopy is controversial in primary THA, as fluoroscopy increases the surgical time and costs [5]. However, intraoperative X-ray analysis gives surgeons the possibility to correct implant orientation to desired angles. Thus, using intraoperative fluoroscopy can significantly improve cup positioning and inclination as previous publications have shown.
Nevertheless, stereometric effects (parallax) in two-dimensional projections can alter angle measurements [6]. Even for different surgical approaches, fluoroscopy causes different results in the measurement of inclination [7]. Although exact measurements or calculation of angles are not very common in daily practice, the above-mentioned considerations must be taken into account, when the angles of intraoperative fluoroscopy pictures are estimated by the surgeon and his team. A previous study has introduced a corrective factor for intraoperative radiographic cup inclination measurements (RI) compared to the postoperative standing radiographs [8]. In the mentioned study a correction factor of 5
Material and methods
We retrospectively reviewed cases of primary total hip arthroplasty performed in the period of 2013 to 2017 in the university hospital Cologne. Only cases of primary osteoarthritis were eligible, any revision surgery or different cup fixation (e.g. screw) techniques were excluded. Of the 516 eligible patients, 113 were excluded due to alternative cup fixation. Further 34 patients were excluded due to inappropriate imaging, leaving 377 patients with complete images and data. All patients included in the study underwent THA with an uncemented acetabular component (Pinnacle, DePuy Synthes, Warsaw, IN, USA) and with either a cemented or uncemented stem. On all patients the modified lateral approach to the hip was performed. The study was approved by the institutional ethics committee (EN 21-1038).
Radiographic evaluation
A Philips BV Endura (Philips Medical Systems DMC GmbH, Hamburg, Germany) Image Intensifier was used for intraoperative fluoroscopy. The patient was in a supine position and the detector of the C-arm was placed as close to the patient as possible to reduce radiation. Images were taken centred over the symphysis with symmetrical obturator foramina, thus both tear-drop figures were visible. All patients underwent standardised preoperative and postoperative weight-bearing anterior to posterior (AP) pelvic radiographs with the x-beam centred on the symphysis (source-to-film distance (SID) of 100 cm). In the underlying study, inclination is defined as radiographic inclination (RI). Radiographic inclination (RI) is defined as the angle
