
Abstract
BACKGROUND:
Lower extremity arteriosclerosis obliterans (ASO) is the most common occlusive disease of the peripheral blood vessels.
OBJECTIVE:
To explore the application effect of symptom management-based rehabilitation strategy in postoperative functional exercises in patients with lower extremity ASO.
METHODS:
The researchers selected 136 patients that underwent lower extremity ASO surgery for the first time in their department from January to September 2020. Patients were divided into a control group (
RESULTS:
Three months (
CONCLUSION:
The rehabilitation management strategy, which is based on symptom management theory, can effectively improve the symptoms, quality of life and self-efficacy of ASO patients in continuous care. This nursing strategy is worthy of clinical promotion.
Keywords
Introduction
Lower extremity arteriosclerosis obliterans (ASO) is the most common occlusive disease of the peripheral blood vessels. A study reports that the number of ASO patients reached 200 million, and the disease’s incidence and prevalence are still on the rise [1]. Studies of the prevalence and risk factors of peripheral arterial disease at home and abroad show that the prevalence of ASO is 6.6% in adults over 35 years old, whereas, in patients older than 75, the prevalence has a positive relationship with age [2]. As the population ages, and the dietary structure changes, lower extremity ASO is becoming a worldwide public health problem.
ASO of the lower limbs is caused by the formation of atherosclerotic plaques of the lower limbs, which leads to arterial stenosis and occlusion. This causes chronic limb ischemia. According to the current investigation [3], patients have a poor understanding and control of ASO in China, as well as a high incidence, amputation rate and mortality rate. Meanwhile, the development and prognosis of ASO are related to improper patient self-management [4, 5]. Recurrent vascular blockage after AS surgery is mainly related to smoking, unstable blood glucose and hyperlipidaemia [6]. The relevant studies confirm that ASO patients’ self-management is affected by demographic characteristics, social and family situations, self-efficacy and other factors. Patients with high self-efficacy can manage their health and deal with various difficulties with medical staff [7, 8]. Therefore, the postoperative rehabilitation of ASO patients requires an exercise programme based on the patient’s characteristics, which will help the patient to recover.
The symptom management theory involves developing management strategies through symptom experience and finally evaluating the management’s effect. This can effectively improve patients’ health, quality of life and self-management ability [9, 10]. Rehabilitation management, which is based on symptom management theory, has been widely used in the clinical care of cancer patients [11]. However, there is no research on the application effect of rehabilitation management based on symptom management theory for postoperative functional exercises in patients with ASO.
This study applies rehabilitation management based on symptom management theory to ASO patients for the first time, aiming to explore the effect of rehabilitation exercises guided by symptom management theory on the functional rehabilitation of ASO patients. This study provides data support for clinical practice.
Materials and methods
General information
A total of 136 patients who first underwent lower extremity ASO (Fontaine IIb) surgery in the researchers’ hospital from January to September 2020 were selected. Patients were randomised into the control group (
Study methods
The control group
The specialised perioperative care routine and health education were implemented for ASO patients according to the general perioperative care of general surgery. The main contents include the following: 1) the aetiology, clinical manifestations, treatment and nursing points of the disease, which the charge nurse introduced; 2) the exercise time, method and points to consider during perioperation; 3) the name, effect and adverse reactions of oral and intravenous treatment; 4) the preparation and cooperation requirements of the special examination and operation and the significance of the results; 4) the pain evaluation method and the side-effects of the drugs; 5) key points of ankle pump movement and Buerger exercises after the operation; and 5) discharge health education. The nurses followed up with the patients via telephone one, three and six months after they were discharged. The contents of the follow-up included functional exercises, diet, sleep, psychological status and other factors. Meanwhile, the patients were informed of outpatient return visits. Three leaflets were issued by the department to explain the performance and prevention of complications to teach patients to identify complications early.
The experimental group
Based on the routine perioperative nursing intervention, the experimental group underwent the rehabilitation management strategy’s combined functional exercises and pain management, based on the theory of symptom management.
