
Abstract
BACKGROUND:
Macular retinoschisis in patients with high myopia is one of the main reasons for a decline in visual function and the perceived deformation of visual objects.
OBJECTIVE:
This study aimed to investigate the therapeutic effect of cataract phacoemulsification and foldable intraocular lens implantation (FILI) combined with internal limiting membrane stripping (ILMS) in the treatment of macular retinoschisis in patients with high myopia.
METHODS:
A total of 52 patients (55 eyes) who had been diagnosed with macular retinoschisis with high myopia between June 2019 and June 2020 were enrolled in the present study. Patients in the control group (25 eyes) received 23G vitreous surgery and macular ILMS and long-term inert gas (C3F8) filling of the vitreous cavity; patients in the research group (30 eyes) were additionally treated with cataract phacoemulsification and soft intraocular lens on the same treatment basis as the control group.
RESULTS:
The difference in average BCVA between the control and the research groups was not statistically significant before the surgery (
CONCLUSION:
Cataract phacoemulsification and FILI further improved the therapeutic effect of ILMS in the treatment of macular retinoschisis in patients with high myopia.
Keywords
Introduction
Macular retinoschisis in patients with high myopia is one of the main reasons for a decline in visual function and the perceived deformation of visual objects [1, 2]. Vitrectomy, combined with internal limiting membrane stripping (ILMS), has been widely used as a treatment method for this disease and has a degree of effect on the recovery of macular retinal structure and improving the patient’s visual acuity [3, 4]. Cataracts appear earlier and progress more rapidly in patients with high myopia. Clinically, however, cataracts tend to occur early in patients with high myopia and macular retinoschisis due to the particular ocular anatomical structure, and the disease is complicated with cataracts of different severities.
In the past, cataract extraction had been considered difficult and risky due to the presence of macular retinoschisis, obvious retinal atrophy, macular structural disorder, and poor visual function in patients with high myopia, making such a procedure of little significance in terms of treatment. Although the visual acuity of patients after vitrectomy combined with ILMS had to some extent been improved, the severity of cataracts following surgery was often aggravated, resulting in a decline in visual acuity without an obvious long-term therapeutic effect. Furthermore, the refractive state of high myopia is not improved after surgery, resulting in a reduced quality of life. Vitrectomy has been reported to be effective in treating macular splits [1]. However, vitrectomy can also lead to serious complications [2]. In addition, patients with macular splits may have relatively stable visual function and macular structure for a long time, and macular splits also spontaneously subsided [3]. These results suggest that vitrectomy may not necessarily be beneficial or necessary for MTM patients. Some scholars believe that cataract surgery may effectively improve visual function despite macular splits [4]. Some researchers believe that macular splitting is aggravated after cataract surgery [5], while others believe that cataract extraction improves visual function despite increased fovea thickness after surgery [6]. However, these studies included a small number of patients with limited follow-up time.
The present study investigated the therapeutic efficacy and safety of vitrectomy with ILMS and cataract phacoemulsification and foldable intraocular lens implantation (FILI) for macular retinoschisis in patients with high myopia. The aim of doing so was to establish possible treatment methods to improve the recovery of the patient’s postoperative visual function.
Data and method
General data
The clinical data of 52 patients (55 eyes) who had been diagnosed with macular retinoschisis with high myopia and underwent surgery in the Department of Ophthalmology of the Affiliated Eye Hospital of Nanchang University between June 2019 and June 2020 were included in the present study. Based on whether the patient decided to combine cataract phacoemulsification and FILI during the surgery (this information was obtained through prior communication with the patients, based on their condition), the patients were divided into two groups, i.e., the vitrectomy-only (control) group, and the cataract phacoemulsification (research) group.
The control group comprised 24 patients (25 eyes); there were 10 male cases with 10 diseased eyes and 14 female cases with 15 diseased eyes (all aged 30–58 years old; average age, 46.23
Both patient groups completed various preoperative examinations, including tests concerning naked eye vision, best-corrected vision, intraocular pressure, slit lamp examination, fundus examination under a digital wide-field lens, A/B ultrasonography of both eyes, fundus color photography, frequency-domain optical coherence tomography (OCT), and intraocular lens (IOL) master and corneal endothelium detection. An A-mode ultrasound was adopted to measure the anteroposterior diameter of the eyeball; OCT was adopted to accurately measure the thickness of the retinal nerve fiber layer, and the Zeiss IOL Master
In the control group, 4 eyes had grade I cataracts, 15 eyes had grade II cataracts, and 6 eyes had grade III cataracts. In the research group, 5 eyes had grade I cataracts, 18 eyes had grade II cataracts, and 7 eyes had grade III cataracts. The naked eye visual acuity of both groups was
The study’s inclusion criteria were: (1) patients with high myopia and a diopter ranging from
The study’s exclusion criteria were: (1) patients with ocular complications associated with systemic diseases; (2) patients with a history of eye surgery that had had an impact on their vision; (3) patients with high myopia complicated with retinal detachment, macular hole, anterior macular membrane, macular neovascularization, and/or other retinal diseases and who had previously received retinal laser photocoagulation; (4) patients with a history of glaucoma, congenital cataract, chronic uveitis, corneal degeneration, and keratitis.
