
Abstract
BACKGROUND:
Monitoring fetal weight during pregnancy has a guiding role in prenatal care.
OBJECTIVE:
To establish a personalized fetal growth curve for effectively monitoring fetal growth during pregnancy.
METHODS:
(1) This study retrospectively analyzed the birth weight database of 2,474 singleton newborns delivered normally at term. The personalized fetal growth curve model was formed by combining the estimating birth weight of newborns with the proportional weight formula. (2) Multiple linear stepwise regression method was used to estimate the birth weight of newborns.
RESULTS:
(1) Delivery gestational age, weight at first visit, maternal height, pre-pregnancy body mass index, fetal sex, parity had significant effects on birth weight. Based on these parameters, the formula for calculating term optimal weight was obtained (
CONCLUSIONS:
A model of personalized fetal growth curve can be established, and be used to evaluate fetal growth and development through estimated fetal weight monitoring.
Introduction
Abnormal fetal growth is associated with increasing perinatal morbidity and mortality [1]. Therefore, it is very important to monitor the fetal development during pregnancy, which also plays a guiding role in obstetric management.
One of the most popular methods to monitor fetal development is based on fetal weight estimation, which is determined by a population-based birth weight data. However, in addition to maternal complications, the birth weight is also affected by many genetic factors from the parents. The term optimal weight (TOW) of a fetus can be obtained according to the maternal height, the weight at first visit, parity and other factors [2].
In this study, the 10
Currently, there are many ways to identify SGA and LGA fetuses, such as the measurement of uterine height, abdominal circumference of the pregnant woman, but the results are often influenced by many factors. At present, the most accepted method for clinical evaluation of fetal weight is to calculate estimated fetal weight (EFW) through ultrasound examinations. Recently, INTERGROWTH-21st project published a new formula in order to achieve this purpose, in which ultrasound examination results, such as biparietal diameter, head circumference, abdominal circumference and femur length were included [4].
Internationally, Hadlock fetal growth curve [5] and INTERGROWTH-21st fetal growth curve [6] are all not customized. There is also a NICHD fetal growth customized curve [7]. For Chinese people, there are semi-customized fetal growth curves established by Mikolajczyk and Zhang [8], and fetal growth curves for people in southern China established by Cheng [9], but it’s not a personalized growth curve for every pregnant woman. Accurate assessment of fetal growth is an essential part of antenatal care and perinatal research [10]. Many studies have shown that customized fetal growth standards are more associated with abnormal fetal development and adverse pregnancy outcomes than not customized standard [11, 12, 13, 14].
The purpose of this study was to establish an adjustable, personalized fetal weight standard for each pregnant woman. Based on the estimation of maternal genetic factors, fetal growth potential (the optimal weight and optimal range of fetal normal growth) was estimated, and fetal development status was judged by comparing with actual fetal weight on this basis. Intervention measures following early detection of abnormal fetal growth have a very important clinical significance.
Materials and methods
Study population
2,474 pregnant women without any complications, who gave birth in Peking University People’s Hospital in China from April 1, 2014 to December 31, 2019, were included. Information including the pregnant woman’s age, parity, height, weight at first visit, delivery gestational age (GA), fetal sex and birth weight were recorded. The means of height, pre-pregnancy body weight, delivery GA and birth weight are shown in Table 1.
Mean parameters of normal pregnant women and fetuses
Mean parameters of normal pregnant women and fetuses
Notes: Data are given as mean
According to domestic and foreign research results, delivery GA, weight at first visit, maternal height, pre-pregnancy BMI, parity, fetal sex are the main factors affecting TOW, which have to be adjusted in the formula in order to calculate the true growth potential of a fetus. This method has been validated in many international studies [15].
Through linear stepwise regression analysis of all the 2,474 pregnancies’ conventional ultrasound database, we obtained the coefficients of each variables. and then established the Eq. (1).
Where
According to Gardosi [16] in 1995, a polynomial formula of Y
To determine whether a fetus is SGA or LGA, the formulas for calculating the normal range of the fetal weight proportion at certain GA were also constructed as follows:
The 90th percentile formula:
The 10th percentile formula:
SPSS for Windows 23.0 was used. Continuous variables were tested by Independent-Samples
Results
Formula for TOW calculation
Through the analysis of multiple maternal genetics and other factors, it was concluded that delivery GA (in days), weight at first visit, height, pre-pregnancy BMI, parity and fetal sex all had significant influences on TOW. If each coefficient can reflect the contribution of parameters to weight, mean to weight can be carried out.