We performed double-observer measurements to determine in RI of the intraoperative fluoroscopy images (IRI) and of the postoperative standing a.p. radiographs (PRI). Measurements were performed using the institutional picture archiving and communication system (IMPAX EE; Agfa Healthcare N.V., Mortsel, Belgium). To check the internal consistency of the measurements, a reliability analysis was performed. The intraclass correlation coefficient (ICC) is determined as an indicator of reliability.
Statistical analysis
Descriptive statistics were performed to summarise the means, medians, and ranges for all variables. Paired t test (for normally distributed values) or the Wilcoxon-rank-sum test (for non-normally distributed values) was performed to identify significance. Statistical analysis was performed for a 95% confidence interval. Results with
Results
The study included 369 patients with a modified lateral surgical approach, 182 (49.32%) were male and 187 (50.68%) were female. At the time of surgery, the patients had an overall mean age of 64.25 years (range 18–90). Male patients had a mean age of 61.51 years (range 22–85) and female patients had a mean age of 66.97 years (range 18–90). This study analyzed 188 left-sided THAs and 181 right-sided THAs. The mean angle of IRI was 37.47
The inclination angles IRI and PRI and the difference between IRI and PRI (DRI) were analyzed using
Side and gender related differences of the mean values of DRI
Side and gender related differences of the mean values of DRI
Values of intraoperative and postoperative inclination angles
Furthermore, patient age was examined for any relationship with IRI, PRI and DRI. Pearson’s correlation showed that IRI (
In another step, we added a correction factor (CF) to IRI and tested against PRI. We added 2
Correction of the intraoperative angle correlating to the postoperative inclination angle.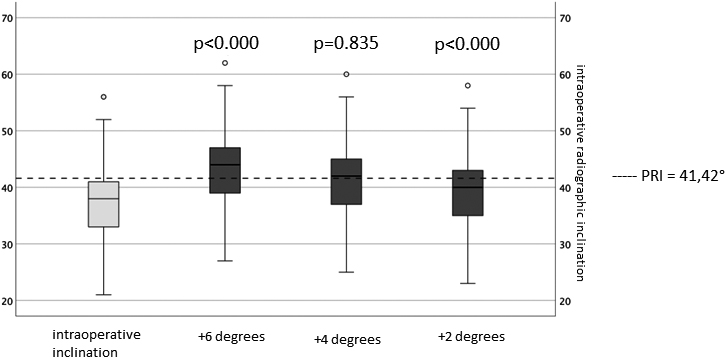
Through the preliminary study by Rueckl et al., the idea of a correction factor (CF) in cup positioning during implantation of total hip arthroplasty was introduced [8]. We analyzed whether the correction factor is reproducible and, second, whether the correction factor is independent of the surgical approach and C-arm model used. The group found a deviation of 5
sDue to the distinct range of IRI among our study population (21
Difference in angular inclination depending on the intraoperative angle.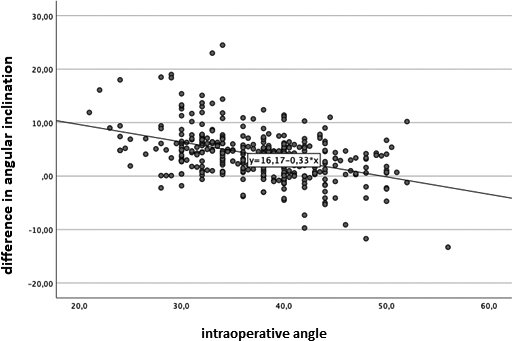
It is known that different C-arm models produce different parallax effects. The correction factor for the 12-inch GE 9900 elite C-arm (GE Healthcare, Chicago, IL) was calculated as 5
Intraoperative measurement of cup inclination angle.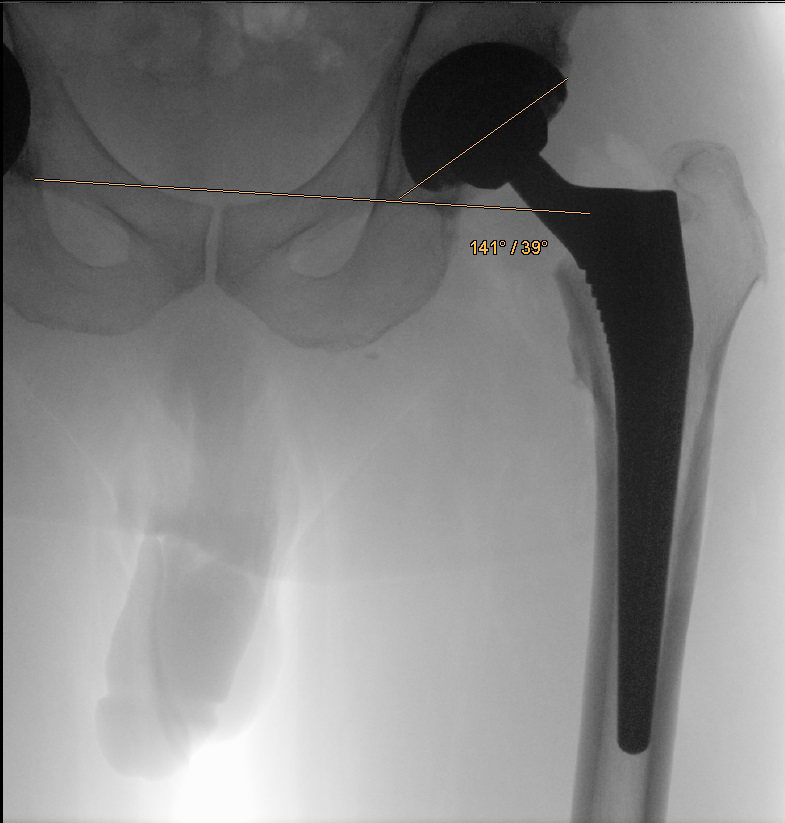
