
Abstract
BACKGROUND:
The Selfit system was developed to improve the mobility and gait-related functions of stroke patients by providing digital exercises and augmented reality training system.
OBJECTIVE:
To evaluate the effects of a digital exercise and augmented reality training system on mobility, gait-related functions and self-efficacy outcomes in stroke patients.
METHODS:
A randomized control trial was conducted on 25 men and women diagnosed with an early sub-acute stroke. Patients were randomly assigned to either the intervention (
RESULTS:
The intervention group practiced proportionally more time per session than the control group with a mean change of 19.7% following 6 sessions (
CONCLUSION:
The findings suggest that Selfit holds promise as an effective intervention for improving mobility and gait-related functions among patients with an early sub-acute stroke as compared to conventional physical therapy treatments.
Introduction
Stroke is a leading cause of mortality and morbidity worldwide [1]. The majority of stroke survivors experience motor function impairment with reduced mobility and altered gait [2, 3]. Gait adaptability, the ability to adapt gait to various surfaces and situations is an important aspect of the functional recovery of gait [4, 5, 6, 7]. Additionally, both the static and dynamic balance, which affect gait of survivors, are also often negatively affected by stroke, which increases the incidence of falls among these patients [8].
One approach to balance training is task-oriented training, whereby the patient repeats functional movements required for daily living. There is evidence that focusing on repeated functional tasks improves motor functions [9] as a result of neuroplastic changes, which are crucial for functional recovery of normal gait [10, 11, 12]. A previous study has shown better results for gait or gait-related functions of stroke patients with the application of task-oriented training, rather than simply increasing the movement of hemiplegic limbs [13].
The Selfit system was developed to improve the mobility and gait-related functions of stroke patients by providing digital exercises and augmented reality training system. Most technology-supported approaches, including virtual reality (VR) [14], exergaming, and robotics are geared toward the activity domain. These approaches present structured and systematic methods for the implementation of task-specific practice concepts [15]. However, it is unclear whether VR mobility training is more effective than other interventions for stroke patients in terms of comfort and maximum walking speed, spatiotemporal gait parameters, and walking ability (
The primary objective of the study was to determine the effects of the Selfit system, using digital exercises and Augmented Reality AR program on mobility, gait-related functions, and self-efficacy outcomes for patients with an early sub-acute stroke. The secondary objective of this study was to assess the satisfaction and feasibility of the Selfit system in the management of patients with an early sub-acute stroke and their therapists.
Methods
The study was approved by the institutional review board of Tel Aviv Sourasky Medical Center, Ichilov Hospital, Israel, and by the Israeli Ministry of Health (Approval number: 0527-17-TLV, 20185430). Consent forms were obtained from all participants. The study was registered with the US National Institutes of Health Clinical Trials Registry ClinicalTrials.gov (Identifier: NCT03671876).
Study participants were men and women diagnosed with an early subacute stroke.
The timeline defines 7 days to 3 months as the early subacute phase and 3 to 6 months as the late subacute phase post stroke. This time represents an important treatment target to maximize the potential of restorative interventions [16].
Trial design
A randomized control trial was conducted at the rehabilitation department of Tel Aviv Sourasky Medical Center between September 2018 and January 2019. The intervention group included patients whose treatment plans included both conventional and Selfit treatment sessions as part of their inpatient physiotherapy rehabilitation program. The control group included participants whose inpatient rehabilitation treatment plan consisted only of conventional treatment sessions. The number of treatment sessions were identical for all study participants: 15 physiotherapy sessions that were 30 minutes long. The intervention group received a total of 15 sessions, nine conventional treatment sessions and six Selfit treatment sessions. The control group received 15 conventional sessions.
Randomization
Prior to the recruitment process, a randomization list of 33 numbers was generated using the randomization command in Microsoft Excel
Blinding
The research team members responsible for the statistical analyses were blinded to the type of intervention.
Participants
The hospital’s rehabilitation department carried out the recruitment process.
