
Abstract
BACKGROUND:
The prevalence of health information technology (HIT) as an adjunct to increase safety and quality in healthcare applications is well known. There is a relationship between the use of HIT and safer-prescribing practices in long-term care.
OBJECTIVE:
The objective of this systematic review is to determine an association between the use of HIT and the improvement of prescription administration in long-term care facilities.
METHODS:
A systematic review was conducted using the MEDLINE and CINAHL databases. With the use of certain key terms, 66 articles were obtained. Each article was then reviewed by two researchers to determine if the study was germane to the research objective. If both reviewers agreed with using the article, it became a source for our review. The review was conducted and structured based on Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
RESULTS:
The researchers identified 14 articles to include in a group for analysis from North America, Europe, and Australia. Electronic health records and electronic medication administration records were the two most common forms of technological interventions (6 of 14, 43%). Reduced risk, decreased error, decreased missed dosage, improved documentation, improved clinical process, and stronger clinical focus comprised 92% of the observations.
CONCLUSIONS:
HIT has shown beneficial effects for many healthcare organizations. Long-term care facilities that implemented health information technologies, have shown reductions in adverse drug events caused by medication errors overall reduced risk to the organization. The implementation of new technologies did not increase the time nurses spent on medication rounds.
Introduction
Background
The prevalence of health information technology (HIT) has been increasing since the 1990s across all aspects of U.S. healthcare organizations [1]. The term HIT “refers to the electronic systems health care professionals – and increasingly, patients – use to store, share, and analyze health information.” HIT includes health information exchange (HIE), electronic health records (EHRs), ePrescribing, EMAR, privacy and security, and other related topics [2].
HIT is the use of an electronic environment to exchange health information and includes programs such as electronic health records (EHRs), health information exchanges (HIEs), telemedicine, patient portals, and personal health records (PHRs). These programs are used by both providers and patients to transmit health information. According to the United States Department of Health and Human Services’ website, HIT used in the healthcare setting “will improve the quality of healthcare, prevent medical errors, reduce healthcare costs, increase administrative efficiencies, decrease paperwork, and expand access to affordable healthcare” [3]. Furthermore, implementation of technology in long-term care (LTC) facilities has been shown to enable better decision making and improved clinical documentation [4]. Although most healthcare organizations have been quick to adopt some form of HIT, LTC facilities have fallen behind and have been slow to implement such programs [5]. LTC facilities have been so slow to adopt that EHR adoption national estimates are nearly nonexistent [1].
In examining reasons behind the slow adoption of HIT in LTC, the high cost of implementing seems to be at the top. When the Health Information Technology for Economic and Clinical Health (HITECH) Act was enacted in 2009, its goal was to support the adoption of EHRs in healthcare systems. This support included incentive money made available to eligible providers and hospitals through the Medicare and Medicaid EHR Incentive Programs [1]. Unfortunately, LTC facilities were not included as eligible healthcare organizations in this funding program. The lack of financial support has led to the lag in HIT adoption in LTC. This is unfortunate given the beneficial outcomes these facilities would see if they did have EHRs. One major benefit could be a potential reduction in the number of adverse drug events affecting residents.
From 2013–2014, there were about 2.2 million Americans residing in either LTC or assisted living facilities and of this number, nearly half of the residents were prescribed at least 9 daily medications [6]. These residents are affected by a phenomenon called polypharmacy. Polypharmacy is defined as the concomitant use of five or more medications [7, 8, 9]. Polypharmacy is the single most common cause of adverse drug events in LTC [10]. An adverse drug event (ADE) is an injury resulting from medical intervention related to a drug [11]. This includes medication errors, adverse drug reactions, allergic reactions, and overdoses [7]. Research has shown that about 16–27% of residents experience a medication error and around 75% of residents are prescribed at least one potentially inappropriate medication [8]. Most medication errors are preventable and can occur at any phase of the medication use process, such as prescribing, dispensing, documenting, monitoring, and administering [6].