The selection and calculation of the artificial IOL degree proceeded as follows: Alcon single focal artificial IOL was adopted using a hydrophobic acrylate material. The corneal curvature was measured by the computer automatic refractometer, the axial length was measured by the A/B ultrasound, and the corneal curvature and axial length were measured using the IOL Master. Measurement values with high repeatability were selected; the built-in software of the IOL Master was used to calculate the degree of artificial IOL power according to the SRK-T formula, and the larger values of the results were selected. The range was pre-set to
Methods
All the patients were given antibiotic eye drops before the surgery, and the pupils were fully dilated. The patients in the control group were treated with vitrectomy and 23G pars plana three-port vitrectomy and macular ILMS using the RESIGHTTM wide-angle fundus observation system. The posterior vitreous cortex was fully removed during the operation, and a 0.1 ml mixture of brilliant blue and 50% glucose was injected into the vitreous cavity to stain the internal limiting membrane of the retina. Once the internal limiting membrane was fully stained, 23 G internal limiting membrane forceps were used to continuously strip the internal limiting membrane in the macular area; the scope of stripping reached the vascular arch in the macular region. The retina was then fully inspected to ensure that no retinal detachment and/or retinal hemorrhage had occurred. Gas-liquid exchange was performed by injecting long-term gas (C3F8) into the vitreous cavity.
Patients in the research group underwent cataract phacoemulsification and FILI before vitrectomy. Soft, foldable artificial intraocular lenses were adopted in this procedure, and the intraoperative corneal incision was 2 mm. The American Alconconstellation vision SYSTEM was used for phacoemulsification and vitrectomy. All artificial intraocular lenses were successfully implanted in the research group; the remaining surgical procedures were the same as in the control group. All operations were performed by one experienced doctor. No complications, such as retinal detachment, macular hole, and fundus hemorrhage, occurred in either group during the surgery. There was also no occurrence of lens capsule rupture or lens position displacement in the research group. The patients were followed up for 6–12 months after the procedure, and the treatment effect was determined by the final follow-up results.
After the surgery, the indicators (e.g., naked-eye vision recovery, best corrected visual acuity [BCVA], intraocular pressure, diopter, axial length, and retinoschisis) and complications (e.g., retinal detachment, macular hole, fundus hemorrhage, posterior cataract in the crystalline lens, artificial intraocular lens position changes, structural changes of macular nerve fibers, fundus retinal changes, and corneal endothelial changes) were observed. For the convenience of statistics, the decimal BCVA values were converted into LogMAR vision values.
Evaluation criteria
The OCT evaluation criteria for postoperative macular morphology were as follows: (1) the anatomical reduction was considered successful when the retinoschisis cavity disappeared after surgery, and the retina was completely reattached without retinal detachment and the occurrence of a macular hole; (2) retinal reattachment improvement was considered successful when the macular retinoschisis cavity became smaller and the thickness of the retinal nerve fiber layer in the macular region decreased but did not completely disappear after surgery; (3) the result was considered unsuccessful when the retinoschisis cavity did not disappear after the operation, without obvious changes compared with before the surgery.
The change in diopter in the control group was considered the difference between the diopter before and after the surgery, and the change in diopter in the research group was taken as the difference between the intraoperative residual diopter and postoperative diopter.
Statistics analysis
The data were statistically analyzed using the SPSS Statistics 22.0 software. The measurement data were expressed as mean
Results
Comparison of basic preoperative conditions
A total of 52 patients (55 eyes) who received treatment at the Eye Hospital Affiliated with Nanchang University were enrolled in the present study. The axial length, diopter, BCVA, MFT intraocular pressure, corneal endothelial count, corneal endothelial hexagonal cell ratio, coefficient of variation, and cataract grade of all patients were statistically measured and compared between the two groups before the surgery (Table 1); the differences between the two groups were not statistically significant.
