
Abstract
BACKGROUND:
Physical activity as one of the major lifestyle-related health determinants is partially addressed by the Montreal Walking Exoskeleton Satisfaction and Perspectives-Questionnaire (MWESP-Q).
OBJECTIVE:
To document satisfaction of people with chronic spinal cord injury after the completion of a 10 to 16 weeks of the wearable robotic exoskeleton-assisted walking program, with the MWESP-Q updated to a context of health promotion.
METHODS:
Following a walking program (10–16 weeks), wheelchair users with chronic SCI completed the MWESP-Q online. Modification of the original questionnaire was conducted with 4 experts to ensure its content validity with a human framework to promote physical activity for health.
RESULTS:
Ten wheelchair users completed the questionnaire (men
CONCLUSIONS:
The updated MWESP-Q is now better equipped to measure physical and cognitive efforts in physical activity and changes in body and organic systems and in capabilities (health promotion). The updated MWESP-Q has 54 statements (14 additional statements and 1 deleted) organized around seven domains. The original measure was replaced by three 7-point Likert scales, one regarding agreement level (40 statements), level of effort (12 statements), and level of change (2 statements).
Keywords
Introduction
There is a growing body of research on the use of wearable walking exoskeletons in rehabilitation (e.g. spinal cord injury), with most focusing on walking performance [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15]. The current technology (wearable robotic exoskeleton (WRE)) is not widely available in the community or in gyms, and current exoskeletons generally require the assistance or supervision of a specially trained therapist (and a walking aid) for sit-stand transfers and safe ambulation. A satisfaction questionnaire was developed to assess user-perceived outcomes in a pilot research project in 2018 [8]. The Montreal Walking Exoskeleton Satisfaction and Perspectives – Questionnaire (MWESP-Q) comprised a total of 41 statements that were organized around seven key domains [8]. Gagnon and colleagues had used the MWESP-Q with 14 wheelchair users with SCI who finished a 6 to 8-week exoskeleton-assisted walking program. All statements were phrased in a positive manner using an electronic cursor on a horizontal and continuous 100-mm long visual analogue scale. At one extreme, 0% would indicate Totally disagree and at the other extreme, 100% would indicate Totally-completely
agree. Results were presented for all statements in % with standard deviation: overall satisfaction related to the training program (2 statements, mean