All study participants were patients of the department of rehabilitation of Tel Aviv Medical Center, and diagnosed with an early subacute stroke, capable of walking independently or with minimal help for a distance of at least 10-meters (Functional Independence Measure [FIM] motor score
The Selfit system
The Selfit system is composed of Hardware and Software components. The Hardware (HW) part consists of a projector, camera, and a processing unit – computer (
The Selfit system was developed to improve the mobility of stroke patients by providing digital exercises and Augmented Reality (Fig. 1). Digital exercise is exercise that utilizes digital tools, such as websites, smartphone applications, messaging platforms, video, audio, games or AR/VR interactions. Augmented reality technology integrates digital information, content, and virtual objects into the patient’s real-world environment in real-time. This technology offers the patients an engaging and immersive method of rehabilitation, allowing a safe environment for patients to exercises. The Selfit system is comprised of a projector (Optoma TX565UT-3D) that projects the exercises on the floor and a motion camera, which collects the persons performance data (Microsoft’s Kinect 2). A laptop computer operates the integration between the projector and the camera (ASUS Vivobook X556UQ).
The Selfit system.
The Selfit program is comprised of exercises that focus on several important aspects of rehabilitation among stroke patients, such as gait, mobility, balance, speed, cadence, range of motion, and dual-tasking.
The person-machine interaction is based on audio and visual cues, providing instructions and feedback to the participant, and has the potential to improve mobility and self-efficacy in early subacute stroke patients. Using a safe augmented reality and real-life interaction, the Selfit system projects structured exercises onto the floor in front of the patient and a motion camera collects participant performance data and analyzes the data to gain insight regarding progress. The Selfit system is equipped with a projector and a motion camera to generate AR rehabilitation exercises on the floor just in front of the patient. The content could be 2D or 3D, with 3D providing an immersive and more realistic training that resembles the real world. For note, using the Selfit system, there is no need to wear glasses or headsets, which may be a barrier to adoption of the technology especially in patients with disabilities.
Leveraging augmented reality projection enables an immersive rehabilitation experience, which could positively affect the participant’s level of engagement and motivation and lead to improved outcomes. The Selfit exercise system is a scalable, structured, digitized version of conventional exercises. Compared to other digital therapy solutions, which typically utilize a smartphone for the therapy interaction, the Selfit system uses a bigger and more visible screen for the interactions. This difference could potentially impact patient outcomes when treating stroke patients, as well as older adults with common visual impairments.
An additional innovative application of the Selfit system is the use of motion sensors during the therapy session to provide better profiling of participant’s progress. This can lead to improved individualized treatment, and ultimately, better outcomes. The use of the system’s audio and visual cues to provide instructions and feedback to the participant, along with the digitization and automation of various aspects of the rehabilitation process, could pave the way for more advanced self-care interactions in the institutional and home settings.
A one-stage screening process was performed to identify potential participants followed by the initial contact with the stroke patient by the research team. All data were anonymized and maintained on a secure server.
Control group
Patients in the control group were treated only with the standard physical therapy treatment. The control group treatment included a conventional physical therapy program, including strength, range of motion, balance, dual tasking exercises and gait training.
Intervention group
In the intervention group, patients received 9 standard-care conventional therapy sessions plus 6 sessions with the Selfit system.
Participants in the intervention group were briefly instructed about the intervention prior to beginning their treatment plans. A physical therapist was assigned to each participant in the intervention group and provided support and physical assistance when needed.
The exercises used during the study were digital versions of exercises used during a conventional rehabilitation program for stroke patients. In the event that a specific exercise was too simple or too challenging, participants had the option of skipping an exercise and move forward to the next one.
A total of 12 exercises were assigned to each participant in the intervention group. The selected exercises were focused on gait, speed, cadence, balance, coordination, and dual tasking. Each exercise was preceded by a short explanatory recording in the language of the participants delivered by the Selfit system. Once the participant completed the exercise, a feedback text was projected onto the floor evaluating their performance (number of errors, speed, etc.). The participant then had the option to click the “Replay” button on the floor to repeat the exercise or click “Next” and proceed to the following exercise.