Comparison of basic conditions between the control group and research group before the operation
Comparison of basic conditions between the control group and research group before the operation
The axial lengths in the two groups at the final follow-up (12 months after the surgery) were measured. The average axial lengths in the control and research groups were 29.83
The postoperative diopter in the control group was
Best corrected visual acuity
A comparison of the BCVA between the two groups is shown in Table 2. The differences in BCVA among time points (before the surgery and 1 and 3 months after the procedure) were not statistically significant (
Comparison of CMT and BCVA between the control group and the research group at time points of before and after operation
Comparison of CMT and BCVA between the control group and the research group at time points of before and after operation
The macular OCT in the two groups before the surgery revealed different degrees of separation in the macular nerve fiber layer, with separation between various layers. Most of the outer layers had split off; this was sometimes accompanied by the simultaneous splitting of the inner and outer layers, with or without localized serous detachment of the macula. The postoperative OCT revealed that the macular nerve fiber layer splitting had closed and the cyst cavity had disappeared (Fig. 1).
In the control group, macular retinal retinoschisis disappeared in 17 eyes, the retina improved in 6 eyes, and the conditions remained unchanged in 2 eyes. In the research group, macular retinal retinoschisis disappeared in 20 eyes, the retina improved in 8 eyes, and the conditions remained unchanged in 2 eyes.
Both patient groups underwent macular OCT at 1, 3, 6, and 12 months after the surgery. The central macular thickness (CMT) gradually decreased at 1, 3, 6, and 12 months after the operation; when compared with the CMT before the surgery, the difference was statistically significant (
Changes in the cornea and corneal endothelium
There was no corneal edema in the control group during or after the surgery. A total of 4 eyes in the research group had mild corneal edema after the operation; this subsequently disappeared, and transparency was restored within 1 week of taking medication. None of the patients experienced severe corneal complications. The corneal endothelia of the two groups at the end of the follow-up period are shown in Table 3.
Indicators of corneal endothelium at 12 months after operation
Indicators of corneal endothelium at 12 months after operation
Change of CMT in one eye in the research group. A: Before operation; B: 3 months after operation; C: 6 months after operation; D: 12 months after operation.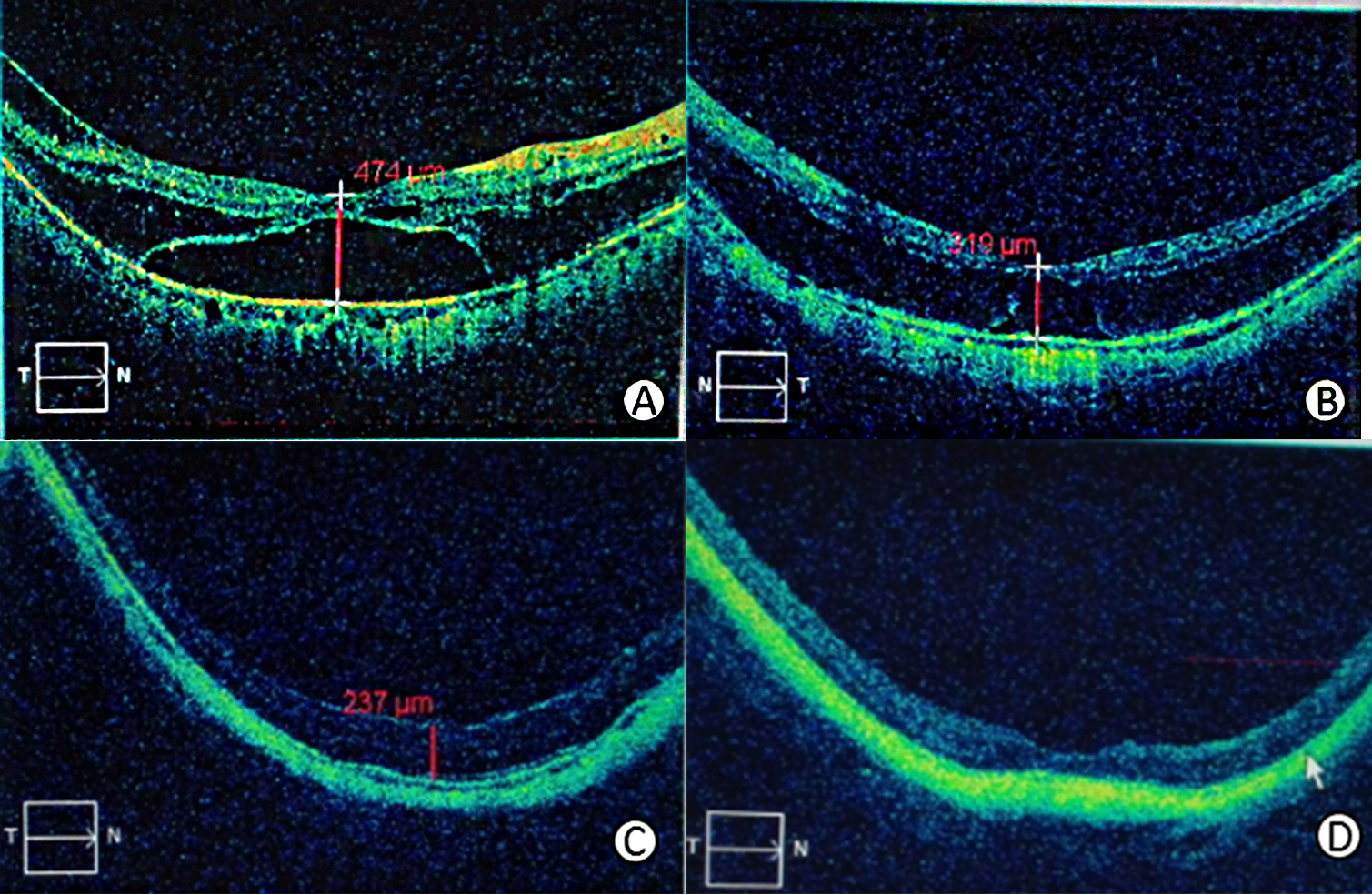
During the surgery, no retinal detachment or retinal hole was found after ILMS in the control or the research group, respectively. During the ILMS process, 3 eyes in the control group and 4 eyes in the research group had punctate hemorrhagic spots around the macular area; however, the bleeding stopped under low-energy laser photocoagulation. Postoperative intraocular pressure increased in 5 eyes in the control group and 6 eyes in the research group; the pressure was
