
Abstract
BACKGROUND:
In recent years, lower limb walking exoskeletons have been widely used in the study of spinal cord injury (SCI).
OBJECTIVE:
To explore the effect of a lower limb walking exoskeleton on quality of life and functional independence in patients with motor complete SCI.
METHODS:
This was a multi-center, single blind, randomized controlled trial. A total of 16 SCI patients were randomly assigned to either the exoskeleton-assisted walking (EAW) group (
RESULTS:
There was an increasing tendency of scores in the psychological health, physical health, and social relationships domain of WHOQOL-BREF in the EAW group after the intervention compared with the pre-intervention period, but there was no significant difference (
CONCLUSION:
A lower limb walking exoskeleton may have potential benefits for quality of life and activities of daily living in patients with motor complete SCI.
Introduction
Spinal cord injury (SCI) is a central nervous system disorder in which the structure and function of the nerves in the spinal canal are impaired, resulting in dysfunction of sensation, movement, and reflexes [1]. Studies have found that only 0.4% of SCI patients achieve complete functional recovery, while the rest are left with varying degrees of paralysis, which limits patients’ independence in daily activities and becomes an important factor in the reduced quality of life for most SCI patients [2].
The lower limb walking exoskeleton is an intelligent, assistive, orthopedic and compensatory rehabilitation equipment. In recent years, lower limb walking exoskeletons have been widely used in the study of SCI as an alternative/compensatory therapy for SCI, which can provide repetitive, efficient, and assisted walking training to help patients achieve postural transition from sitting to standing to walking [3, 4, 5]. It has been shown that SCI patients with complete motor impairment of the lower limbs can walk safely with the help of a powered exoskeletons that can help SCI patients walk safely, improve their pulmonary and bowel function, but with no significant improvement in motor function [6, 7, 8, 9]. For quality of life, studies have found the potential benefits of powered exoskeletons in the area of health-related quality of survival [10]. Therefore, the aim of this study was to observe the effect of exoskeleton-assisted walking (EAW) training on quality of life and activities of daily living (ADL) in motor complete SCI patients through a randomized controlled trial.
Method
Study design and ethical statement
We conducted a clinical trial with a multicenter randomized, single-blind, parallel group design. The study protocol was approved by the Medical Ethics Committees of The General Hospital of Western Theater Command, Chengdu Gu Lian Rehabilitation Hospital and Sichuan Rehabilitation Hospital (2020ky011, 5, CKIL-2020028) and registered with the Chinese Clinical Trials Registry (ChiCTR2000035955). All participants signed an informed consent form.
Allocation
We recruited eligible SCI patients from three hospitals in Chengdu from October 2020 to July 2021. Inclusion criteria included (1) men aged 20–60 years; (2) meeting the diagnostic criteria of grade A and B in the 2019 International Standards for Neurological Classification of Spinal Cord Injury [11], with an injury level between the second thoracic vertebrae and the first lumbar vertebrae; (3) intact skin and limbs were structurally intact limbs; (4) height 155–190 cm and weight not exceeding 90 kg; (5) participants with sitting balance at least level 1 sitting balance, and can stand with the help of assisted devices but can’t walk independently; (6) participants who understand the significance of the study, have sufficient compliance with this study, and sign an informed consent form. Exclusion criteria were as follows: (1) muscle tension of grade 2 or higher (determined by modified Ashworth scale) in both lower extremities; (2) patients with a systolic blood pressure
Randomization and blinding
The random number table was generated by computer, and the envelopes with the words “EAW group” and “routine group” were prepared by the personnel unrelated to the test according to the ratio of 1:1 based on the random number table. The envelopes were extracted according to the enrollment time, and the subjects were informed that they would enter the EAW group or the conventional group. The whole experiment was unblinded by a third party. Due to significant differences in treatment modalities, only assessors, data entry personnel, and analysts unrelated to the trial were single-blinded.
Intervention
Both the conventional control group and the EAW group were treated with the routine exercise therapy based on expert consensus [1].
In the EAW group, additional EAW training was performed for 40–50 minutes, including sitting, standing and walking training, once a day, five times a week for 8 weeks. The oxygen saturations of participants were detected before training to prevent adverse events; the patients’ heart rate was monitored during training and was maintained below 80% of the expected maximum heart rate (220-age). The walking speed and rest time depended on the subjects’ tolerance level. Knee pads, ankle pads and sports shoes were worn during training to protect the participants’ joints.