Project-specific logic model highlighting the relationships between the different domains of interest and related outcome measures. L/E: lower extremity; SCI: spinal cord injury; U/E: upper extremity; WRE: wearable robotic exoskeleton. Reproduced with the permission of JMIR Res Protoc 2020, 9(9), p. 7.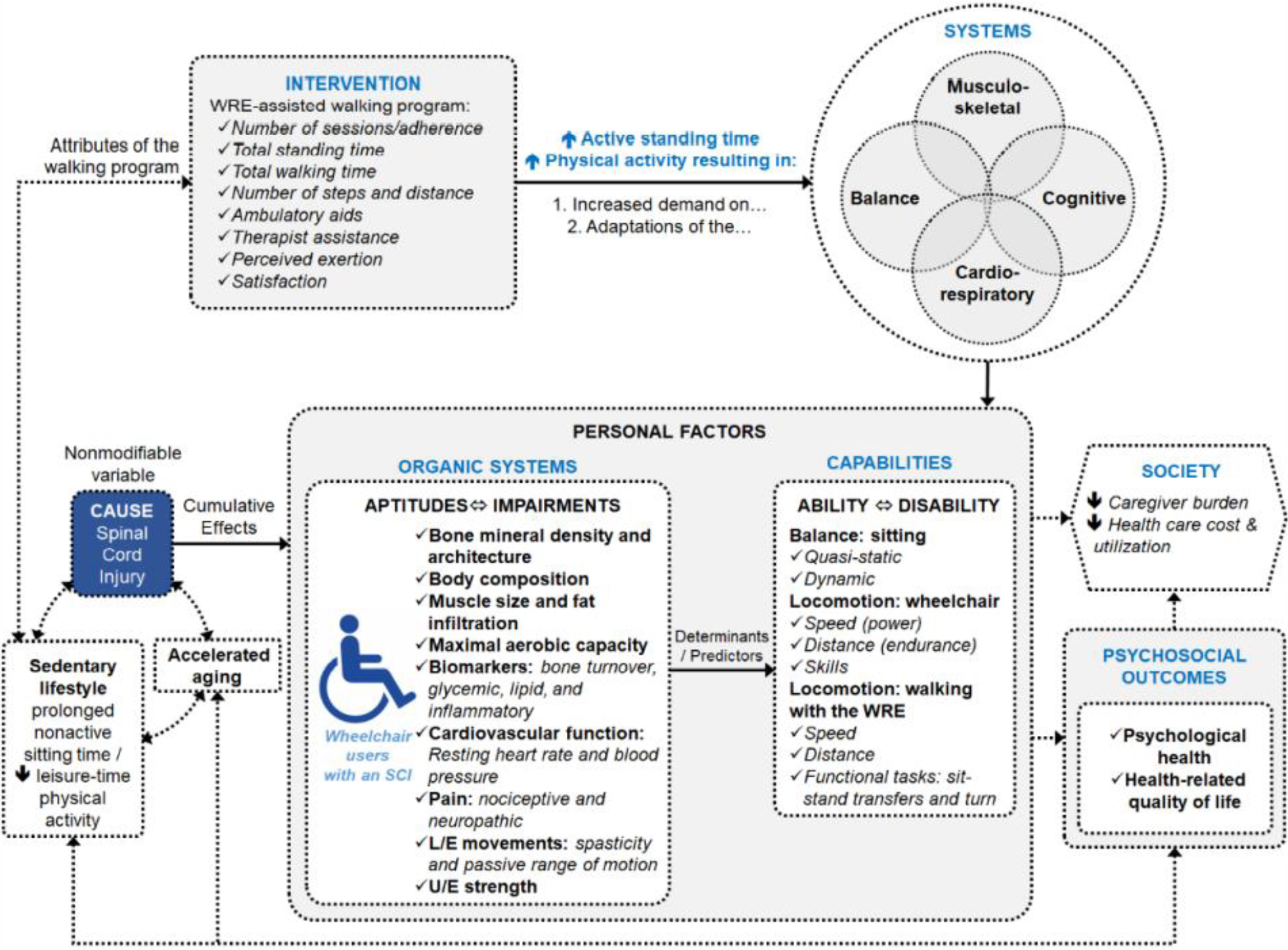
Given a new walking program with more attributes associated to health promotion, i.e. closer to adapted physical activity programs offered in rehabilitation or other specialized centers, it has become necessary to update the MWESP-Q. The protocol for the present study has been published previously in JMIR Research Protocols [16] as ‘Effects of an Overground Walking Program With a Robotic Exoskeleton on Long-Term Manual Wheelchair Users With a Chronic Spinal Cord Injury: Protocol for a Self-Controlled Interventional Study’. The questionnaire had to be updated according to a logic model in the published protocol and is reproduced here with permission (Fig. 1) [16, p. 7].
In lower left, sedentary lifestyle is prolonged nonactive sitting time and decreasing leisure-time physical activity, following a spinal cord injury. In upper left, a WRE-assisted walking program with additional attributes will increase active standing time and will increase physical activity; this will increase demands or results in adaptations of the bodily systems (musculoskeletal, cardiorespiratory, cognitive, balance, cognitive). This will possibly result in measurable effects on organic systems (e.g., bone mineral density, maximal aerobic capacity, pain) and capabilities (e.g., balance sitting, locomotion with wheelchair and the WRE), central of Fig. 1. In turn, these adaptations may impact the society and produce psychological outcomes, right of Fig. 1. It was necessary to add statements to the MWESP-Q [8] to better emphasize health promotion regarding the attributes of the program, physical activity in society and psychological impacts as well to measure statement agreement level more accurately, the level of change and the level of effort.
Given this twofold rationale (new program and need to assess it), the research objective was to document satisfaction of people with chronic spinal cord injury after the completion of a 10 to 16 weeks of the wearable robotic exoskeleton-assisted walking program, with the MWESP-Q updated to a context of health promotion. According to our published protocol [16], the objective should answer this research question “What are the participants’ satisfaction levels with the walking program and the wearable robotic exoskeleton itself?” It was hypothesized that wheelchair users with a chronic spinal cord injury would express high levels of satisfaction with the walking program using the wearable robotic exoskeleton and with the wearable robotic exoskeleton itself.
