
Abstract
BACKGROUND:
Stress urinary incontinence is prevalent among women and the incidence increases with age.
OBJECTIVE:
To explore the effect of intelligent pelvic floor muscle rehabilitation on elderly female patients with incontinence.
METHODS:
A total of 209 patients with urinary incontinence who were treated with pelvic floor muscle rehabilitation at Peking University International Hospital from September 2020 to January 2022 were selected by convenient sampling. All subjects were divided into the 50–60 year old patient group (
RESULTS:
The results showed that pelvic floor knowledge and exercise compliance in the experimental group were better than in the control group at 7 and 12 weeks after intervention (
CONCLUSION:
The intelligent pelvic floor rehabilitation model that combines a mobile application with smart dumbbells can maintain and strengthen the clinical treatment effect for elderly patients with urinary incontinence.
Introduction
Stress urinary incontinence (SUI) is an involuntary leakage of urine caused by excessive pressure on the bladder and urethra due to coughing, sneezing, laughing or exercising [1]. It is a common disease affecting about 200 million people around the world [2]. It is prevalent among women and the incidence increases with age. Urinary incontinence in Chinese women is as high as 18.9% [3]. Among them, women over the age of 60 account for 53% of the cases [4]. Although this condition is rarely life-threatening, SUI can severely affect an individual’s physical, psychological and social well-being, as well as quality of life [5]. Interventions may include non-surgical options (e.g. lifestyle changes, pelvic floor muscle training, medication) and surgical options to support the urethra or increase bladder capacity [6, 7, 8]. However, a non-surgical approach is the first-line treatment for SUI. It comprises pelvic floor muscle treatment (PFMT) based on Kegel exercises. Compliance with pelvic floor muscle training among elderly patients is poor due to a lack of knowledge for pelvic floor rehabilitation, dull and monotonous exercises, forgetfulness, a lack of daily supervision and guidance, etc., thus diminishing the rehabilitation effect. Tools available through the application of information technology can not only create a better medical service model for patients but also improve the work efficiency of medical staff [9, 10, 11]. This study aims to combine a mobile phone application (app) with smart dumbbells to construct a mobile intelligent pelvic floor rehabilitation model. With pelvic floor muscle training as the core, the app provides health information, pelvic floor muscle training guidance, real-time and dynamic supervision and reminders. The system automatically records the exercise contraction and relaxation time and intensity, automatically generates test scores and curves and gives feedback reports on results, improving pelvic floor rehabilitation knowledge, exercise compliance, pelvic floor muscle strength and quality of life in elderly patients with SUI.
Materials and methods
General information
This study was approved by the ethics committee of the Peking University International Hospital (approval number: 2021-046 (BMR)), and all patients signed an informed consent form. Using the method of convenient sampling, 209 female patients diagnosed with urinary incontinence in the outpatient department of the Peking University International Hospital from September 2020 to January 2022 were collected.
Inclusion criteria: (1) age
Methods
Data collection methods
The researcher explained the purpose and content of the study to the subjects, signed the informed consent form after obtaining the patients’ consent, and distributed questionnaires to the patients, which included the general information questionnaire, pelvic floor rehabilitation knowledge awareness questionnaire, pelvic floor muscle strength measurement and evaluation and urinary incontinence quality-of-life scale. At 7 and 12 weeks of intervention, the awareness questionnaire of pelvic floor rehabilitation knowledge and urinary incontinence quality-of-life scale were issued. Additionally, a pelvic floor muscle exercise diary was collected and pelvic floor muscle strength was measured in the clinic; the results were evaluated and recorded. Specific data collection methods were: (1) The fixed person in charge of the two groups established health files, including basic data, informed consent, knowledge awareness questionnaires, scoring scales and the pelvic floor muscle training implementation process. (2) Both groups of patients received the same pelvic floor-related knowledge training, including the concept of SUI, its harm to the body, the causes of the disease, the understanding of the pelvic floor muscle group, the factors affecting the muscle group, the correct lifestyle and the methods of pelvic floor muscle training. The control group was given the paper version of the publicity and education materials, and the experimental group was given voice guidance through the mobile phone app. (3) The training time of both groups was two times a day, 20 minutes each time. (4) Both groups of patients made appointments for 7- and 12-week follow-ups for a pelvic floor treatment evaluation at the hospital. The patients’ pelvic floor class I muscle fibres and class II muscle fibres were evaluated for muscle strength, and the patients’ awareness of pelvic floor rehabilitation knowledge, exercise compliance, quality of life and programme implementation were recorded by questionnaire.