Outcomes
Functional independence and quality of life assessments were performed before and after 8 weeks of training. (1) WHOQOL-BREF [12]: was used to assess the quality of life of patients. The WHOQOL-BREF contains 4 dimensions: physical health domain, psychological health domain, social relationships domain and environment domain, with a total score of 100, and the higher the score, the higher the quality of life. (2) SCIM-III: this scale is used to assess the functional independence of patients with SCI. SCIM-III has 19 items, including 3 dimensions of self-care, respiratory and sphincter management, and activity, with a total score of 0 to 100. The higher scores indicate better functional independence of the patient.
Statistical analysis
All statistical analyses were performed using SPSS version 23 (IBM Corp., Armonk, NY, USA). The level of significance was set at 0.05. Data conforming to a normal distribution were expressed as mean
Results
Patients
A total of 79 SCI patients were screened, 59 of whom were excluded (
Baseline characteristics of participants in the EAW group and the conventional group
Baseline characteristics of participants in the EAW group and the conventional group
EAW: exoskeleton-assisted walking, DOI: duration of injury, AIS: international standards for the neurological classification of an SCI, LOI: level of injury.
CONSORT diagram of enrollment of the study participant.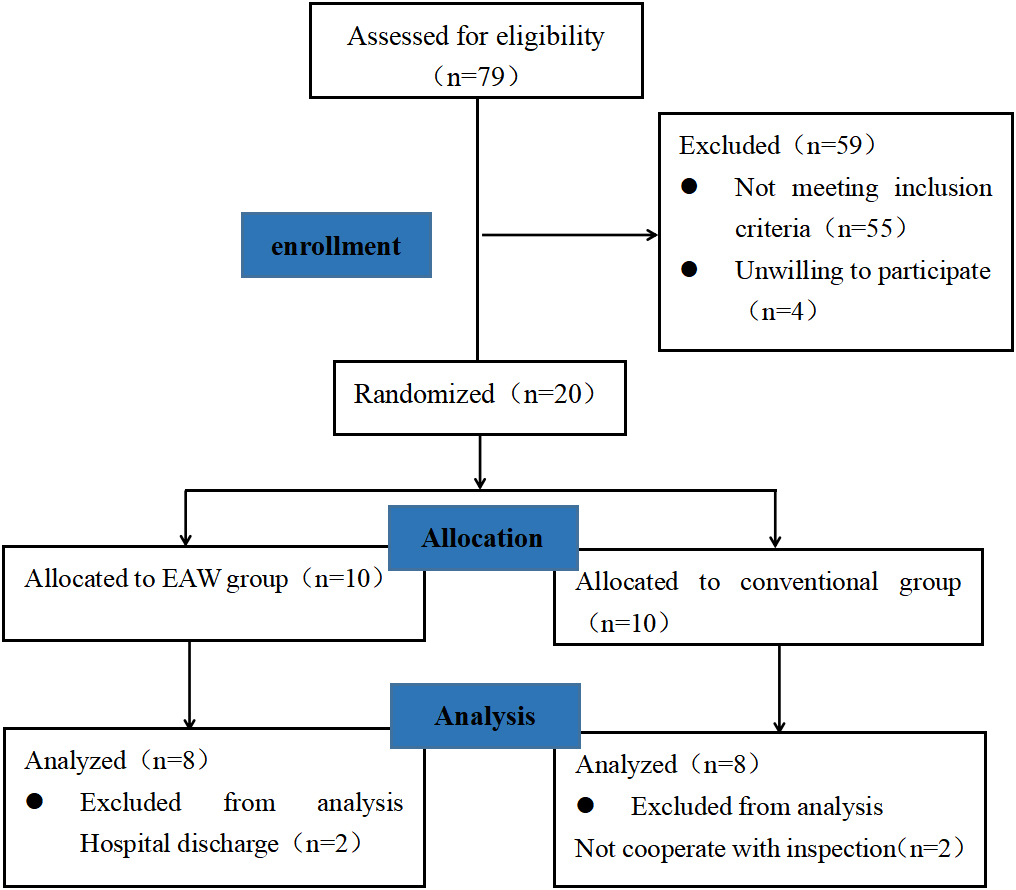
The detailed results of SCIM are shown in Table 2. Before the training, there was no significant difference in the scores of each field of the WHOQOL-BREF between the two groups (
Outcomes of WHOQOL-BREF
Outcomes of WHOQOL-BREF
Comparison of results pre- and post-training in EAW group.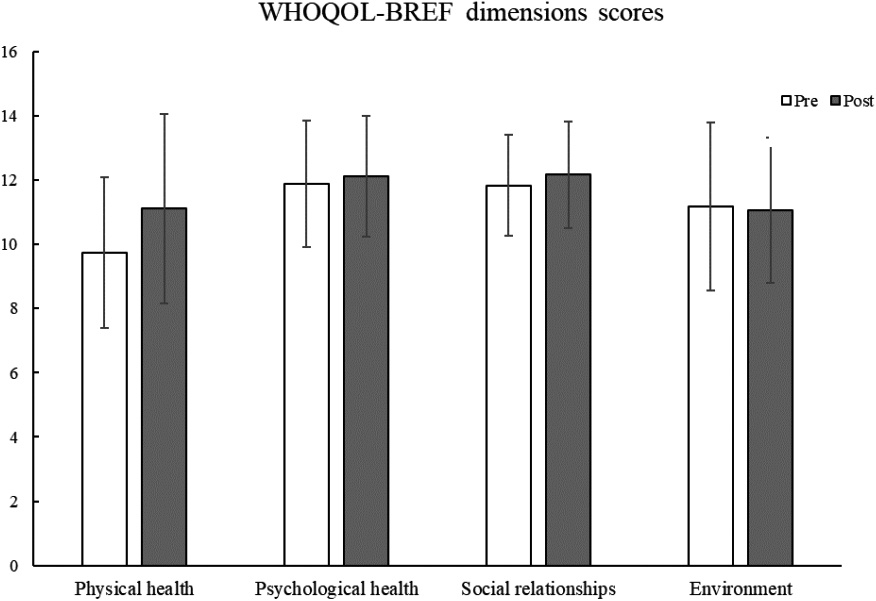
The SCIM-III scores of patients in the EAW group before training and after 8 weeks of training were not significantly different compared with the conventional group (
Outcomes of SCIM-III
Outcomes of SCIM-III
SCI
Restricted mobility in patients with SCI is one of the most important factors leading to reduced quality of life and functional independence. Limited mobility and consequent reduction of overall activity level will further impair physical fitness. Restoring the ability to walk is crucial for SCI patients, especially those with motor complete impairment, where motor dysfunction is more severe and more restrictive to daily life. The wheelchair is the preferred travel tool for SCI patients, but