In the control group, the degree of lens opacity was aggravated to different degrees before and after the surgery. Among these, a total of 10 eyes developed panba-like turbidity at the posterior capsule; in 15 eyes, the color of the lens cortex and nucleus deepened, and in the case of 15 eyes, the patients were admitted for cataract extraction. In the research group, there was no dislocation or obvious displacement of the intraocular lens during the follow-up period. A total of 16 eyes had different degrees of posterior capsular opacity, which was eliminated using a yttrium aluminum garnet (YAG) laser. No macular hole, retinal detachment, macular neovascularization, or other complications occurred in either of the groups.
Discussion
Retinoschisis in patients with high myopia is a complication that affects ocular fundus lesions; it is often accompanied by posterior pole scleral staphyloma and progressive axial lengthening, as well as degenerative changes in the retina and choroid. Retinoschisis mostly occurs in the nerve fiber layer or outer plexiform layer and affects visual signal transmission. When retinoschisis involves the macula, central vision is severely affected [10, 11]. At present, many domestic and overseas experts believe that in patients with high myopic macular retinoschisis and persistent visual loss, vitrectomy combined with ILMS will have a certain effect on controlling the progress of retinoschisis, preventing the occurrence of complications (e.g., macular hole and retinal detachment caused by macular retinoschisis), and improving the prognosis of high myopia.
The internal limiting membrane is considered an important cause of macular retinoschisis. The residual cortex after vitrectomy and the continuous traction of the internal limiting membrane by collagen fibers on the membrane’s surface are possible reasons for the occurrence of macular retinoschisis [12, 13]. Releasing the traction effect of the internal limiting membrane is conducive to the restoration of the retinoschisis cavity.
In the present study, the authors used brilliant blue to stain the internal limiting membrane of the retina and a 23G minimally invasive vitrectomy system to completely strip the internal limiting membrane. The study results revealed that the degree of retinoschisis after the surgery had been significantly reduced in the control and research groups compared with before the procedure.
In the control group, 68% of diseased eyes achieved anatomical reduction and 24% achieved retinoschisis improvement; in the research group, 66.6% of the diseased eyes achieved anatomical reduction and 26.6% achieved retinoschisis improvement. At 1, 3, and 6 months after the surgery, the thickness of the macular retina gradually decreased; there was no significant difference in the thickness between 6 and 12 months after the surgery (
A complicated cataract is a common complication of high myopia. The condition causes severe vision loss and has a significant impact on the patient’s life. In the past, patients with high myopia and macular retinoschisis cataracts could only undergo surgery when the cataract opacity affected the surgical procedure during the ILMS process. In most cases, cataract extraction was not performed, as the ocular fundus could only be narrowly observed. However, the occurrence of postoperative cataract complications seriously affected the patients’ vision and some even had to undergo repeat cataract surgery.