2.2.2.1 The establishment of the rehabilitation and nursing strategy group
The head nurse was the administrator of the team, and the whole-course nurses were responsible for specific operations. The whole-course nurses performed routine perioperative care during the inpatient phase, including diet, pain, medication and rehabilitation guidance. Rehabilitation strategies were developed by a specialist group led by two to three supervisor nurses.
2.2.2.2 The establishment of a WeChat group
1) Lectures on rehabilitation of functional exercises, lower limb oedema and pain management were sent every day through the WeChat group. The content was produced by the specialised group members, reviewed by the head nurse and presented in the form of a PowerPoint presentation. 2) Patients were to respond daily to the contents, including the rehabilitation exercises, kilometres to be walked and information on lower limb swelling and pain and were guided by specialist nurses and doctors; 3) The researchers set up relevant problems to guide the patients to express their own symptoms and experiences, especially concerning pain. Was the pain related to diet and failure to take medicine on time? Did the patients take anticoagulants as advised? Was the limb pain accompanied by other symptoms? The researchers learned about the patients’ rehabilitation needs through semi-structured enquiry.
2.2.2.3 The specific plan of the rehabilitation management strategy
After receiving the discharge order, the charge nurses evaluated whether the patient understood the medicine, diet, functional exercises and other information and made the patient’s discharge care plan. According to the patient’s operation and pre-discharge rehabilitation situation, the specialised group formulated an individualised rehabilitation plan, guided the patients and their families on how to perform the functional exercises and achieved self-efficacy by allowing the patients to conduct a self-evaluation.
Planned functional exercises
1) Three days after surgery, the patients exercised actively, sitting and standing for 10 to 15 minutes two to three times per day. Throughout the observation of the recovery situation, the movement transitioned to walking up and down the stairs and walking for 100 metres two to three times per day. Step by step, the frequency was increased. A plan was developed for the walking distance and Buerger exercises, and the exercise time and amount of exercise were recorded, along with any accompanying symptoms; 2) One week after surgery, the patients were guided to master the disease’s harm factors, quit smoking and establish healthy eating and living habits; 3) a week before discharge, the patients were taught how to self-monitor their skin temperature, colour and pulse. If there were any instances of reduced skin temperature, colour cyanosis or lower limb swelling, the patients were to inform the medical staff. The patients had to take care of their feet well to avoid scalding, and cold and hot compresses were prohibited.
Pain management
1) The specialist pain nurse evaluated the patient’s pain for the first time, including scoring and sleep quality. 2) A multi-node evaluation was conducted, including preoperative and postoperative during the experience of pain and before discharge. According to the results of the evaluation, the doctors were advised to give early analgesia and provide feedback 30 minutes after drug administration. 3) In order to avoid the influence of differences in culture, region and living habits, the content of the health education was presented through convergent media [12] and was not limited by time, space or region, which catered to the developmental trend of contemporary education, with the advantages of being easy to understand, convenient and fast. This maintained and improved the educational effect. Patients were encouraged to express feelings of pain, and caregivers conducted non-pharmacological interventions to relieve the pain.
2.2.2.4 Drug management
According to the discharge advice, the nurses formulated the order and time point plan for the medication, including antihypertensive drugs, hypoglycaemic drugs, anticoagulant drugs, stabilising plaque drugs, clearing drugs and drugs that promote blood circulation, and asked patients about the medication in the WeChat group every week.
2.2.2.5 The strategy adjustment scheme
The specialist team comprehensively evaluated the patients’ recovery. The team followed up with the patients via telephone one week, one month, three months and six months after discharge, and the outpatient follow-up occurred once per month. The disease management and rehabilitation exercises were reviewed at each follow-up. Treatment and convalescent blood pressure, blood sugar, D-2 polymer, the ankle-brachial index (ABI) and other information were collected, and line charts were made. The effects of the treatment were explained to the patients to help them identify with the effectiveness of the treatment and rehabilitation care. At the same time, the functional exercise programme was adjusted according to the line chart to determine whether to increase or decrease the exercises and whether to immediately return to the hospital for examination. During the intervention, the post-discharge follow-up guided the caregivers’ emotional support intervention, playing a supervisory and promotional role and understanding the rehabilitation needs of the patients.
