
Abstract
BACKGROUND:
The design and manufacturing of effective foot orthoses is a complex multidisciplinary problem involving biomedical and gait pattern aspects, technical material and geometric design elements as well as psychological and social contexts. This complexity contributes to the current trial-and-error and experience-based orthopedic footwear practice in which a major part of the expertise is implicit. This hampers knowledge transfer, reproducibility and innovation.
OBJECTIVE/METHODS:
A systematic review of literature has been performed to find evidence of explicit knowledge, quantitative guidelines and design motivations of pedorthists.
RESULTS:
17 studies have been included. No consensus is found on which measurable parameters ensure proper foot and ankle functioning. Parameters suggested are: neutral foot positioning and control of rearfoot motion, maximum arch, but also tibial internal/external rotation as well as a three point force system. Also studies evaluating foot orthoses centering on the diagnosis or orthosis type find no clear guidelines for treatment or for measuring the effectiveness.
CONCLUSIONS:
A gap in the translation from diagnosis to a specific, customized and quantified effective orthosis design is identified. Suggested solutions are both top-down, fitting of patient data in simulations, as well as bottom-up, quantifying current practices of pedorthists in order to develop new practical guidelines and evidence-based procedures.
Keywords
Introduction
The design and manufacturing of an effective foot orthosis is a complex multidisciplinary problem involving biomedical and gait pattern aspects, technical material and geometric design elements and psychological and social contexts. The International Classification of Functioning, Disability and Health (ICF) has been developed to standardize the process of tackling this problem by describing it in terms of anatomical functioning, activities, and participation [1]. In the Netherlands the “Process description Medical Devices” has been developed to describe the necessary steps to obtain an effective orthosis [2]. This review is a search for evidence-based knowledge and quantitative guidelines in the design of effective and efficient functional orthopeadic footwear.
The process starts with the client and her problem followed by the intake and assessment, in which the care demand is defined. This important step involves an amount of interdisciplinary perspectives mentioned above and should result in the expected value of the healthcare solution. Deschamps et al. [3] categorizes the expected value of the healthcare solution constructed from three intertwined domains, primary clinical strategy (biomarkers, clinical meaningful endpoints, and surrogate endpoints), secondary clinical strategy (patient-therapist relationship, therapist and patient’s features, treatment features) and thirdly the foot orthotic design practice (physical properties, geometric features, visual properties) [3]. These domains are also reflected in the six steps of the history taking [4] 1) administrative, 2) medical diagnosis, 3) specific complaint and disability (pain, instability, walking skills), 4) use of other medical aids, 5) general health status, 6) social activity and participation. If the solution for the demand for care is an orthosis, the results of these analysis determine the conditions and the design requirements [4].
In the process of defining the design requirements, the pedorthist makes many implicit decisions based on experience and expertise. In every step of the process of anamnesis, from diagnosis, to care plan, to fitting, to manufacturing and delivery [2] relevant patient information is translated into decisions. Experienced practitioners do this in a holistic way, taking all available information into account and implicitly weighing what is most relevant for what purpose. What information is used and relevant for which decision is not tangible and explicit.
Moreover, a large part of the requirements is described in qualitative terms. This is the case for all psychological and social aspects, but also for many biomedical and gait aspects. Apart from the geometric contours of the foot, ankle and leg, all other parameters measured are generally described qualitatively. From a design perspective the many different variables that need to be considered are not numerically defined upfront and thus can’t be quantitatively evaluated afterwards. This complexity is an important contributor to the fact that the orthopedic footwear practice has evolved in a profession based on trial-and-error and experience in which a major part of the knowledge is implicit.
There are a couple of important drawbacks of this implicit way of working. The first is that this type of knowledge is difficult to transfer to new generations of practitioners. The experienced practitioner knows intuitively which of the multiple variables effect which choice in what way. It takes years for an inexperienced fellow to build up that same level of expertise. The second drawback is that this way of working can hamper innovation. The experienced practitioner knows what works and what doesn’t only if he follows the same procedure. For fully new procedures, this expertise has to build up from scratch. For instance, technical innovations like digitalization require numerical values and exact definitions of measures and material properties in design and construction. When exact geometric and functional properties and forces are known, the manufacturing itself becomes subordinate. That itself could also open ways to new innovative materials or construction applications in the manufacturing. However, this can’t be used if the design and construction parameters and the variables affecting those are not exactly quantified.