Intervention methods
The control group was given routine nursing and home rehabilitation guidance by professional nurses trained in urinary incontinence maintenance. The following intervention methods were implemented: (1) The nurses distributed the pelvic floor function rehabilitation instruction manual [12], ensured the understanding of pelvic floor muscles and taught patients the methods of pelvic floor muscle exercise. (2) The patients recorded their own bladder diary information, including the amount of water consumed, number of urination instances during the day and night, the length of pelvic floor contraction exercises, etc.
The experimental group was guided by the smart app for pelvic floor rehabilitation, which had been developed by the preliminary team. The rehabilitation knowledge guidance and exercise contents in the app were consistent with those in the control group; it contained references to guidelines for the diagnosis and treatment of female SUI [3]. A continuous pelvic floor rehabilitation mode was constructed by the smart app and vaginal dumbbells (see Fig. 1). Method (see Fig. 2). Specific contents of the app included the following: (1) Patients could obtain knowledge of pelvic floor muscles at any time through the app master lecture hall, and the information was presented in the form of text, pictures and videos; (2) Home training was provided to: (a) deliver exercise reminders every day; (b) allow patients to choose from four levels of pelvic floor muscle rehabilitation training courses with increasing difficulty according to their own needs, and carry out pelvic floor muscle contraction and relaxation exercises through animated voice guidance; (c) automatically generate exercise data, including the time of each contraction and relaxation and total duration; (d) prompt the patient to adjust the irregular contraction and relaxation of muscle movements after connecting the vaginal dumbbells to ensure the optimal effect; (3) Patients could establish a WeChat group to have questions answered during exercise in one-hour sessions at a fixed time every day; this encouraged patients to share exercise experiences and increased their enthusiasm for exercise; (4) Weekly telephone follow-ups that provided psychological support helped the patients adjust according to the exercise performance of the research object and correct non-standard actions, and the importance of adhering to pelvic floor exercise and changing bad living habits was emphasised.