In an LTC facility, it is common practice for the provider to give prescription orders over the telephone to the nurse [12]. This practice opens a window of vulnerability in the system of receiving medication orders, allowing for errors to potentially occur [13]. Illegible handwritten orders from either the provider or nurse are also a cause of medication errors [13]. The issue of medication errors could possibly be alleviated with the implementation of electronic-prescribing, or e-prescribing. Technologies such as computerized provider order entry (CPOE) systems have shown to be successful in reducing prescription errors [14]. Potentially inappropriate medications are prescribed if the provider is not aware of certain medications the patient is currently taking that may cause a drug-drug interaction.
LTC facilities tend to have multiple providers that oversee residents [13]. Providers read the patient record to learn about their medical and medication history. Facilities must implement a strong system to continually update medication administration records. With certain EHR systems, there is order integration in place that will create a warning message upon the entry of a potentially inappropriate medication being prescribed. There are several key areas in LTC that can benefit from the adoption of HIT. These include transfer of data, regulatory compliance, quality improvement, structured clinical documentation, medication use process, and communication [15].
Researchers analyzed the common causes of medication errors within the LTC setting. Tariq et al. found five underlying themes associated with technological interventions in LTC: reduced risk, decreased error, decreased missed dosage, improved documentation, and no change in time spent in the medication entry or administration process. The excess workloads were found to be a direct result of staffing shortages and high levels of turnover [16].
Jiang et al. identified 21 risk factors for medication failure. The most common risk factors fell under the category of ineffective monitoring processes [17]. This aligns with research by Gurwitz et al. which determined that errors both in monitoring (325 of 464 preventable medication errors) and ordering (315 of 464 preventable medication errors) were responsible for the largest percentage of preventable medication errors [19].
When researching LTC facilities, their adoption of HIT and the effect on adverse drug events, revealed that little research has been conducted. This is most likely due to the slow adoption of HIT in the LTC setting. Studies have shown that staff members tend to exhibit an interest in learning to navigate new HIT systems despite posed challenges such as technology support, workload changes, and insufficient training [15].
Objective
The aim of this systematic review is to determine if a relationship exists between the use of HIT and a safety improvement in prescription administration in LTC facilities.
Material and methods
Sources
The systematic review was conducted with techniques from the assessment of multiple systematic reviews (AMSTAR) [18] and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [20]. This review was also constructed and conceptualized utilizing the Kruse Protocol for writing systematic reviews [21]. The researchers utilized the CINAHL, through EBSCO, and PubMed, through MEDLINE, databases. These two databases were identified and utilized due to their widespread availability, improving the replicability of the review. A Boolean search chain was utilized to identify articles germane to the research topic. The search chain is made up of keywords pulled from Medical Subject Headings (MeSH) section within the PubMed database. The keywords utilized to conduct the MeSH search were: HIT, medication errors, and LTC. The resulting MeSH terms were incorporated into a Boolean search chain which is displayed in Fig. 1. A combination of MeSH terms helped ensure the search was exhaustive.