Search string and Inclusion and exclusion criteria used in this study
Search string and Inclusion and exclusion criteria used in this study
Another drawback is the reproducibility. The implicit knowledge and experience base differs from one practitioner to the other. This means that the same information can lead to different decisions depending on the practitioner one is dealing with. Lastly, it hampers the building up of evidence-based procedures. If one doesn’t explicitly know which rationale has led to which decisions and outcome, the decision-making process can’t be compared between colleagues and procedures can’t be discussed and optimized to best serve clients. Insurance companies are forcing this kind of evidence-based practice upon the profession. For that appropriate measurement tools are required.
Description of the literature search and evaluation process.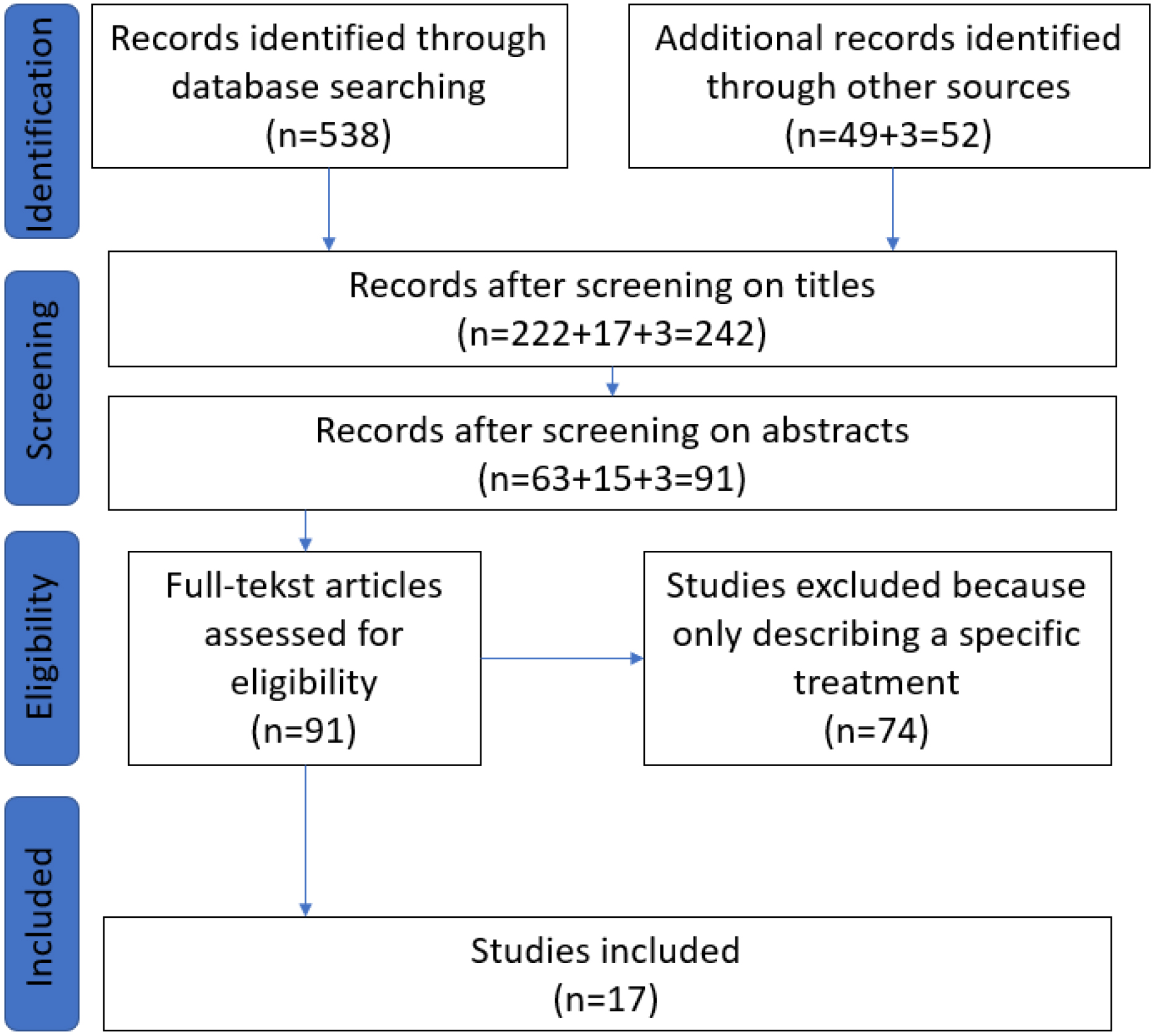
To open up the orthopedic practice for technological innovations and evidence-based practice, it is necessary to make the implicit knowledge of the orthopedic practitioner more explicit. This requires a thorough analysis of the actions of the practitioner during the fitting process, the step that creates the design of the orthosis. However, it also requires an analysis of the motivations of these actions, since quite a number of the actions are motivated by the results of the previous step, and the diagnosis. And lastly the choices and decisions made in the translation to manufacturing should be made explicit.
The SmartScan project executed by Fontys University of Allied Health Professions and partners aims at enabling these technological innovations by developing a smart glove [5]. This glove digitally captures both the geometric contours and the pressures exerted by the orthopedic practitioner and thus makes the fitting actions measurable and explicit. The thus obtained digital representation not only shows a 3D- geometry but also crucial information on the forces required for the correction. It is developed to ultimately replace the currently common used casting method, which is laborious, time consuming, environmentally unfriendly and less reproducible.
In line with this development, a review of literature has been performed to find evidence of explicit knowledge, quantitative guidelines and motivations for actions of pedorthists, based on the following questions: a) What knowledge base is available for the actions of orthopedic footwear experts? b) Which identified variables affecting orthoses design are quantified and measurable with respect to their influence on orthosis design and customer value?
The Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) [6] was used in order to present results in a full and transparent way and to minimize bias. No study protocol was registered.
Search methodology
Using the PICO scheme free text keywords were defined. A computerized search was conducted in January 2022, using the databases Medline via Pubmed. Major search terms are represented in Table 1. Relevant gray literature was derived via Google Scholar and from reference lists of earlier studies on the subject done at the department of Allied Health Professions of Fontys University of Applied Sciences in Eindhoven. Furthermore, reference lists of included studies were checked for relevant literature.
Study selection
All studies describing the process of fitting and designing orthopedic or ankle-foot orthoses were eligible for inclusion, including case studies and popular articles. Also, studies describing the professional acts and the thought processes and considerations of the practitioners were included. Excluded were studies evaluating surgical interventions or studies which only described the effect of an orthosis without describing the process and decisions made in its design.
We limited the search to publications dated from after 1990. Publications before that date are considered too old to be state-of-the-art. All inclusion and exclusion criteria are shown in Table 1.
Titles and abstracts from all search results were assessed to identify eligible studies. From the selection of potentially relevant articles full reports were obtained and in- and exclusion criteria were assessed.
Data extraction and methodological quality
Data from each study included in this review was independently extracted by two reviewers. Data were extracted into standardized tables, including author, publication year, title, abstract selection quote and a categorization according to the disorder or diagnosis. Upon further examination studies assessing the effect of an orthosis for a specific disorder were excluded, because their findings can’t be translated into general principles and guidelines.
Results
Description of the included studies
The initial search identified 538 studies and 52 studies from other sources. After title and abstract screening 91 studies remained. These were further categorized into whether or not they only handled about a specific diagnose or treatment or described the process of fitting and manufacturing of orthosis also in general. After this selection 17 studies remained and were included.