Selfit exercises projected onto the floor. Twelve mobility exercises with different combinations of visual elements such as foot marks, lines, and squares, represented by numbers from one to twelve.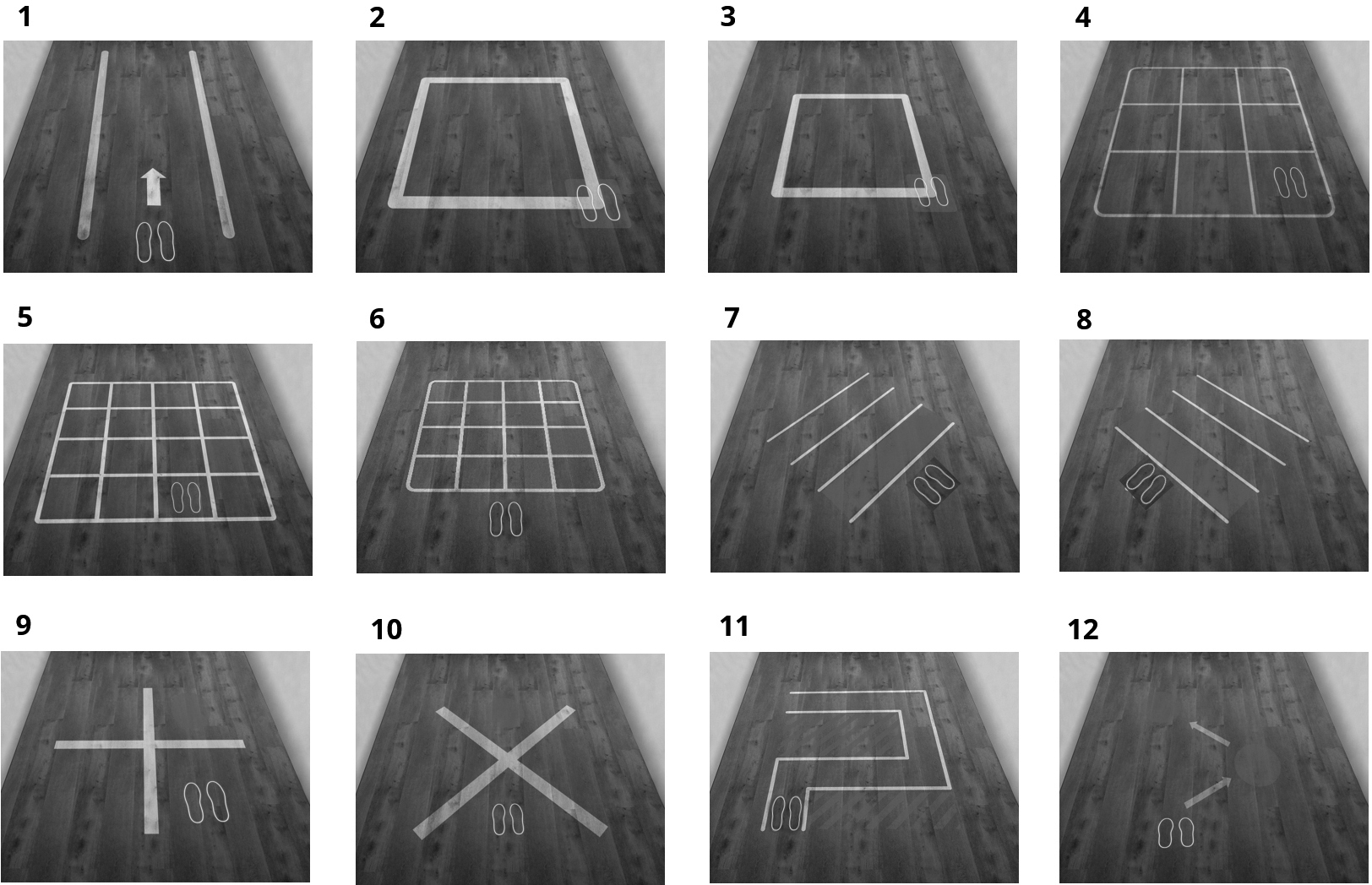
Twelve exercises per session were assigned for each participant (Fig. 2): Exercise 1 – walk directly between two lines; Exercise 2 – walk on the square, facing forward; Exercise 3 – walk on a smaller sized square, facing forward; Exercise 4 – step to the marked cue upon a 3x3 board; Exercise 5 – step on the marked cue upon a 4x4 board; Exercise 6 – memorize the path of the marked signs and follow it; Exercise 7 – cross over the lines (left side version); Exercise 8 – cross over the lines (right side version); Exercise 9 – cross over the straight lines according to the marked signs while facing forward; Exercise 10 – cross over the diagonal lines, according to the marked signs while facing forward; Exercise 11 – walk the path. Exercise 12 – walk from one target to another.