Observation indicators
Both groups of patients used the following indicators at the 7
Flowchart of intelligent pelvic floor rehabilitation mode.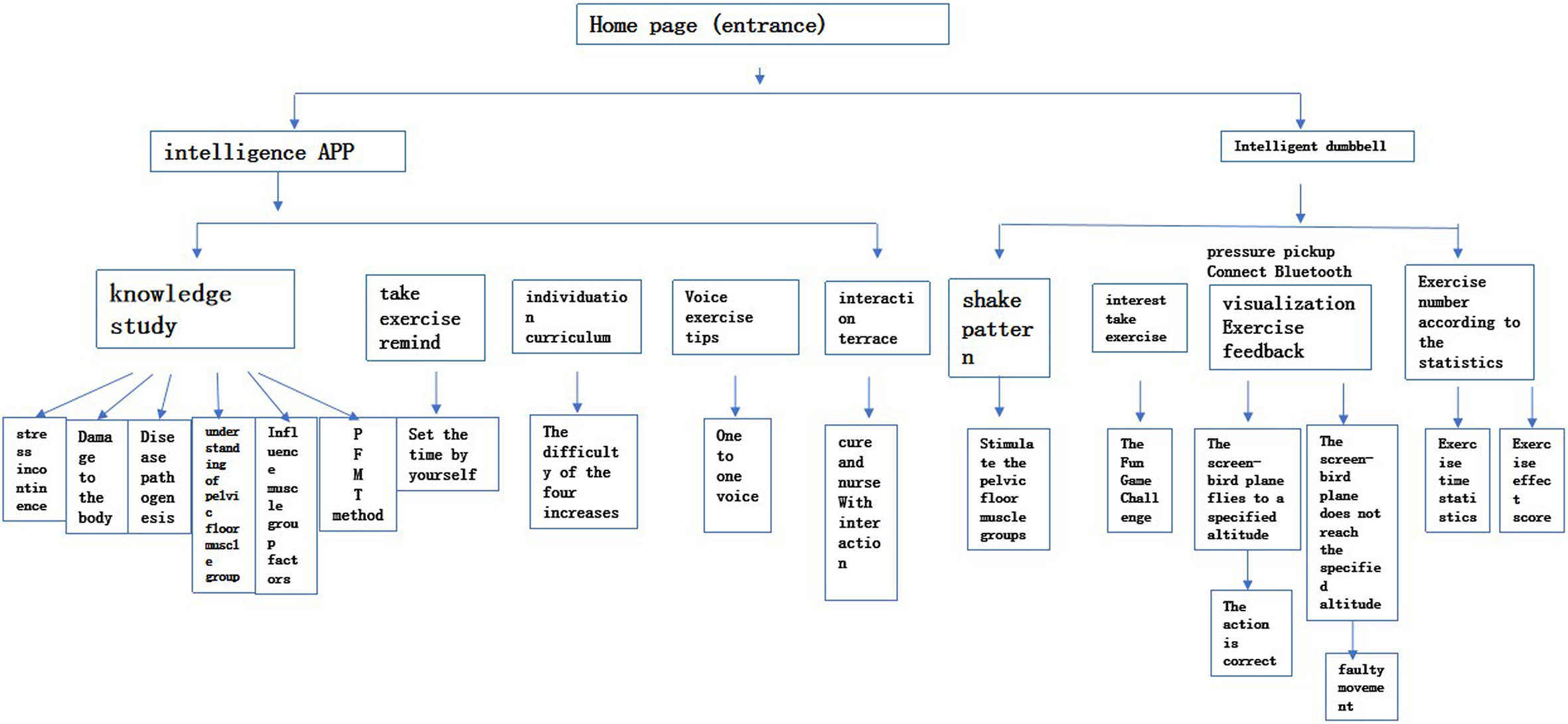
floor rehabilitation knowledge awareness questionnaire was given. The self-developed questionnaire used in this study assessed for the patients’ knowledge and understanding of SUI disease, related lifestyle and other health information and pelvic floor muscle rehabilitation exercises. The content validity index was 0.910. Cronbach’s coefficient of the questionnaire was 0.866; (2) To ensure pelvic floor muscle exercise compliance, patients recorded the frequency, intensity and duration of daily exercise in a pelvic floor muscle exercise diary, and compliance was determined according to the pelvic floor muscle exercise diary and telephone inquiries. The standard exercise frequency was two times a day, 20 minutes each time, for a total of 40 minutes a day, making the total weekly exercise time more than 280 minutes. Patients were considered to be in good compliance when they achieved 50% of their total weekly exercise time (i.e. 140 minutes) [13]; (3) Patients were scheduled to come to the hospital for pelvic floor muscle strength measurement and evaluation at 7 and 12 weeks. In this study, biofeedback electrical stimulation (biofeedback electrical stimulator, model UROSTYM, produced by Canadian Laborie Medical Technologies Co., Ltd.) was used in the gynaecological outpatient department of Peking University International Hospital to evaluate pelvic floor muscle strength (including class I muscle fibres and class II muscle fibres) using a frequency of 50 Hz and a pulse width of 250 us; (4) The Chinese version of the Urinary Incontinence Quality of Life Scale translated by Woodley et al. [14]. The Chinese version of the I-QOL included behavioural limitations, psychological impacts and social barriers, with a total of three dimensions and 22 items. Likert 5 grades were used for all scores, with one to five points assigned from ‘completely like this’ to ‘never like this’, and finally all the scores were accumulated. The higher the score, the better the quality of life. Cronbach’s coefficients of the scales overall were 0.93.