there is still a huge difference between it and the upright bipedal walking of healthy people, as the wheelchair does not provide the physical and psychological benefits of standing and walking [14]. Walking aids and orthoses are commonly chosen walking devices for SCI patients, but they have high requirements on patients’ functional level, are difficult to use and consume large amount of energy, which still limit the overall mobility [15]. In this context, the lower extremity walking exoskeleton emerged, which can take into account both treatment and mobility modes [16]. During exoskeleton-assisted walking, the patient is in a state of upright walking and weight-bearing on both lower limbs, similar to a natural gait pattern, which may increase sensorimotor stimulation to promote the strengthening of lower limb and trunk muscles [17, 18, 19]. Such effective and substantial amount of fully weight-bearing, repetitive, symmetrical exercise training may improve motor function and quality of life [16]. As shown in animal studies, extensive exercise training may promote neuroplasticity in a dose-dependent manner, increasing the likelihood of functional recovery in patients [20, 21].
Artificial intelligence (AI)
AI has made great strides in medicine in recent years. With the assistance of new AI technology, the traditional medical environment has changed dramatically [22]. AI methods have been applied to various areas of cardiology: imaging, electrocardiograms, wearable, risk prediction, and diseases classification [23, 24]. Meanwhile, deep learning algorithms have shown extraordinary advantages in the field of histopathologic diagnosis, such as tumor identification, classification, prognostic prediction, and biomarker/genetic changes prediction [25, 26]. In addition, AI plays an increasingly prominent role in ophthalmology, respiratory diseases [27] and chronic infections [28, 29, 30]. Wearable exoskeleton is an important application of AI in the field of rehabilitation medicine, several studies have confirmed that wearable exoskeleton can significantly improve motor, balance and cardiopulmonary function in patients [31, 32]. Various wearable exoskeleton devices have been developed [33, 34]. The device used in this study was developed by the University of Electronic Science and Technology of China. Previous studies have demonstrated its safety in patients with SCI, however it has not been studied in terms of quality of life and activities of daily living [8].