Data collection
Outcome measures, timed up and go (TUG), dynamic gait index (DGI), the 0-meter walk test and activities-specific balance confidence (ABC) survey were collected before and after the intervention. Participant and therapist were asked to complete the Suitability Evaluation Questionnaire (SEQ) to assess feasibility and engagement post-intervention.
Independent measures
Demographic data, including age, sex, height, weight, and length of hospitalization was collected from participants’ medical record.
Activity-based outcomes
Activity-based outcomes were measured to investigate different parameters of movement in a therapy session including mobility and gait-related functions for both groups. These parameters included: session duration, movement duration, rest time, step count and step per second.
Session duration was measured from the beginning to the end of the therapy session with the Selfit system. Movement duration was defined as the patient’s movement time during a therapy session with the Selfit system. Rest time was defined as session duration minus movement time. Step count was calculated as the number of steps within the therapy session with the Selfit system. Steps per second was calculated as the number of steps per second during the session.
The activity-based outcomes for the intervention group were collected using the Kinect 2 camera (part of the Selfit system), while the activity-based outcomes for the control group were collected using Apple’s iPhone 7 native counter app.
Mobility outcome measures
The TUG is a validated, widely-used functional physical task for measuring lower extremity function, mobility, and balance [17]. The DGI is a clinical tool used to assess a person’s gait, balance, and risk of falling, as well as evaluating walking patterns during a person’s normal steady state, and walking patterns during more challenging tasks [2]. The 10-meter Walk Test was used to determine functional mobility, gait, and vestibular function, evaluating walking speed over a short distance [18].
Self-efficacy outcomes
Self-efficacy outcomes were assessed using the ABC Scale, a validated and widely-used structured survey that measures an individual’s confidence in their ability to perform activities without losing their balance [19].
Feasibility and satisfaction measure
Participants in the intervention group and therapists were asked to complete the SEQ to assess overall feasibility and satisfaction. The SEQ consists of 11 questions graded on a 5-point Likert scale. Lower scores reflected positive feedback for the intervention, while higher scores reflected negative feedback.
Data analysis and statistical methods
R software version 4.0.0 was used for statistical analysis, using library nlme version 3.1–147. Descriptive statistics were performed for the participants’ demographic and clinical characteristics. Mean and standard deviations were reported for continuous variables, and frequencies and percentages were used for categorical variables. Distribution of the variables was examined visually by density curves and quantiles plots, and statistically tested using the Shapiro-Wilk normality test.
The analysis of covariance (ANCOVA) was performed to assess the differences between the groups of TUG, ABC, DGI, and 10-meter walk test results following the intervention, with pretests as covariates. The 2 ways repeated measure ANOVA was performed to assess the differences in step count and step speed over-time between the groups. Linear mixed effects regression models were applied to compare quantitative results between the two groups while factoring in their change over time and accounting for inter-correlation factors. The models included main effects for the session and group indicators and a random intercept term. When appropriate, a fixed effect for the interaction term between session and group was added to the model.