2.2.2.6 The establishment of a public account to conduct convergent media health education
Xing Taohong’s financial media health education team achieved good results [13]. The researchers’ department made relevant content according to the patients’ discharge rehabilitation needs. Four specialised group leaders and team members, who were supervisor nurses or above, were responsible for the content, include the following: 1) high-risk factors inducing ASO and their related effects, such as smoking and irregular medication; 2) an animated display of the ASO surgery; 3) classification, usage and precautions of common drugs, such as aspirin, warfarin and rivaroxaban; 4) education surrounding ankle pump movement and Buerger exercises; 5) daily life management and dietary guidance, such as the control of blood pressure and blood sugar; 6) the self-monitoring of lower limb function; and 7) the re-examination’s time and content. All of this was presented in the form of ‘text
Evaluation indicators
Visual simulation scoring (VAS) was used for the pain evaluation. VAS is the most commonly used method to assess pain, and studies prove that it is a highly reliable method of evaluating acute and chronic pain in middle-aged and elderly people [14]. The system is divided into four levels, with a total score of ten points. A score of zero indicates painlessness, whereas one to three indicates mild pain, four to six indicates moderate pain and seven to ten indicates severe pain. The recovery effect was evaluated using the ABI with time nodes at one, three and six months after discharge. The exercise of self-care agency (ESCA), which includes care skills and self-care responsibility, was used for the self-care ability evaluation. Each entry was rated at level five, with a total score of 172. The higher the score, the better the self-care ability. A life quality self-evaluation scale with a ten-point system was used to assess the patients’ quality of life, including emotional status, physical pain, mobility and overall health. A high score indicated a high quality of life.