Quality of life
In previous studies, EAW training has shown substantial advantages on the quality of life in SCI patients. Cruciger et al. [35] trained two chronic SCI patients with exoskeletal support for 12 weeks and both showed significant reductions in pain severity and improvements in all health-related quality of life domains, in addition to improvements in motor function and ambulation. Platz et al. [36] reported a significant increase in physical function scores of patients after EAW training, while the scores of other fields did not show significant changes. In addition, a 22-year-old male showed an increase of more than 20% in physiological function, physical function, somatic pain, general health status, and energy after 6 months of EAW training [37]. Similarly, the EAW group showed an increasing trend in the scores of physiological and psychological domains after 8 weeks of training, which may imply that the patients were less restricted in work and other activities, and may reflect the patients’ higher expectations for the application of exoskeleton robot. Previous studies have found that increased LEMS scores also laterally reflect improved quality of life in terms of health [38, 39]. The time of single assisted walking training for patients in this study was only 40–50 min, which is a large difference compared to 60–120 min in past studies, which may be a possible reason for the trend of increased quality of life only in this trial [40].
ADL
The results of this study showed that SCIM-III scores increased in both groups compared to the pre-training, and there was no significant difference in the comparison between groups. But, the total score of the conventional group increased significantly after 8 weeks of training, and all subcategories (self-care, respiratory and sphincter management, and activity) showed significant increases. This seems to suggest that EAW has a negative impact on patients. However, Tasi et al. [41] found that adding EAW training to standard nursing promoted the functional activity in SCI patients. Another study similarly reported that SCI patients showed positive feedback on activity limitation after EAW training [10]. Baunsgaard et al. [42] also found that SCI patients showed improvement in functional independence after 24 sessions of EAW training, patients in the acute phase showed a significant increase in mobility, while the chronic phase did not show significant changes, and the more pronounced improvement in patients in the acute phase may be attributed to the shorter time of injury and the ascending stage of functional recovery. Although there was no significant difference in the age of the two groups in this trial, there was also a certain gap. During the study period, it was found that the younger SCI patients showed a stronger willingness to recover, while the older ones had lower expectations for future recovery and were significantly more dependent than the younger ones, which may have an impact on the assessment of functional independence after training. Further verification of the correlation between age and functional independence is needed in the future.
Limitations
The increase in scores from this experiment was only a trend change with no significant difference, which is consistent with the results published by Cruciger et al. and Platz et al. Future experiments with large samples are needed to demonstrate the effect of EAW on the quality of life of SCI patients. In addition, in future studies, the inclusion of exoskeleton robot home users could be considered to enhance the observation of long-term efficacy. At the same time, the possible influencing factors such as age, disease duration and injury level should be controlled, and the experimental method of paired design is used for verification.
Conclusion
Assisted walking training via a lower extremity walking exoskeleton for patients with motor-complete SCI in the thoraco-lumbar segment has potential improvements for quality of life and activities of daily living. In addition, exoskeletal robots can assist standing and walking in patients with motor-complete SCI with no reported adverse events. EAW in SCI patients deserves further investigation as a ground-based exercise modality similar to normal walking.
Data availability statement
The datasets generated and analysed during the current study are available from the corresponding author on reasonable request.
Author contributions
WW and JL were involved in the generation of the idea, design of this study and analysis of feasibility. XH and YW contributed to the writing of the manuscript. XH played an important role in acquiring data and interpreting the results. RP, JL, XG, XB and HC were involved in protocol revisions and implementation. JY, CC, QW, HX and YC contributed to the review of this article and references classification. All authors read and approved the final manuscript.
Funding
This study was supported by the Key R&D Projects of Sichuan Science and Technology Plan (No. 2020YFS0168).
Ethical approval
The study protocol was approved by the Medical Ethics Committees of the General Hospital of Western Theatre Command, Chengdu Gu Lian Rehabilitation Hospital, and Sichuan Rehabilitation Hospital (2020ky011, 5, CKIL-2020028).
Footnotes
Acknowledgments
We thank all participants for their cooperation in our study. We thank the Science and Technology Planning Project of Sichuan Province for providing financial support for this study. We also gratefully thank the support for this study provided by the General Hospital of Western Theatre Command, Chengdu Gu Lian Rehabilitation Hospital, and Sichuan Rehabilitation Hospital.
Conflict of interest
The authors report no conflicts of interest.