Value of an orthosis
Three studies examined the process of valuing of a foot orthosis from a top-level perspective [3, 7, 8].
The group of Deschamps et al. [3] developed a model, The VALUATOR model, that takes a broad view of the process of the foot orthosis practice. This model explicitly takes into account the client-expert relationship and his expectations regarding the orthosis. The actual fitting and fabrication of the orthosis is only a part of this process. The model identifies six key areas in which outcome observations should be made: 1) value, 2) customer-centered approach, 3) zone of optimal bio-psycho-social stress, 4) bio-psycho-social testing, 5) monitoring, 6) primary and secondary clinical strategies.
Brehm et al. [7] notice insufficient evidence-based knowledge in the practice of fitting and evaluating orthoses on the lower legs. They suggest a method starting from an overview of concepts needed to evaluate orthoses using the ICF, making a distinction between the effectiveness of the orthosis (does it do what it should do under the given conditions) and the effectiveness for the patient (to what extent has this helped the patient). Depending on the orthosis and care demand a different set of intervention-related concepts and patient-important concepts are relevant. These Core-Sets can then be coupled to specific parameters that should be measured and tested for that condition. The tests and measurements quantify the requirements and give a tool to evaluate effectiveness both of the orthosis and for the patient. The measurement methods and qualification criteria should be agreed upon between experts.
A nested decision scheme is ideally used in clinical practice. Decision 1 results in a tentative orthotic intervention with goal setting at ICF Activity level. Decision 2 is based on gait analysis and physical examination and concludes which specific technical requirements the orthosis should fulfil to effectively influence the ICF function level. These two decisions comprise the treatment algorithm. Evaluation is at two levels again, A: Activity level, that should match treatment goal setting, and M: Mechanical evidence that is necessary additional information to evaluate the correctness of the treatment algorithm (dashed line e). Taken from reference [8]. J. Harlaar et al., ‘Studies examining the efficacy of Ankle Foot Orthoses should report activity level and mechanical evidence,” Prosthet. Orthot. Int., vol. 34, no. 3, pp. 327–335, 2010.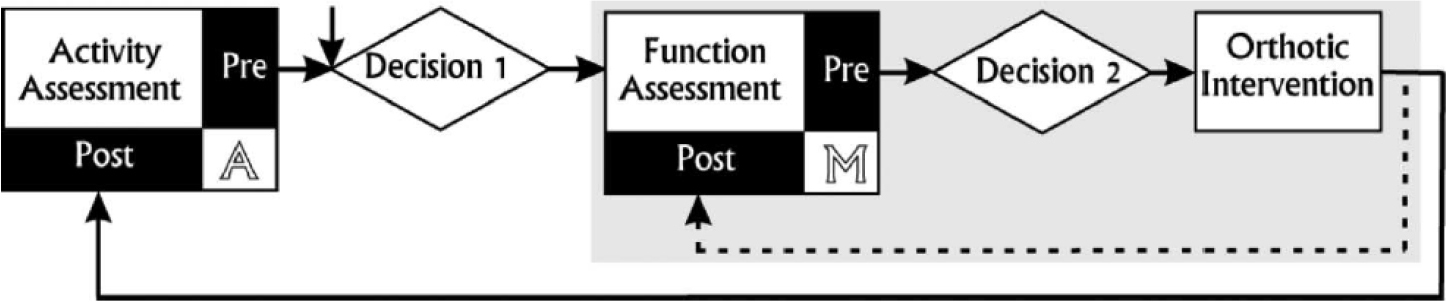
Harlaar et al. [8] state that according to the ICF effectiveness can be measured at the level of functionality, activity and participation. Many studies measure either functionality (mechanical evidence, 3D gait analysis) or activity (stability, walking speed, walking power, walking energy). But one is not always an unambiguous predictor of the other. Mechanically it should be possible to unambiguously and objectively characterize AFOs. This can be done by quantifying the behavior in mechanical terms around the talocrural joint, stiffness and neutral angle, also taking into account the effect of the shoe. For some of these decisions, the measuring instruments from the clinic are not yet useful in daily orthopedics practice. Zooming into the function of the orthosis, most orthoses are aimed to regain or maintain normal foot functioning.