Results
Participants’ characteristics
Thirty-three early subacute stroke patients were enrolled in this study. Among the 33 patients enrolled in the study, 8 participants did not complete the study due to an unexpected early discharge from the rehabilitation department (Fig. 3). In total 25 participants completed the study, 11 participated in the intervention group and 14 in the control group. Demographics and clinical characteristics are described in Table 1. No significant differences in demographic characteristics were observed between the groups.
Demographic and clinical characteristics of the control versus intervention groups
Demographic and clinical characteristics of the control versus intervention groups
Detailed participant flowchart.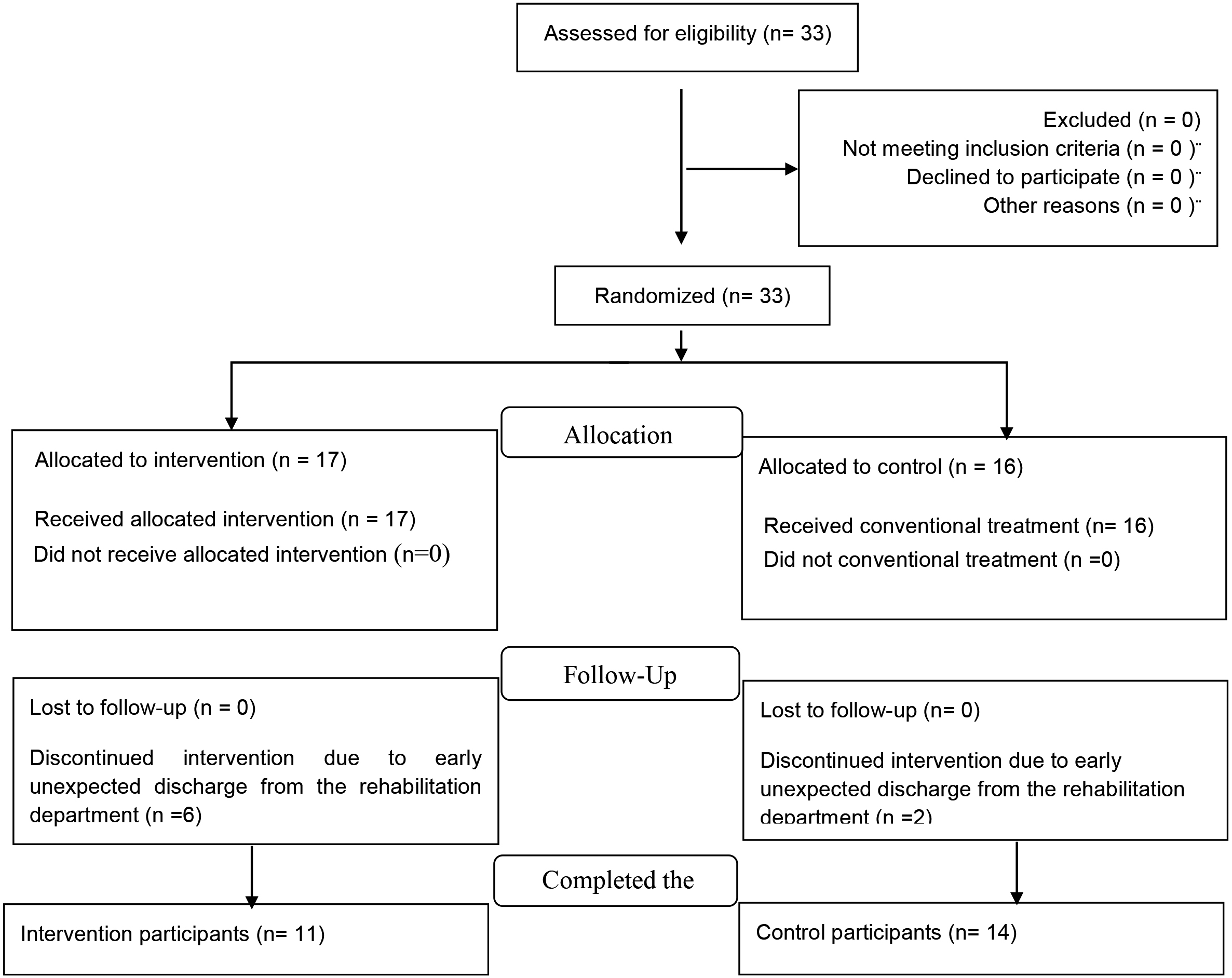
The total time preforming the session task was reduced by a mean of 10.5% in the intervention group compared to the control group (
Movement time vs. session time
The time practice of the intervention group per session (i.e., more movement time) was longer than that of the control group with a mean change of 19.7%, resulting from six sessions for each group (
Step count
The average step count increased over time for the intervention group and was significantly higher in the intervention compared to the control during the last sessions (
Steps per second
The average steps per second increased over time for the intervention group and were significantly higher in the intervention compared to the control during the last sessions (
a. Average step count of 6 sessions. A line graph plotting the average steps count of the intervention group (grey circle) and the control groups (red squares). 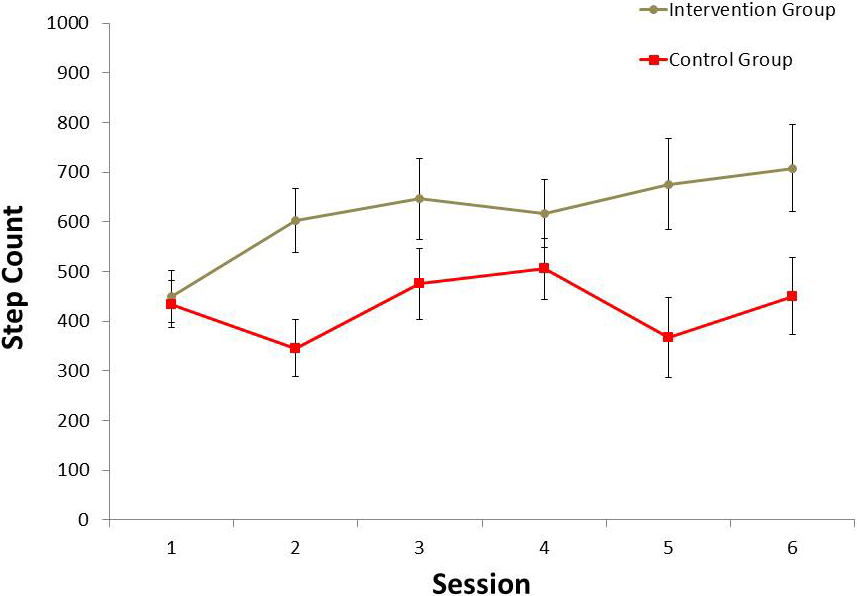