Intelligent APP operation method.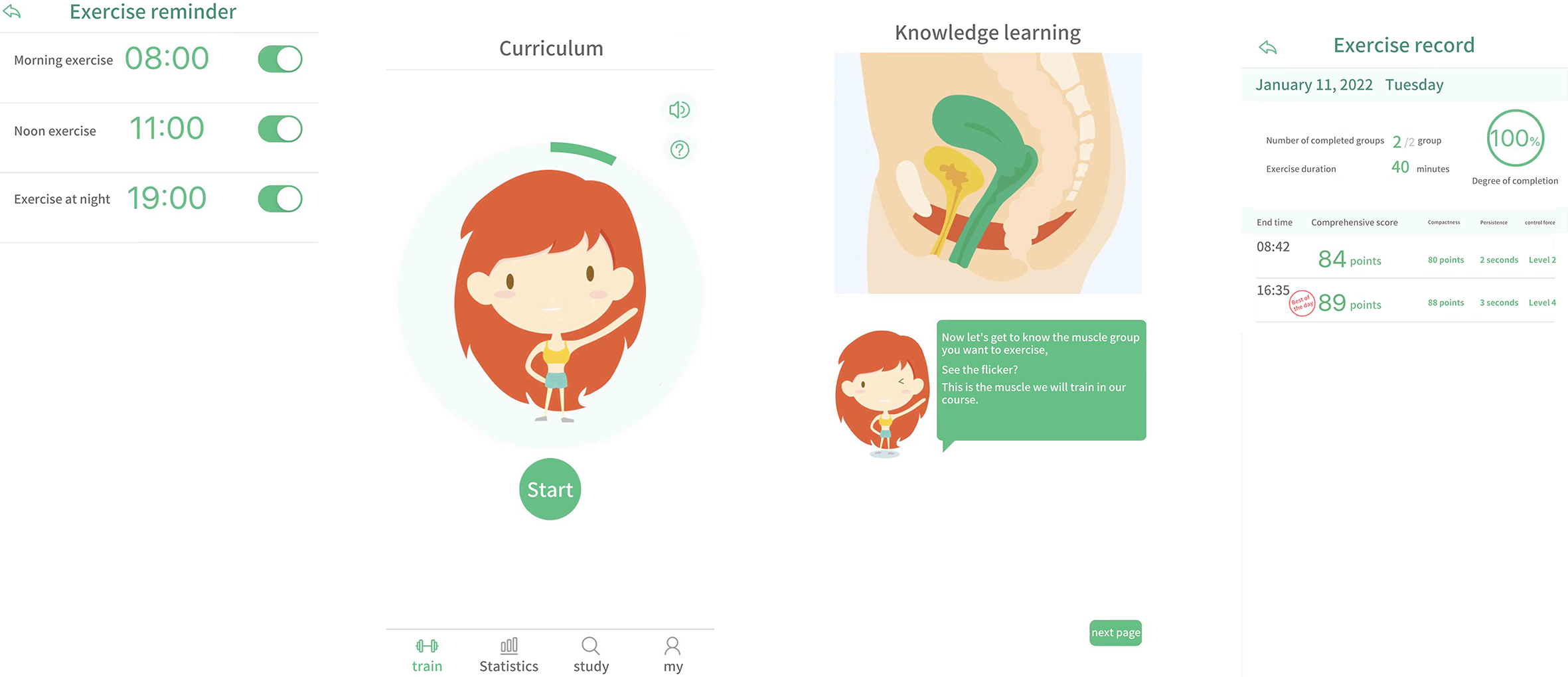
The SPSS 26.0 software was used for statistical analysis. If the measurement data were normally distributed, they were described by the mean
Results
Comparison of general data between the two groups
First, we analyzed and compared the general data of the patients. A total of 209 patients were included in this study (over 60 years old patient group: 158; 50–60 year old patient group: 51). There was no significant difference between the two groups in age, Body Mass Index (BMI), mode of delivery, ICI-Q-SF score and other factors (
General data of the research subjects over 60 years old group
General data of the research subjects over 60 years old group
BMI, Body Mass Index.