The foundation for current orthopedic foot practice seems to have been laid by Merton Root [9, 10]. He determined and defined neutral positions of joints in the foot and correlated derogations of these neutral positions with abnormalities and pathologies. Treatments aim to correct the foot in a neutral rotation position around the subtalar joint. His Static Biomedical Exam includes 17 measurements that should show which corrections are necessary. An efficient orthosis should correct this position and support the rearfoot-motion [10].
Jarvis et al. [11] challenge this Root model by showing that it is not a valid description of foot functioning or the testing of foot functionality and therefore not a valid basis for clinical evaluation of the foot and the prescription of orthoses. In their study, they evaluated the presence of 5 deformities defined by this ’Root model’ and their effect on the gait pattern in 100 symptom-free participants. All participants had two or more deformities according to the Root criteria, but none of these effected their gait pattern.
Ball et al. [10] argue that the neutral position defined by Root is not neutral but in fact favoring supination. They also find no evidence that an orthosis helps to control the motion of the rearfoot. In their work they review scientific studies to identify potential mechanisms that define the success of an orthosis. In studies with healthy participants 16 measurements of the Root Static exam could not be correlated with dynamic rearfoot motion. The only measurement showing a positive correlation was the measurement, described as the “difference in navicular height”. This measurement, specifically created by McPoil and Cornwall [12] quantifies the changes that occur in navicular height when a subject stands first in a weight-bearing subtalar neutral position and, second, in a relaxed standing position.
Studies of Chuter et al. [13] also show a lot of variation in the correction and therewith in the definition of the neutral position, between different pedorthists and within the same person. This study examined the variation of the cast made of the same foot in a neutral position between experienced and inexperienced OT-ers and of 1 OT-er making the same cast 10 times on the same foot. There appears to be a 16.5∘ variation in the relationship between forefoot and hindfoot (from 10∘ eversion to 6.5∘ inversion). But the researchers state that this should not pose a problem for the result of the orthosis.
Another study of Lee et al. [14] shows that when the forefoot and hindfoot are properly aligned, it doesn’t matter what you do with the angle of the subtalar joint. In 20 patients, various corrections were made to the subtalar joint, 4∘ eversion, 2∘ eversion, 2∘ inversion, and neutral. These cause significant changes in volumes, but no significant changes in parameters like arch height and navicular height.
Glaser et al. [15] note that the classical model of Merton Root is based on a foot movement around only 1 axis. They argue that this is an oversimplified representation of reality. Based on a thorough analysis of the biomechanics of the foot during the gait cycle they come up with a postural model to best prevent postural collapse and control foot function. In their Maximum Arch Supination Stabilization (MASS) posture model arch height is the most crucial aspect when designing an orthosis [15, 16]. They propose a foot orthosis that acts as a composite leaf spring. This composite spring applies an even distribution of force per unit area by remaining in full contact with the foot throughout the gait cycle. The shape of the leaf spring is achieved by the highest “arch” position in stance, with heel and forefoot touching the ground. The stiffness is determined by a combination of weight, flexibility of the foot (5-point scale) and activities of the user.
Ball et al. [10] also argue that simple planar analysis, hindfoot inversion/eversion, is insufficient to study the nuances of foot and ankle during functional activity. The subtalar joint provides movement in 3 planes: “subtalar pronation/supination is said to be composed of eversion/inversion in the frontal plane, medial/lateral rotation in the transverse plane, and a small amount of plantarflexion/dorsiflexion in the sagittal plane.” He concludes from his review that measuring tibial internal/external rotation is a better indicator of foot and ankle function than hindfoot inversion/eversion, especially with regard to effects of foot type and use of orthoses.