Postoperative measurement of cup inclination angle.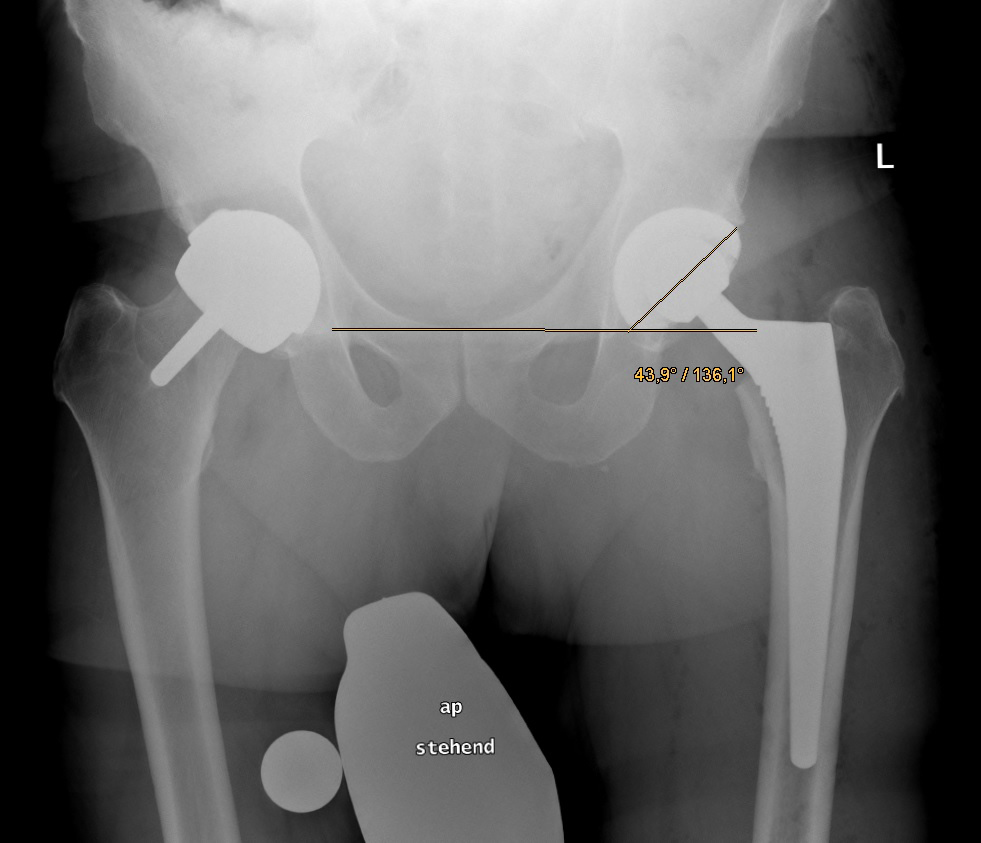
In the study by Rueckl et al., the direct anterior approach (DAA) was used as the only surgical approach. In contrast, the modified lateral approach was used as the only surgical approach in our study. Since an almost identical factor was found in both studies, we interpreted this as being independent of the surgical approach.
In synopsis, the consideration of a correction factor of about 4
We were able to successfully reproduce the correction factor as described in the preliminary study by Rueckl et al. and thus substantiate the relevance of an intraoperative correction factor for optimal cup positioning during implantation of a total hip arthroplasty.
While it was calculated for the direct anterior approach before, we have shown that the correction factor is also valid for the lateral approach to the hip and independent of the C-arm model used. From our calculations we can recommend adding a correction factor of 4
Limitations
The parallax effects may differ from various C-arm models. The given correction factor is calculated for the Philips BV Endura. However, the actual effects and their significance of different C-arm models on parallax effects remains unclear. Furthermore, we calculated the correction factor based on the data that we collected in a university hospital as described. The resulting variance in cup positioning influences the calculation of the correction factor. Other clinics with a different setting will presumably produce a different variance in cup inclination and thus possibly receive a slightly different correction angle.
We did not calculate our findings with correlation to the body mass index of the patients. Body mass alters the distance (in mm/cm) of C-Arms to the individual hip cup center. This may also affect the calculation of the correction factor.
We did not perform a subgroup analysis for different cup sizes. From our findings it remains unclear, whether the cup size itself influences the angulation or the calculated correction factor.
Funding
The authors received no financial support for the preparation, research, authorship, and/or publication of this manuscript.
Ethical approval
A positive vote was given by the medical ethics committee of the University of Cologne (EN 21-1038).
Informed consent
The authors declare that there is no information (names, initials, hospital identification numbers, or photographs) in the submitted manuscript that can be used to identify patients.
Footnotes
Acknowledgments
None to report.
Conflict of interest
The authors do not have any potential conflicts of interest for this manuscript.