b. Average steps per second of 6 sessions. A line graph plotting the average steps per second of the intervention group (grey circle) and the control groups (red squares).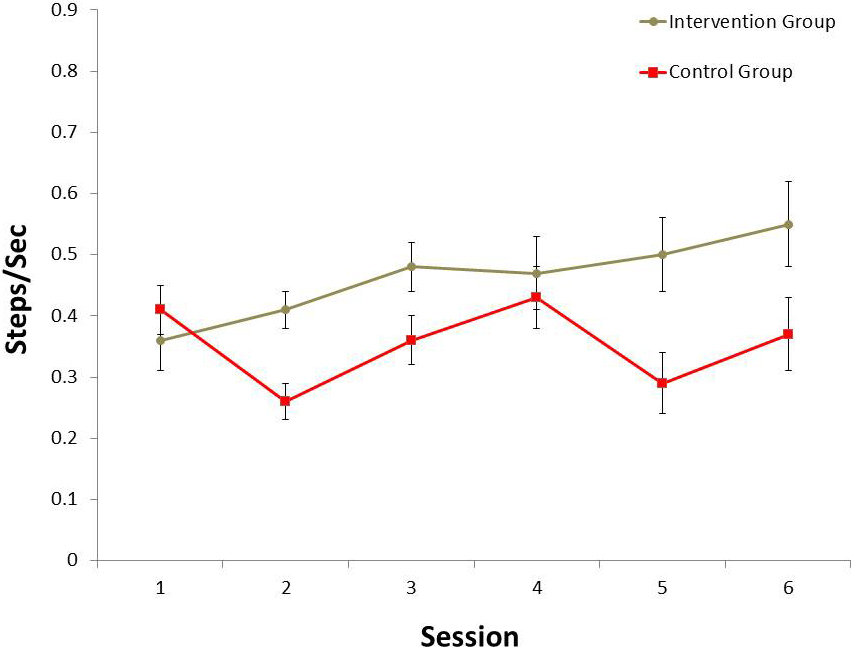
The TUG test was performed at pre- and post-intervention for both study groups. In the ANCOVA with the TUG pretest score as a covariate, post-TUG scores were better in the experimental group compared with the control group (12.43.4 vs 21.33.0,
The dynamic gait index (DGI)
The DGI test was conducted pre- and post-intervention for both groups. In the ANCOVA with the DGI pretest scores as a covariate, no significant differences were found between the intervention and control groups for post-DGI scores.
10-meter Walk test
The 10-meter Walk test was performed at pre- and post-intervention for both study groups. In the ANCOVA with the 10-meter walk pretest as a covariate, no significant differences were found between the experimental group and the control group for post-10-meter test results.
Activity specific balance confidence (ABC) scale
The ABC test was performed at pre- and post-intervention for both study groups. In the ANCOVA with the ABC pretest scores as a covariate, no significant differences were found between the control groups and the intervention group for post-test ABC scores.
Intervention feasibility and satisfaction
The average score of the SEQ per question in the intervention group was 1.99 (1 reflecting excellent feedback, 5 reflecting negative feedback). Among the therapists the average score per question was 1.65.
Discussion
Principal findings
The main purpose of this study was to investigate the potential benefit of innovative technology, the Selfit training system, on mobility and efficacy outcomes for patients with an early subacute stroke. With respect to mobility and balance, stroke patients who participated in Selfit’s