Statistical analysis
The data were analysed using the SPSS 21.0 statistical software. The measurement data were expressed as ‘mean
Results
The patients’ general data
Table 1 shows the patients’ general data. The mean age of the control group was 56.62
Comparison of the general data between the two patient groups
Comparison of the general data between the two patient groups
There was no significant difference in pain between the control group and the experimental group at the point of discharge (
The recovery effect in both groups
The ABI results show no significant difference in recovery effect between the control group and the experimental group at discharge (
Comparison of the ABI index between the two groups.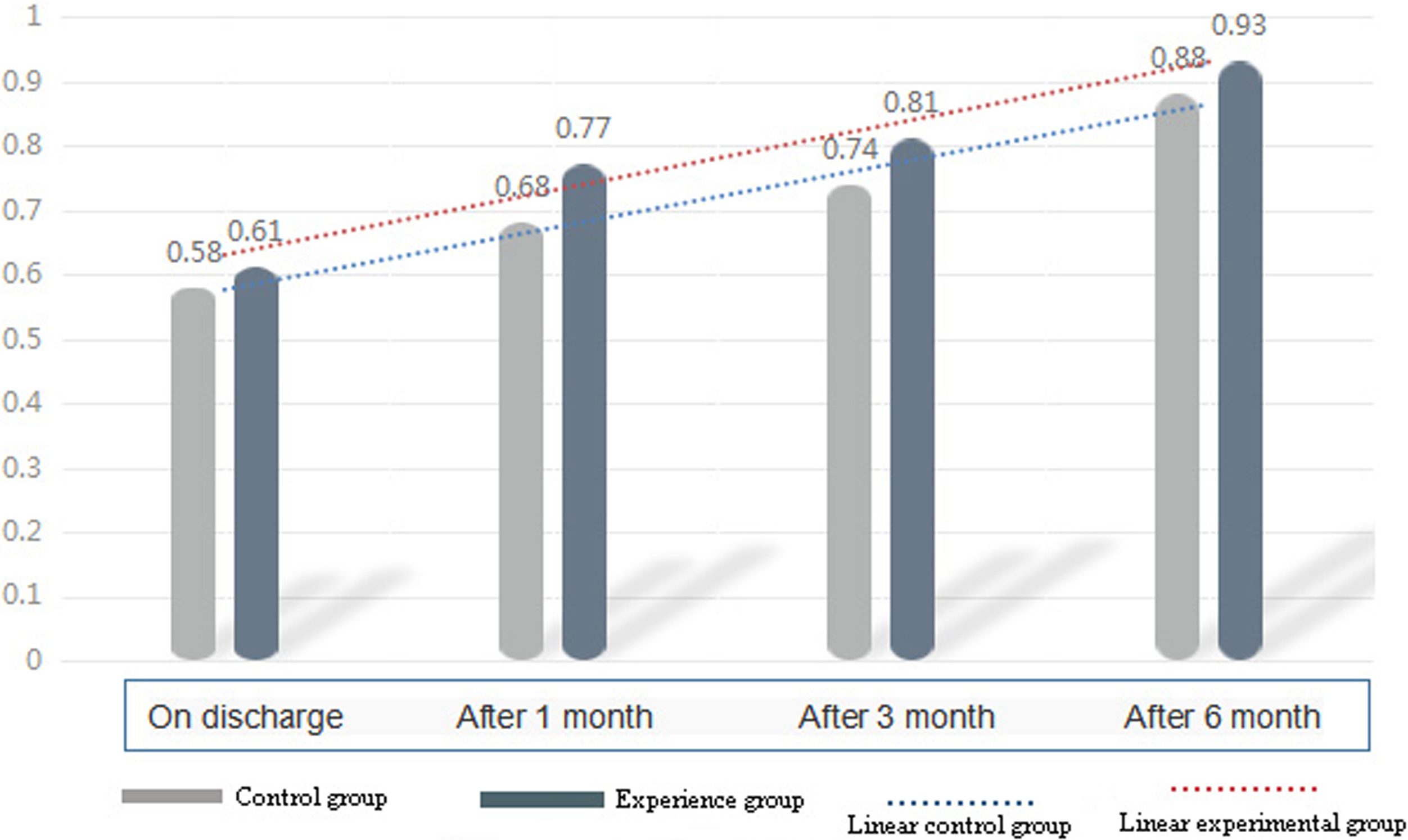
The ESCA statistics show that there was no significant difference in self-care ability at discharge between the two groups (
| Group |
|
Discharge | One month | Three months | Six months | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No | Mild | Moderate | Severe | No | Mild | Moderate | Severe | No | Mild | Moderate | Severe | No | Mild | Moderate | Severe | ||
| Control group | 68 | 4 (5.88) | 28 (41.18) | 28 (41.18) | 8 (11.76) | 4 (5.88) | 31 (45.59) | 26 (38.24) | 7 (10.29) | 18 (26.47) | 40 (58.82) | 6 (8.82) | 4 (5.88) | 36 (52.94) | 20 (29.41) | 11 (16.17) | 1 (1.47) |
| Experimental group | 68 | 5 (7.35) | 30 (44.12) | 26 (38.24) | 7 (10.29) | 4 (5.88) | 32 (47.06) | 26 (38.24) | 6 (8.82) | 23 (33.82) | 36 (52.94) | 6 (8.82) | 3 (4.41) | 40 (58.82) | 18 (26.47) | 7 (10.29) | 0 (0.00) |
|
|
0.396 | 3.140 | 8.055 | 10.191 | |||||||||||||
|
|
0.947 | 0.067 | 0.045 | 0.013 | |||||||||||||
Comparison of self-care ability in the two groups
Six months after the intervention, the mood status (
Comparison of life quality scores at 6 months after the intervention.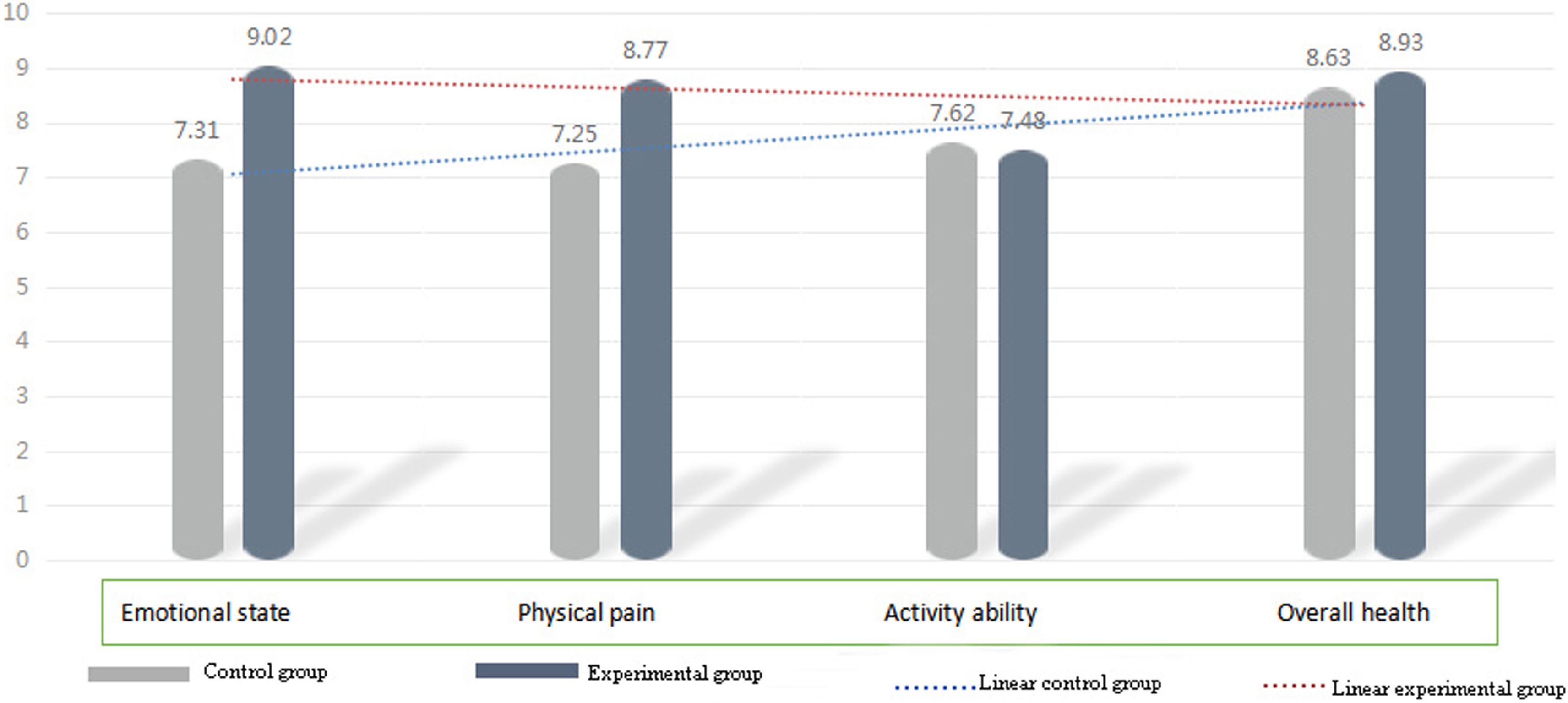