Literature search utilized to identify the group for analysis, with inclusion and exclusion criteria.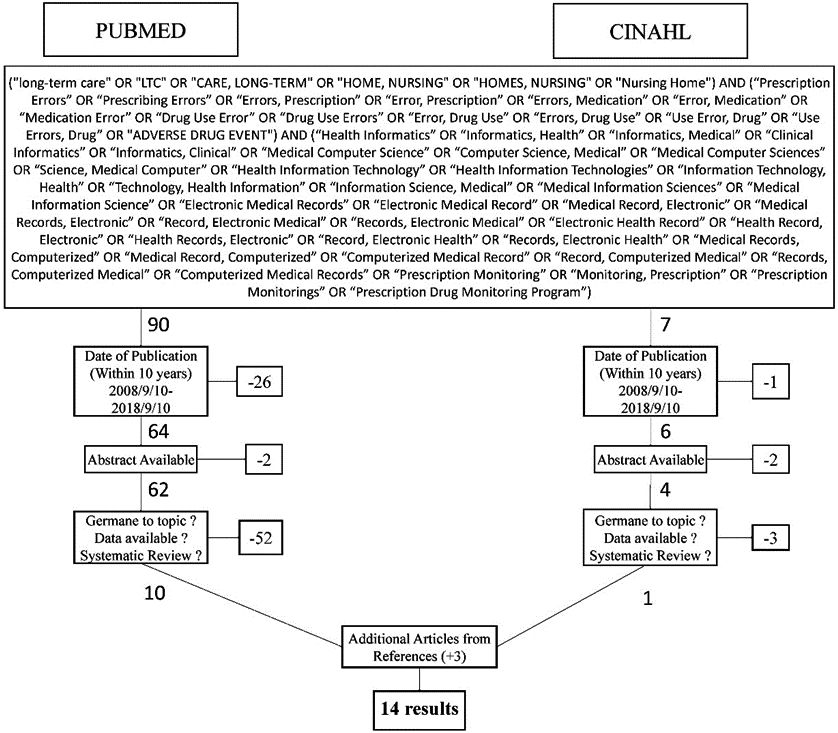
Chart of frequency and proportion of outcomes.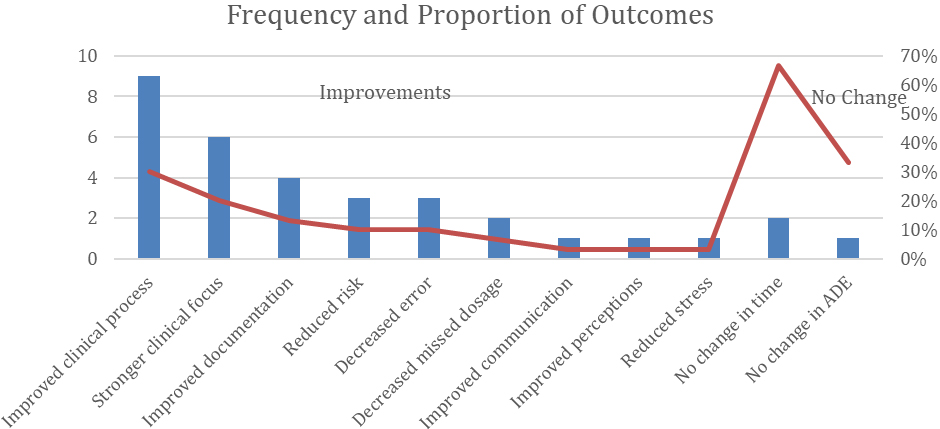
For an article to be included for review, the article had to have been published within 10 years of the database search date. Searches were conducted between September 3rd and 4th in 2018. The articles had to exhibit an association between HIT (HIT), medication errors, and LTC (LTC). Articles had to have an abstract available within either CINAHL or PubMed.
Study selection
Figure 1 illustrates the step-by-step selection of articles to include in the review. The Boolean search chain yielded 90 articles within PubMed and 7 articles within CINAHL. The results were then limited to those published within the last 10 years, which eliminated 26 articles within PubMed and 1 article within CINAHL. The results were then filtered to remove articles that did not have an abstract available. This filter removed 2 articles from PubMed and 2 articles from CINAHL. This process left 66 articles for the researchers to evaluate. Researchers then conducted a review of available abstracts to determine if the articles were germane to the research topic.
Selection bias
To counter potential selection bias in the review, a minimum of two researchers reviewed each abstract. Researchers were instructed to keep individual notes on each abstract. An initial consensus meeting was held to compare notes. If every researcher that reviewed an abstract agreed, the article was either included in the group for analysis or removed from analysis based on the consensus. In the event of a disagreement, the researchers discussed the article in detail to determine if the article should be included for analysis. A Kappa statistic of 0.83, indicating strong agreement, was calculated following the consensus meeting [22, 23].
Synthesis of results
Researchers created a literature matrix (LM) within Excel to document and organize the 66 research articles that resulted from our search. Abstracts were screened by multiple reviewers, and notes were recorded for discussion. Articles removed from analysis were documented as being: a duplicate, having no outcomes, being a review, or for not being germane. Following the consensus meeting, 31 articles were determined to meet the criteria for inclusion into the review. Articles were analyzed by a minimum of two researchers and notes were recorded by each researcher for further discussion. Following the second consensus meeting, 11 articles were determined to include in the analysis. The references of the original 66 articles were then scanned to identify additional articles for inclusion. Researchers were able to identify an additional 3 articles for inclusion, resulting in a total group for analysis of 14 articles. Each researcher analyzed 7 of the 14 articles, notes were recorded of potential themes, and a third consensus meeting was held to discuss common themes.