Packer et al. [14] reported a post-vitrectomy nuclear cataract incidence as high as 80%. Cherfan et al. [15] observed 100 patients with an epimacular membrane in one eye who underwent vitrectomy and ILMS; the lens of 96 (out of 97 operated-on eyes) contralateral eyes was transparent before the surgery. At 24-month follow-up, the rates of nuclear sclerosis in the operated-on and non-operated-on eyes were 68.4% and 12.8%, respectively.
Phacoemulsification extraction combined with intraocular lens implantation has significant advantages, such as a smaller surgical incision and less tissue damage, a shorter surgery time, faster postoperative incision healing and visual recovery, and fewer complications.
Gu et al. [16] compared the respective postoperative effects of small incision extracapsular extraction and phacoemulsification in patients with high myopia. The results revealed that phacoemulsification was conducive to vision improvement in the treatment of high myopia complicated with a cataract. It also had the advantage of fewer postoperative complications, making it a safe and reliable method for this condition.
In the present study, the patients in both groups had different grades of cataracts before the surgery; the difference between the two groups was not statistically significant (
During the postoperative follow-up, the degree of eye opacity in patients affected by nuclear cataracts was significantly aggravated in the control group, and there was a statistically significant difference when compared with the opacity before surgery (
Corneal endothelial cells in patients with high myopia are prone to morphological changes leading to the decline of corneal endothelial function. In the process of phacoemulsification, a degree of damage will inevitably be done to corneal endothelial cells, the number of cells will decrease, and the function of endothelial cells will decline. Corneal edema, bullous keratopathy, and even blindness may occur after the surgery.
In this study, a comparison of corneal endothelial cell density, the percentage of hexagonal cells, and the coefficient of variation between the two groups before and after surgery revealed that in the research group, the number of corneal endothelial cells and the percentage of hexagonal cells at 12 months after surgery had decreased compared with the number and percentage before surgery; the differences were statistically significant (
In the research group, 8 eyes had mild corneal edema after the operation; after 1 week of drug treatment, the corneal edema was resolved, and corneal transparency was restored. No recurrence of corneal edema, corneal degeneration, or bullous keratopathy occurred during the follow-up period. Based on these results, it was concluded that cataract phacoemulsification effected a degree of damage to the cornea. The possibility of corneal complications via the compensatory function of corneal endothelial cells was considered to be low.
The postoperative recovery of visual acuity of retinoschisis in patients with high myopia was found to be related to specific factors, such as preoperative BCVA, axial length, postoperative continuity, or the absence of an ellipsoid band, and retinal reattachment. The difference in BCVA before and after surgery was not statistically significant. While no significant difference in BCVA was observed at 1 and 3 months after the surgery, the BCVA at 6 and 12 months after the procedure was better in the research than in the control group, and the difference was statistically significant (
The slit-lamp examination revealed that in the control group, lens opacity had been significantly aggravated after surgery, and the color of the nuclei of most lenses had deepened, affecting patients’ vision. After FILI, the refractive medium in the control group remained transparent. Some patients had their condition complicated with a posterior cataract; after YAG laser opacification and post-capsulectomy, the visual acuity was restored. In terms of naked eye vision, the patients in the control group still had to wear super-high frame glasses for correction after surgery because no refractive correction had been performed on the affected eye. In the research group, the patients’ dependence on frame glasses was reduced, and their quality of life was improved following the correction of the refractive state.
From a long-term perspective, postoperative complicated cataracts are inevitable and will have a serious impact on patients’ postoperative vision. Furthermore, due to the characteristics of patients with high myopia and a cataract with a long axial length, thin sclera, and large suspensory ligament fragility [17], as well as a vitreous cavity filled with water, some patients in the control group had to undergo repeated cataract extraction and, as a result, also faced increased surgical risk [18, 19].
There is an increase in the number of patients with high myopia and macular retinoschisis, and controversies regarding the treatment of macular retinoschisis in high myopia, which has an unsatisfactory effect. The surgical outcome of vitrectomy is not ideal for patients with high myopia and macular retinoschisis caused by factors that include posterior scleral staphyloma, retinal choroidal atrophy, long axial length, and pigment epithelial defects [19, 20, 21]. However, vitrectomy combined with ILMS remains an important method for the treatment of retinoschisis in patients with high myopia [22, 23, 24, 25].
Conclusion
In this study, cataract phacoemulsification and FILI, combined with vitrectomy and ILMS, had a degree of effect on patients with high myopia and macular retinoschisis; it prevented the continuous development of retinoschisis, reduced further damage to visual function, and caused no obvious postoperative complications. Thus, it can be considered a safe and feasible surgical method. However, the number of cases observed in the present study was limited; a large-sample, multicenter, long-term comparative study is required for further observation.
Footnotes
Conflict of interest
The authors have no conflict of interest to declare.