General data of the research subjects 50–60 year old group
BMI, Body Mass Index.
Comparison of different indexes in different treatment periods in over 60 years old group
Before the intervention, there was no significant difference in the knowledge awareness rate between the experimental group and the control group (
Comparison of different indexes in different treatment periods in 50–60 year old group
Comparison of different indexes in different treatment periods in 50–60 year old group
SUI is more common in postmenopausal women and elderly women, mainly caused by pelvic floor tissue relaxation. The main causes of pelvic floor tissue relaxation are pregnancy and vaginal delivery injury, and the decrease of estrogen level after menopause. In addition, age, pelvic organ prolapse, obesity, genetics and other factors may also cause SUI [15]. The treatment of SUI can be divided into conservative treatment and surgical treatment. Behavioral therapy and pelvic floor rehabilitation are the first choice for the initial treatment of urinary incontinence. The literature on treatment of SUI is summarized in Table 5.
Literature summary
Literature summary
At present, the use of apps has been widely explored in the prevention of early postpartum SUI. For the first time, this innovative study combined the use of a mobile phone app with smart vaginal dumbbell training, achieving good results in elderly female patients. The results of the study showed that there was a statistically significant difference among elderly patients in the understanding of pelvic floor rehabilitation before and after the intervention (
Compliance with pelvic floor muscle training in elderly patients
The results of this study showed that the difference in compliance before and after intervention was statistically significant (
Pelvic floor muscle strength of patients
The results of pelvic floor muscle strength in this study showed that there was no significant difference in the pelvic floor muscle strength of class I and class II muscle fibres before intervention and at the 7th week of intervention (
Quality of life of patients
The results of this study showed that in terms of quality of life, the pairwise comparison of the quality-of-life total scores at different time points indicated there was no significant difference between the two groups at 7 weeks (
Based on the findings of this study, the use of the smart app improves the knowledge and awareness of elderly female patients with SUI, improves the compliance and clinical efficacy of pelvic floor rehabilitation training, and we speculate that artificial intelligence (AI) may also have a positive effect on the treatment of patients. A large number of studies have found that AI is of great help in the treatment of human diseases, such as urinary tract infection, pulmonary emphysema, prostate cancer, neonatal sepsis [23, 24, 25, 26]. Therefore, AI intelligent therapy will be the direction of our future efforts.
Limitations
However, at this stage, intelligent applications and vaginal dumbbells still have many functions to be improved, such as real-time information exchange, pelvic floor related Q & A and other functions related to the hospital information system to realize information sharing. It is necessary to conduct a controlled trial design to further verify the impact of the smart app based intelligent continuous rehabilitation model intervention on elderly women with SUI. It is also important to extend the follow-up time to observe the long-term efficacy. And the sample size of this study is small, and the age range is 61–65 years old, so it is impossible to divide into different subgroups for comparison. In the follow-up study, the sample size and age range will be expanded and the age will be divided into different subgroups for comparison.
Conclusion
This study built an intelligent, continuous rehabilitation model based on the smart app, which included knowledge lectures, regular exercise reminders, personalised training courses, automatic exercise data generation, queries and statistics. Use of this model helped improve patient compliance with pelvic floor muscle rehabilitation. The use of the smart app improved knowledge and awareness among elderly female patients with SUI and also improved the compliance of pelvic floor rehabilitation training. Future use of this app can consolidate and strengthen the clinical efficacy of urinary incontinence treatment and play a positive role in maintaining pelvic floor muscle function, improving the long-term treatment effect of SUI.
Ethics statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Peking University International Hospital (approval number: 2021-046 (BMR)).
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Competing interests
None of the authors have any personal, financial, commercial, or academic conflicts of interest.
Funding
Not applicable.
Author contributions
Mao WJ and Jiang MZ conceived the study, Chen WD participated in its design and coordination, and Du J and Xiao Q helped draft the manuscript. All authors read and approved the final manuscript.
Footnotes
Acknowledgments
Not applicable.