During hospitalisation, it is difficult for patients to fully master all knowledge of their disease and rehabilitation, and functional exercises are usually completed at home [15]. At the same time, the development of medical and public resources is unevenly distributed. The link between hospitals and the community is lacking. Patients recovering at home after surgery have difficulty accessing medical treatment. Network resources have overcome the obstacles of time and space, and patients receive seamless care and achieve good results [16, 17, 18]. Improving the prognosis of ASO patients and avoiding the disease’s progression and complications require the joint efforts of medical staff and patients. Therefore, in terms of strengthening patients’ health education, special attention should be paid to improving patients’ self-management ability when providing exercise guidance for rehabilitation. Studies have shown that, even if patients obtain some knowledge of functional exercises and related issues during hospitalisation, the functional exercises will gradually decline or cease post-discharge because of a lack of relevant support, poor compliance and other factors. In this study, the rehabilitation management strategy, which was based on symptom management theory, had a better effect on postoperative functional exercises in patients with lower limb ASO. This study shows that, after the intervention of the rehabilitation management strategy, patients’ sense of identity is enhanced, and their autonomous initiative is improved. In addition, patients’ self-care ability, nursing skills, self-care responsibility, health knowledge level and self-concept are also improved significantly. At the same time, the comparison of patients’ ABI shows that the rehabilitation management strategy is effective. Continuing nursing focuses on the improvement of patients’ self-management ability, which can improve the effects of treatment and patients’ functional recovery.