intervention program demonstrated a significant improvement in TUG tests, two important assessment tests for gait and risk of falling among stroke patients. The intervention effect suggests that scalable, structured, digital exercises and an augmented reality training system, such as the Selfit training system, may be beneficial for stroke patients.
Many activities of daily living require performing more than one task at a time [20], which is known as dual-task performance. People with low cognitive or physical function experience difficulties in performing dual-task’s and are more prone to physical injuries, such as falls [21, 22]. Erickson et al. [23] reported that training in dual-task situations yields better results, such as increased cerebral blood flow, compared to training in single-task situations. It is possible that the dual-tasking exercise provided by the Selfit system may be beneficial to stroke patients.
The literature also supports visual cueing to increase stride length and walking speed for patients recovering from a stroke [24]. The use of visual cues improves walking symmetry, balance, and functional mobility during stroke rehabilitation. In a study by Hollands et al. [4] both symmetry and walking speed significantly increased among patients after only one or two sessions of visual cueing. The Selfit system provides visual cues, which have the potential to improve function and mobility in stroke patients.
In our study, however, no statistical differences between the groups were found in the 10-meter walk test and self-efficacy scale (ABC). It is possible that the intervention was too short to observe significant changes. Future studies should examine the effects of a longer intervention using the Selfit system on 10-meter walk test and self-efficacy scale.