Results
Study selection and study characteristics
The group for analysis consisted of 14 articles [24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37]. Table 1 lists in reverse chronological order the study design, the technological intervention, country of origin, the impact the technology had on LTC facilities, and miscellaneous notes about medical outcomes and bias. The articles ranged from 2008–2017. Seven of 14 (50%) articles focused on nursing facilities [25, 28, 29, 30, 31, 34, 36], 4 of 14 (29%) articles involved residential aged care facilities [26, 27, 31, 33], and 3 of 14 (21%) articles involved various LTC facilities [24, 28, 35]. Five of 14 (36%) were from the U.S. [27, 33, 34, 36, 37], 4 from Australia [24, 26, 28, 31], 2 of 14 (14%) were from Sweden [25, 35], 1 of 14 (7%) was from Canada [29], 1 was from the Netherlands [30], and 1 was from Denmark [32]. Only one article analyzed reported medical outcomes [23].
Individual study results from the group for analysis
Individual study results from the group for analysis
CDSS, Clinical decision support software; CPOE, Computerized provider order entry; EHR, Electronic health record; eMAR, Electronic medicine administration record; EMM, Electronic medication management; GRAM, Geriatric Risk Assessment MedGuide; ICT, Information communication technology; MDSS, Medical decision support system; MDT, Medication distribution technology; PDA, Personal digital assistant.
Electronic health records (EHRs) were evaluated in 3 of 14 (21%) studies [24, 28, 31]. Electronic medicine administration records (eMARs) were also evaluated in 3 of 14 (21%) studies [25, 26, 36]. Other forms of technology, each evaluated in one study, were electronic medication management (EMM) [27], an online medication error reporting system, clinical decision support systems (CDSSs) [30], a personal digital assistant (PDA) with CDSS [35], information communication technology (ICT) [32], computerized provider order entry (CPOE) [37], automated monitoring plans, and medication distribution technology (MDT) [29].
In Australia, the implementation of an EHR improved documentation levels while not significantly changing nursing time spent on most activities, and improved documentation results in safer prescribing [28]. The EHR was also responsible for greater completeness and more comprehensiveness of electronic admissions records, which greatly contribute to proper admission policies [31]. In a nominal-group technique, the EHR was ranked as the 5
In Sweden, eMAR was associated with lower levels of stress about causing medical error and resulted in a more positive perception of the medication administration process [25]. In Australia, eMAR did not significantly change nursing time spent on medication administration, but it increased documentation compliance, decreased probability of a missed dosage, increased freedom from the error of signing twice, increased documentation space, and improved time-recording of administering dosages; however, it was also associated with adverse unintended consequences during power outages [26]. In the U.S., eMAR shortened medication order entry, improved communication, improved clarity of the medication administration process, and when combined with other factors, it was responsible for reduced occurrences of late and missed doses [36].
Electronic medication management (EMM) functions in the U.S. were studied such as maintaining medications, ordering prescriptions, managing allergy lists, and warning of drug interactions or contraindications [27]. While no medical outcomes were reported, EMM is expected to improve the overall quality of care and patient safety in LTC facilities.
The only article that reported medical outcomes studied a Geriatric Risk Assessment MedGuide (GRAM) system in the U.S. to monitor falls and medication-related delirium [33]. The GRAM was associated with a decrease in mortality, hospitalization, delirium onset, and adverse drug event hospitalization.
The article on CPOE (without decision support) in the U.S. did not report a reduction in ADE rate in the LTC setting [37]. The article on CDSS in the Netherlands reported great potential to serve as a second-generation medication surveillance system [30]. The use of a personal digital assistant (PDA) as a medical decision support system (MDSS) showed improvement in ability to obtain profiles for medication which enabled nurses to reduce medication errors [35].