Method
Research design
A cross-sectional quantitative design (online questionnaire) was conducted in the retention phase of the study [16], within three weeks of discontinuing or completing the WRE walking program. This study was initiated at the Laboratoire de pathokinésiologie in the Centre de recherche interdisciplinaire en réadaptation du Montréal métropolitain (CRIR), Québec, Canada, which is part of the Centre intégré universitaire de santé et de services sociaux du Centre-Sud-de-l’Ile-de-Montréal in Montreal, Canada, and at the Laboratoire du muscle et de sa fonction of the Université du Québec à Montréal.
Sample and recruitment
In this study, participants were recruited to participate in an exoskeleton-assisted walking program consisting of 34 sessions (60 min/session, 1–3 sessions/week) [16]. Questionnaires and tests were used to document the intervention and personal factors presented in the logic model [16]. As stated in the published protocol, after sample size calculation, we aimed to recruit a non-probabilistic sample of 20 participants in this study [16]. Briefly, to be included, individuals needed to use a wheelchair as their primary mode of locomotion, be able to understand French or English, and reside (or be able to arrange to reside) within 75 km of the main research site. Individuals were excluded if they had neurological impairments unrelated to the spinal cord injury (e.g., multiple sclerosis), had a concomitant or secondary musculoskeletal impairment limiting their ability to safely ambulate (e.g., hip heterotopic ossification), had a history of fragility fracture within the past year, or any other condition that may preclude safe lower extremity weight-bearing, walking or exercise tolerance (e.g., unstable cardiovascular or autonomic system, renal insufficiency, etc.). Individuals also had to meet criteria specific to the wearable robotic exoskeleton (Ekso GT, Ekso Bionics) used in this study, including anthropometric measures and lower- and upper-extremity range of motion. Inclusion and exclusion criteria are described in detail in the published protocol [16]. Recruitment and interventions began in 2019 but were very much restrained due to the pandemic over the past 2 years. Due to time constraints and funding concerns, the study was not resumed after 2021. Unfortunately, this led to many participants being unable to complete the entire 16-week walking program. We therefore asked all participants who had completed or nearly completed the wearable robotic exoskeleton (WRE) walking program (10 to 16 weeks) to answer the updated version of the MWESP-Q. Out of a possible 15 participants, 66% (
Intervention with the exoskeleton
The overground robotic exoskeleton used in this study was the Ekso GTTM, manufactured by Ekso Bionics® (
Updating the MWESP-Q to a context of health promotion
In psychometrics, modification of an original questionnaire refers to content validity. Content validity primarily relies on the expertise of individuals familiar with the construct being measured [17]. These subject-matter experts are usually provided with access to the measurement tool and are asked to provide feedback on how well each question measures the construct in question. From the three key aspects of content validity (domain definition, domain representation, and domain relevance) [17], the second one was of interest for the study. Two research team meetings were devoted to the modifications to the original questionnaire to get a consensus on the statements to be added, removed or modified. Discriminant measurement scales were adopted depending on the domains of the MWESP-Q, for a total of three different scales. From the research team, there were four experts included two physiotherapists (AB, DHG), one occupational therapist (CV) and one kinesiologist (FB, see Acknowledgments). They revised all questions of the MWESP- Q and formulated new questions according to Fig. 1 (Project-specific logic model highlighting the relationships between the different domains of interest and related outcome measures) which is consistent with the European framework for physical activity [18].
The upgraded MWESP-Q includes 13 new statements for a total of 54. Items were added for four of the seven key domains: satisfaction with the robotic exoskeleton (
Data analysis
Descriptive analyses were conducted on the sociodemographic and clinical variables and on all statements (7-point Likert scales) included in the MWESP-Q. All statistics were perform using Excel. The seven key components (domains) are presented as means and standard deviations to help interpret the score according to the 7-point Likert scales. Furthermore, medians were also calculated for all statements.