Additionally, this study aimed to investigate the feasibility and satisfaction of the Selfit system by participants and therapists. The intervention group and their physical therapists reported good feasibility and high satisfaction with using a digital exercise and augmented reality training system as part of the rehabilitation regimen.
The results of the study also showed that the intervention group has a longer practiced time per session than the control group. This may be due to the gamified therapy approach and an increased level of engagement. Another possible explanation for the increased practice time with Selfit is the consecutive exercise sequence, which challenges the participant and encourages them to move from one task to another with little distraction from the external clinical environment in addition to the interactive real-time feedback. Furthermore, the Selfit system only had minimal logistical requirements for set-up on the part of the therapists. This aspect could also partially explain the positive feedback for the intervention reported by the therapists involved in the study.
A previous study demonstrated that patient task-oriented training compliance is low, due to the required frequency of repetitions during conventional treatment sessions [25]. In our study, the number of steps per session and the speed (step/sec) increased over time in the intervention group. It is possible that factors such as repetition, external queuing, and direct feedback have a positive effect on patient’s compliance. Variety, repetition and visual or auditory feedback are known to be essential elements for the success of the treatment of stroke patients [26]. These elements are provided by the Selfit system, suggesting that they may help stroke patients to be compliant with prescribed exercise program.
VR and augmented reality approaches for rehabilitation have several advantages, including, adaptability and variability based on patient baseline, transparent data storage, remote data access, reduced rehabilitation session costs, as well as engaging, entertaining and motivating properties [27, 28]. In addition, these technologies often allow the healthcare providers to evaluate different outcomes and analyze data [28]. Disadvantages of VR augmented reality use for rehabilitation include expensive initial cost of equipment, lack of computer skills, lack of support infrastructure, patient safety concerns, and symptoms (motion sickness, nausea, vertigo and disorientation) [28, 29, 30].
Despite the limitations, augmented reality holds promise in rehabilitation of stroke patients. The results of the study showed that the incorporation of digital exercise and augmented reality improved some aspects of rehabilitation, including mobility and gait-related functions in this patient population.
Study limitations
This study has a number of limitations. First, the study provided a relatively short intervention period, which may limit our understanding of the long-term effects of the Selfit system on early subacute stroke patients. The lack of improvement in the 10-meter walk test results may be due to the short intervention. Although patients had a higher step count in the intervention group compared to the control, there were no differences in the 10-meter walk test between the groups. It is possible that longer intervention with Selfit may yield significant improvement in the 10-meter walk test results as well. Furthermore, although both groups received the same number of sessions (a total of 15 sessions each group), we cannot exclude the possibility that the better improvement in the scores of the intervention group is due to more movement time within a session. Presumably, the benefit provided by Selfit technology is due to the encouragement of patients to exercise more than in the conventional physical therapy program.
In addition, the Human-Machine Interface efficacy was not tested as a measured outcome in this study. In this study, the intervention was managed by a physical therapist, who introduced the Selfit system to the participant, and assisted him with workflows. Future study is required to address the human-machine interaction factor. In addition, the study did not employ personalized exercise regimentation for each participant. The exercise program was standardized and only a relatively small number of exercises were included. The possibility exists that a personalized exercise regimen by the Selfit system, which is tailored to stroke patients’ need may yield better results. Furthermore, the activity-based outcomes were measured with different technology in the control and interventional groups due to methodological limitations. For example, the control group had the conventional session, which includes walking around the hospital which could not be monitored by Selfit technology. Nevertheless, the accuracy of both technologies measuring session duration, movement duration, rest time, step count and step per second are likely to be similar and therefore the differences between the groups should not account for the differences in the measurement tools.
Conclusions
The findings of this study suggest that the Selfit system has the potential to improve mobility and gait-related functions in stroke patients. Additional studies should be conducted with a larger sample and longer program and follow-up periods to establish the benefit of incorporating the Selfit system into stroke rehabilitation programs.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors have no conflicts of interest to declare.
Funding
No funding was provided to support the study.