Information Communication Technology (ICT) in Denmark also reported potential to improve handover between shifts at aged care facilities [32]. A web-reporting site was made available to 393 nursing homes in North Carolina, and it recorded 5,823 errors over the course of one year: This information made available to the general population could easily prevent repeat errors in other facilities [34]. Finally, Medication Distribution Technology (MDT) in Canada was able to identify medication errors more rapidly than a manual process, which reduces the risk of harm to residents [29].
Risk of bias within studies
Some studies involved questionnaires that would have been stronger study designs if they had included a control group, which would have strengthened their validity [35]. One did not use any randomization, and another used a convenience sample, which both lend themselves to selection bias [24, 26] Another reported very different pre-implementation numbers prior to the technological intervention, which is a form of selection bias because the two organizations were not similar for comparison [25]. Multiple studies self-identified reporting bias.
Additional analysis
Affinity matrix of observations of results of technological implementation
Affinity matrix of observations of results of technological implementation
A tabulation was created to organize the observations in the articles analyzed. Table 2 lists these observations in terms of improvements (30 of 33, 91%) and no change (3 of 33, 9%) as a result of the technological intervention (negative effects were not observed). Several individual observations were categorized into themes. Improved clinical process occurred nine of 30 improvements (30%) [24, 26, 27, 29, 30, 32, 34, 36]. Observations of stronger clinical focus occurred six of 30 improvements (20%) [29, 33, 35]. Improved documentation occurred in four of 30 (13%) improvements [26, 28, 31]. Reduced risk and decreased error both appeared 3 of 30 (10%) improvements [26, 29, 31, 35]. Decreased missed dosage appeared in 2 of 30 (8%) improvement [26, 36]. The rest of the observations of improvement appeared only one time each (3%) [25, 36]. The bottom of the table shows the two observations of no effect: no change in time (2 of 3, 67%) [26, 28], and no change in ADE rates (1 of 3, 33%) [25].
Summary of evidence
In this systematic review, the researchers analyzed a group of 14 existing articles. The existing research evaluated the impact of several different forms of HIT that were implemented in LTC (LTC) facilities. This technology included, but was not limited to, systems such as electronic medication administration records (eMARs), electronic medication management (EMM) systems, clinical decision support software (CDSS), electronic health records (EHRs), personal digital assistants (PDAs), and computerized provider order entry (CPOE).
The eMAR system was one of the most common types of technology implemented in LTC facilities and was evaluated in 3 of 14 studies. In one study, the participants were two LTC facilities of similar demographics that were both utilizing paper medication records. One of the facilities implemented an eMAR system while the other remained paper-based. Overall, it was found that the implementation of the eMAR system was perceived positively in the medication administration process. Nurse satisfaction improved and the perceived safety of the medication administration process for patients increased. The risk of several types of medication errors also reduced with the eMAR implementation, perceived workload improved, as did communication among staff members [35].
A second study involving an eMAR system analyzed 5 LTC facilities that needed a large-scale technology change and implemented an eMAR into each facility. The eMAR shortened the time of medication ordering, improved communication, and improved clarity of the medication administration process. In combination with other factors, the new technology also reduced the occurrences of late and missed doses of medication [36].
Another study involved one LTC facility with two separate units: one of which used an eMAR. After observing 7 nurses administering medication over 12 shifts, it was found that the use of an eMAR did not significantly change nursing time spent on medication administration. The unit with an eMAR saw improvement in compliance with organizational requirements for documentation, decreased probability of a missed dosage, and improved time-recording of administering dosages [26].
The other commonly implemented technology in LTC is EHRs. An observational work-sampling study was undertaken over a 2-year period with nursing staff before and after the implementation of an EHR. It was found that the use of an EHR improved documentation levels while not significantly changing nursing time spent on most activities. The improvement of documentation has been shown to result in safer prescribing [28]. Implementation of an EHR system was also shown to improve the completeness of admission forms. This study took place in Australia and included 9 LTC facilities. Overall, they examined 147 paper and 251 electronic admission forms and found that the electronic admission forms had a higher prevalence of completeness which helps to reduce the risk of potential medication errors [31].
Other forms of technology such as a CDSS and EMM were shown to prevent medication errors by giving alerts on potential drug interactions and inappropriate doses. A PDA was shown to be effective and efficient at pulling a patient’s record and preventing adverse drug reactions.