Severe pain can trigger a series of changes in bodily functions. Studies have shown [19, 20] that the stress response caused by pain puts the body into a high coagulation state, which may cause arterial thrombosis at the surgical site for patients with cardiovascular, especially for patients with ASO. In addition, the more pain points and the longer the pain’s duration, the greater the psychological impact, resulting in a negative mood and lower pain acceptance [21]. In this study’s rehabilitation strategy, patients’ pain and anxiety were effectively relieved through WeChat group supervision of drug use, analgesic propaganda, education of related knowledge and multi-node evaluation. The application of the rehabilitation strategy could improve patients’ quality of life and ensure safe drug use.
ASO is a chronic degenerative lesion, and the factors affecting patients’ rehabilitation mainly include blood sugar, blood pressure, diet and changes in the amount of exercise [22]. Moreover, some studies show that patient compliance will gradually decrease after discharge [23]. The essence of systematic rehabilitation strategy education is centralised management. Unlike traditional perioperative health education, which is disease-centred, AOS is patient-centred and starts by focusing on the psychological and physiological aspects. A series of nursing measures have been taken to improve the rehabilitation effect. With the help of convergent media, this study covers health-related knowledge from multiple angles and answers patients’ questions in a timely manner through a public account and WeChat group to strengthen patients’ disease and rehabilitation knowledge, enhance their self-care ability and improve their condition. Some studies have confirmed through the structural equation model that self-efficacy, as an intermediary force, indirectly affects patients’ quality of life by affecting self-management [24]. Therefore, while performing the centralised rehabilitation strategy, it is important to make the individualised adjustment plan according to the patient’s actual situation and changes in symptoms and formulate a quantitative exercise plan, including Buerger and progressive walking exercises to promote blood circulation in the lower limbs, which can effectively accelerate the recovery of limb functions.
This study designed a set of rehabilitation management strategies based on the theory of symptom management, which has a good application effect in the postoperative functional exercise of patients with lower extremity arteriosclerosis obliterans. The rehabilitation management system, designed according to national resources, requirements and patient needs, has its own characteristics and organizational structure. The primary role of any health care system is to provide effective, accurate, safe and equal service to all patients [25, 26, 27]. In a rehabilitation management system based on symptom management theory, in addition to the knowledge and experience of doctors and nurses, inpatient diagnosis and treatment and rehabilitation after discharge, it is necessary to have the correct and tested medical apparatus. In future research, in order to make the rehabilitation management system more scientific, it is necessary to introduce metrology into medicine and define medical device inspection standards and regulations. In the rehabilitation management strategy based on symptom management theory, improving the safety and reliability of equipment will make the treatment and rehabilitation of patients better and more reliable [28]. Moreover, with the advancement of technology, artificial intelligence is more widely used in medical rehabilitation [29, 30, 31]. In future research, the integration of artificial intelligence and rehabilitation management will greatly reduce the workload of doctors and nurses, and make the recovery of patients more efficient.
This study has a few limitations. The main limitation is the small sample size, and it is difficult to generalise the results of the study because of its single-centred nature. In addition, the follow-ups ended after six months; therefore, the study lacks long-term follow-ups, which may also have influenced the results.
Conclusion
The rehabilitation management strategy based on symptom management theory focuses on the needs of ASO patients in continuous care and effectively improved their symptoms, quality of life and self-efficacy.
Ethics statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Shanxi Bethune Hospital.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Competing interests
None of the authors have any personal, financial, commercial, or academic conflicts of interest.
Funding
Not applicable.
Author’ contributions
Yuan YY and Chen JQ conceived the study, Wang XQ participated in its design and coordination, and Song JL helped draft the manuscript. All authors read and approved the final manuscript.
Footnotes
Acknowledgments
Not applicable.