Quantification of parameters
Quantification of parameters in foot orthosis design seems to be most prominent in ankle foot orthoses (AFOs). Common indications for prescribing an AFO are excessive knee flexion, hyperpronation, and valgus stress at the knee, where the AFO functions to stabilize, correct and immobilize. Design variables are: data collection and impression techniques, sagittal alignment of the orthosis-shoe combination, footplate length of the AFO, lateral and medial trim lines of the AFO, and placement considerations. However, it is difficult to determine which of these variables determine the effectiveness of an AFO for specific clinical conditions [17].
A diagram shows relative tibial shank alignment. The ankle angle of the AFO (AAAFO) is the relationship between the tibial section and footplate of the AFO. The shank angle to vertical (SVA) is the position of the tibial hank relative to the force of gravity acting vertically. The shank angle to the floor (SAF) is the position of the tibial shank relative to the floor. Taken from reference [17]. B. S. Malas, “What variables influence the ability of an AFO to improve function and when are they indicated?,” Clin. Orthop. Relat. Res., vol. 469, no. 5, pp. 1308–1314, 2011.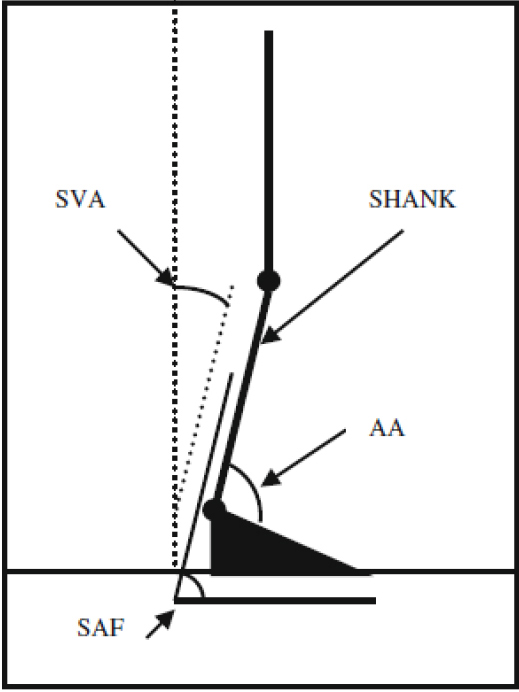
A diagram shows the appropriate three-point force system provided by an AFO to reduce hyperpronation. Taken from reference [17]. B. S. Malas, “What variables influence the ability of an AFO to improve function and when are they indicated?,” Clin. Orthop. Relat. Res., vol. 469, no. 5, pp. 1308–1314, 2011.
Malas et al. [17] endorse the importance of taking into account multiple axes when fitting an AFO. They state that aligning the AFO with the patient in the shoe has the greatest impact. Full and semi-loaded examinations prior to making imprints for rotational deformities are required to determine how much the deformity can be corrected by manual manipulation and prevent over- or under-correction. The focus should be on stabilizing the proximal joints of the lower leg and ensuring good postural alignment (bottom leg-floor angle 10–12 degrees). See Fig. 3. Footplate length affects ankle mobility and the lateral and medial trim lines must keep the foot in proper alignment. This is most effective if they provide a 3 point force system, see Fig. 4.
In Scotland a Best Practice Statement for the fitting of an Ankle Foot Orthosis is developed by Bowers et al. [18] that takes into account measurable biomedical and gait aspects as well as social aspects such as user perception and effects on daily functioning.
Arch et al. [19] investigated the relation between AFO-stiffness and muscle-activity, to conclude that AFO mainly compensates weak uniarticular soleus function and doesn’t effect biarticular medial gastronemicus function. This results in a negative effect on the knee acceleration in stance, that can be a trigger for new AFO-designs.
Several reviews indicate that the effectiveness of ankle-foot orthoses and orthoses is, to say the least, debatable [20, 21, 22, 23]. This is often due to the low quality of the studies, the different methods of measuring and evaluating the orthoses, and the often-occurring lack of crucial information regarding the rationale behind the choice of intervention. There are no clear guidelines for treatment and for measuring the effectiveness of treatment for many disorders.