A study conducted by Lyhne et al. found the use of ICT has the potential to improve handover between shifts, thus reducing the risk of adverse events [32].
The final technology evaluated in LTC facilities, MDT, is composed of two parts. Part one is an automated packaging device in the pharmacy servicing the facility. Part two is a mobile medication cart used to dispense medications in the facilities. The use of MDT is believed to improve the detection of medication errors and to enhance the medication-use process security. Baril et al. conducted a study in 6 LTC facilities utilizing an MDT system in Quebec, Canada with a total of 600 residents. It was determined that the MDT was able to effectively identify potential medication errors, reducing the risk of harm to the residents [29].
A key theme found through article analysis, observed in 3 of 14 studies, is that the use of HIT did not significantly increase the amount of time consumed on nursing activities. While time did not increase, the quality and timeliness of documentation did significantly improve. The improvement in documentation was observed in 6 of 14 studies. Improved documentation, using HIT, reduces the potential risk to the patient. The research also found that the implementation of HIT reduced the occurrences of late or missed doses. The decreased likelihood of late or missed doses was observed in 3 of 14 studies. Overall, the implementation of information technology systems enabled improvements in overall compliance and organization of patients’ health records within the LTC facilities.
Comparison to other studies
The results of this review aligns with existing work conducted on the topic. Implementing EHRs in LTC facilities improved documentation efficiency (including decreased time spent on documentation), improved communication among staff and between staff and residents, increased the understanding of a resident’s needs, and facilitated quicker decision making [25]. The researchers concluded that these improvements improved quality of care and reduced the potential for adverse events.
The use of EHRs improved patient safety in residential aged care homes [39]. The researchers concluded that EHRs allow for better access to patient records and helps facilitate decision making. EHRs also helped to alert providers of potential drug interactions [39]. Both CDSS and CPOE have a positive impact on improving medication safety [40].
Other healthcare settings have found a more definitive association between the implementation of HIT and a reduction in medication errors. Bates found that CPOE and CDSS can improve the safety of drug administration in hospitals, especially in terms of ordering [41]. Bates also concluded that HIT will reduce the burden of menial tasks on providers [41]. HIT can reduce medication errors, while at the same time reducing the utilization of redundant care. The researchers also found that HIT helped improve the adherence of providers to care guidelines and improved monitoring and surveillance [42].
Implications
The research shows the benefit of implementing HIT in the LTC setting. HIT has the potential to reduce the occurrence of medication errors. These types of errors cost an estimated $42 billion worldwide, so any stride toward reducing their occurrence can yield significant cost savings [9]. Improving quality of care and reducing the potential burden placed on care providers could also improve staff retention.
Limitations
The systematic review was limited by the lack of existing evidence on the adoption of HIT in the LTC setting. Other studies highlight the causes of this lack of adoption [43, 44]. The limited existing research prevented researchers from focusing on a specific form of HIT. Publication bias also limited the research as journals tend to only publish research with significant results, thus limiting the pool of existing research to pull from.
Lack of research forced consolidation of LTC facilities for analysis. This complicated assessment of the impact of HIT on an individual type of facility. Depth of research would have enabled analysis by infrastructure, location, system, and sources of funding.
Conclusion
LTC residents are prescribed as many as 9 medications per day (or more) [6]. This compels the analysis of methods to reduce the potential for prescribing errors. HIT can reduce prescribing errors. Unfortunately, LTC facilities have lagged behind other sectors in the adoption of HIT because of the lack of funding these facilities received from the HITECH Act. This systematic review analyzed the effect of technological interventions on prescribing errors with no change in time spent on documentation. This research can be beneficial to decision-makers in the LTC setting that are considering implementing HIT. The research can be used to ease apprehension from the nursing staff that the HIT will be an added burden.
Future studies
Future research is needed into barriers for adoption of HIT in the LTC setting. A longitudinal study into the effectiveness of HIT at reducing medication errors across multiple forms of LTC facilities would be a beneficial addition to existing knowledge. Another beneficial study would be to compare an array of various forms of HIT at improving medication safety across similar healthcare facilities.
Footnotes
Conflict of interest
The authors report no conflicts of interest in this work.