Comparison of coefficients on influencing term optimal weight
Comparison of coefficients on influencing term optimal weight
Notes:
The constant in Table 2 represents the expected birth weight adjustment constant. A pregnant woman who weighs 63.3 kg and is 162.7 cm in height at her first visit is expected to have a fetal TOW of 3418.4 g in 280 days. Equation (3.1) showed the calculation progress of TOW.
According to Eqs (2)–(3.1), an easy-to-operate personalized fetal growth curve model was created. Here we used an example to show the core steps of how to apply the curve.
Pregnant woman A went into a hospital at 24
Pregnant woman A enters information at the hospital during the second trimester
Pregnant woman A enters information at the hospital during the second trimester
Output information about personalized fetal growth curve model
Notes: Revised weight, the difference between the newborn birth weight constant and the estimated newborn birth weight.
Schematic diagram of personalized fetal growth curve results of a pregnant woman A.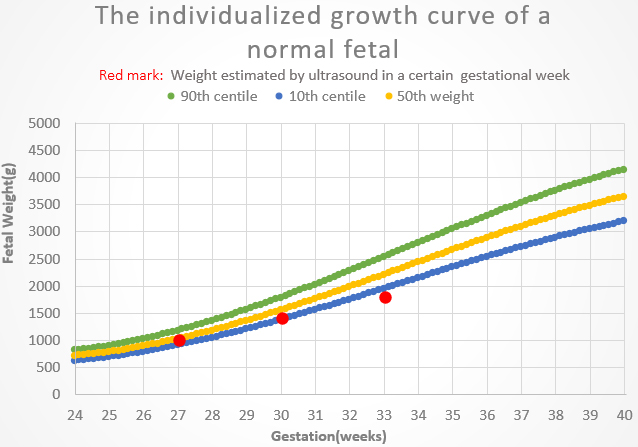
That is, the TOW of pregnant woman A was expected to be 3,639 g. The corresponding 10th to the 90th percentiles were 3,130 g and 4148 g. Her personalized fetal growth curve is shown in Fig. 1. Three curves in the figure represented the 10th percentile, the 50th percentile, and the 90th percentile of fetal weight at each GA. The red marks represented the EFW by ultrasound examination at 27, 30 and 33 weeks, that is, 500 g, 1000 g and 1400 g successively. It can be observed from the schematic diagram that the fetal weight at 33 weeks was less than the 10th percentile, and the risk of that it may be a SGA fetus can be suspected.
The purpose of this study was to develop a personalized fetal growth curve for a Chinese population. The results showed that the parameters significantly associated with personalized TOW were delivery GA, maternal height, weight at first visit, pre-pregnancy BMI, parity and fetal sex. However, the research results of Gardosi [16] showed that GA, the weight of the initial diagnosis, had multiple square influences on fetal weight, while other factors had linear influences.
To establish an adjustable personalized fetal weight standard for each pregnant woman, the EFW formula obtained in this study was combined with the proportional weight formula constructed by Gardosi. And based on the data of normal pregnant women who gave birth in Peking University People’s Hospital within more than 5 years, the model was established, and the coefficients in the formula were more accurate. According to the model of fetal growth curve, we can determine whether a fetus is SGA or LGA through personalized standard, but not the whole population standard.
Both SGA and LGA are associated with adverse perinatal outcomes. Determining which fetus is too small or too large accurately is very important to detect such high-risk babies. Personalized fetal growth curves can help us to achieve this purpose much better, and the procedure makes this progress more easily to operate. And at the same time, we should know that to verify the effectiveness of the personalized fetal growth curve model needs to be studied further in the future.
Conclusion
The objective of this study was to provide obstetricians with a method to screen pathological growing fetuses, and to provide personalized care for them. When a pregnant woman comes to the hospital for the first prenatal care at around 24 weeks, doctors can acquire her personalized fetal growth curve according to several factors, such as delivery GA, weight at first visit, maternal height, pre-pregnancy BMI, parity and fetal sex. And then the EFW by ultrasound examination can be used to determine whether the fetal growth is within the optimal range. If the EFW is less than the 10th percentile, it will be doubted with SGA. If it is greater than the 90th percentile, LGA will be suspected. Monitoring fetal growth during pregnancy is crucial to the following prenatal care and the safety of the fetuses. A personalized fetal growth curve can help to achieve this purpose much better, and avoid the possible misdiagnosis of SGA and LGA when based on population standard.
Footnotes
Acknowledgments
This research was supported by National Key R&D Program of China (2019YFC0119700), Bill & Melinda Gates Foundation (OPP1148910), Beijing International Science and Technology Cooperation Base for Intelligent Physiological Measurement and Clinical Transformation.
Conflict of interest
None to report.