In a review of 13 studies, Hill et al. [21] describe the orthopedic measures taken to correct five different disorders in children (pes planus (
Smythe et al. [24] describe the consensus on 4 general criteria for assessing the treatment of clubfoot in Africa (18 practitioners, 10 African countries). These are so general, that they can’t be used as parameters for the design of an orthosis: the foot is plantigrade, the child can wear a normal shoe, the child reports no pain, the care provider is satisfied.
Discussion
The process of design and manufacturing orthopedic footwear has a clearly established purpose on a high level: to create satisfied patients that use their orthopedic footwear when needed. Patient satisfaction is a multi-faceted phenomenon as is described by Deschamps et al. [3]. The fitting and fabrication process of the orthosis is only a small portion of this process. Zooming in on this portion the purpose of a foot orthosis is well-defined: to aid in the ability to stand and walk, preferably pain-free and without it costing too much energy. However, the ability to stand and walk is dependent on a complex ingenious interplay of bones, joints, tendons, muscles and nerves that is highly characteristic for each individual. There is no consensus on what the best measurable parameters are to ensure proper foot and ankle functioning.
The Root model [9], focusing on neutral foot position and rearfoot motion has been challenged as not generally applicable. Glaser [15] proposes an alternative MASS model that centers maximum arch as the main parameter to ensure effectiveness of an orthosis. Ball et al. [10] suggests tibial internal/external rotation as a better indicator of foot and ankle function. Malas et al. [17] stress the importance of taken into account multiple axes and a three-point force system, when designing an orthosis.
Reviews show that studies that compare or evaluate foot orthoses by centering on the diagnosis or on the type of orthosis find no clear guidelines for treatment and for measuring the effectiveness of treatment for many disorders [20, 21, 22, 23, 24]. Looking from a wider perspective this is not strange, because every human gait cycle is different, dependent on highly individual bone and joint structures and its interplay with muscles and nerves. Malfunctioning in this chain can have many causes and thus, there are many cures.
From a mechanical point of view, the decisions being made are customized combinations of immobilization, correction, support and cushioning tailored to specific parts of the foot. Overall, this should lead to improved walking and standing ability of that specific patient. In general, for each joint, an experienced practitioner knows how to correct position, stabilize or support. However, because each human gait is different, each disabled gait will need different combinations of these measures on different locations for an efficient orthosis.
The implicit knowledge used by the practitioner is the translation of the information from gait analysis and patient assessment into specific customized improvement measures, specified per foot location. Quantification of these measures will be highly dependent on the individual patient, but also on the individual practitioner. There is no generally applicable quantitative measure or parameter that ensures proper gait and foot functioning, no objective definition of ‘what is good?’
Therefore, there still appears to be a gap in available tools required to make the translation from the diagnosis to specific, customized and quantified design requirements for an effective orthosis. Solutions to bridge this gap might be top-down, coming from computer simulations fitting detailed foot and biomechanical models to specific patient and gait information and analyzing effects of quantified correction measure designs on gait patterns through simulation, before manufacturing. Or they may be bottom-up, analyzing and quantifying current practices of orthopedic shoe practitioners in order to develop new practical guidelines and evidence-based procedures as is being attempted in the SmartScan project e.g. [5].
Author contributions
CONCEPTION: F. Holtkamp, Y van Zaalen, T. Sonderkamp.
PERFORMANCE OF WORK: T. Sonderkamp, F. Holtkamp.
INTERPRETATION OR ANALYSIS OF DATA: T. Sonderkamp, F. Holtkamp.
PREPARATION OF THE MANUSCRIPT: T. Sonderkamp, F. Holtkamp.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: F. Holtkamp, T. Sonderkamp, Y van Zaalen.
SUPERVISION: F. Holtkamp, Y van Zaalen.
Ethical considerations
This study, as a literature review, is exempt from Institutional Review Board approval.
Footnotes
Acknowledgments
This research was funded by SIA-RaaK grant number RAAK.MKB12.032.
The authors would like to acknowledge Geert-Jos van der Maazen for his contribution to the project.
Conflict of interest
The authors have no conflicts of interest to report.