Baseline characteristics of the study participants (
10)
Baseline characteristics of the study participants (
Participants
Table 1 presents the baseline characteristics of the participants (
User’s satisfaction (scale 1 to 7) regarding the exoskeleton and exercise training program (
10)
User’s satisfaction (scale 1 to 7) regarding the exoskeleton and exercise training program (
*1
Since the MWESP-Q is organized around seven key domains, results are presented for each domain with more details in three tables. Please note that there are three possible response scales, and they are always specified at the bottom of the tables. In Table 2, three domains are presented. Overall, participants
User’s satisfaction regarding the exoskeleton and exercise training program (
10)
User’s satisfaction regarding the exoskeleton and exercise training program (
*1
In Table 3 two domains are captured with two different Likert scales. Participants
User’s satisfaction regarding the exoskeleton and exercise training program (
*1
The last two domains are presented in Table 4 with two different Likert scales. In general, participants reported a
The study objective has been achieved. The research question has been answered, since participants’ satisfaction levels with the walking program and the wearable robotic exoskeleton itself have been documented in 54 statements (with the updated MWESP-Q). Our hypothesis was partially confirmed: 10 wheelchair users with chronic SCI expressed high levels of satisfaction with the walking program using the wearable robotic exoskeleton and with the wearable robotic exoskeleton itself, but only in four key components of the updated MWESP-Q. Participants expressed their satisfaction as that they “strongly agree” in satisfaction domain (over 6.5/7) and “agree” in domains of exoskeleton, learnability, and motivation to engage in physical activity (from 5.5 to 6.5/7). Regarding risks and fears domain of risks and fears, it appears that participants expressed they somewhat disagreed or disagreed with 8 of the 11 statements, which seems to be a good feeling when the fear is moderate, compared with none at all or being extremely afraid. Finally, in the domains of program and of perceived health benefits of WRE, wheelchair users had reported “medium effort” for the general perceptions of physical and cognitive exertion during the training sessions, as well as “neutral and light improvements” in the 12 outcomes at the end of the WRE walking program (from 4.4 to 5.7). The relatively small sample size (
Compared to Gagnon et al’s study where wheelchair users finished a 6 to 8-week locomotor exercise program, their results in percentage from a 100-mm long visual analogue scale were more difficult to interpret clinically, such as 67.9%
Strengths and limitations of the study and future research
The strength of this cross-sectional quantitative design lies in its internal validity. In this respect, the survey questionnaire (MWESP-Q) was improved according to the rules of the art of content validity [17], i.e. with experts on the study and dedicated to health promotion, with the theoretical model already published [16, 18]. Also, to address a possible expectancy bias, participants were notified that the questionnaires were administered and analysed by an offsite (based in another city) research professional (FSD) that they had never met. All participants were specifically informed, and reminded on several occasions, that their therapists would not have access to their answered questionnaires. The recruitment of 15 persons was done in one city and had to stop due to the COVID-19 pandemic (3 persons could not answer the questionnaire because they did not complete at least 10 weeks of training, two did not fill the questionnaire). The external validity of the results of this study is therefore limited, given the small sample size (10 instead of 15) in a single location and the fact that only 7 out of 10 people completed 16 weeks of intense training with the walking exoskeleton. Future research is needed to assess satisfaction, health benefits and level of effort in adapted physical activity using next generation exoskeletons in a community context. Since the Ekso GT is now discontinued and replaced by Ekso NR (
Conclusions
This study has documented satisfaction of 10 people with chronic spinal cord injury after the completion of a 10 to 16 weeks of the wearable robotic exoskeleton-assisted walking program, in a context of health promotion. The participants agreed and strongly agreed with satisfaction domain statements as well as ‘exoskeleton, learnability, and motivation to engage in physical activity” domain statements, meaning that they were satisfied with the training program and that they would recommend it to others. After only 10 to 16 weeks of sit-stand transfer training and intensive walking with the assistance of a therapist, users reported light improvements, e.g., arm strength, sitting balance, spasticity in the legs, intestinal elimination, sleep, ability to propel wheelchair and to transfer. They also declared moderate improvements in general endurance and psychological well-being. This study also recommends using the updated MWESP-Q in future research where a walking robotic exoskeleton is used in a health promotion context, i.e., in a context of adapted physical activity to stay fit or to prevent secondary health complications. The original questionnaire of satisfaction (MWESP-Q) was updated to include physical and cognitive efforts in physical activity and changes in body and organic systems and in capabilities, that is part of health promotion, that is fully supported by WHO Europe, since physical activity is one of the major lifestyle-related health determinants [18]. The updated MWESP-Q proposes 13 additional statements for heath promotion in the WRE walking program attributes, in perceived health benefits of walking with the robotic exoskeleton and in perceived fears. The MWESP-Q also now measures level of agreement in seven key components, The level of perceived change and level of effort. original measure (in percentage) was replaced by three 7-point Likert scales, one regarding agreement level (40 statements), level of effort (12 statements), and level of change (2 statements).
Author contributions
CONCEPTION: Dany H Gagnon, Mylène Aubertin-Leheudre PhD, Antony D Karelis, Suzanne N Morin, Michelle McKerral, Cyril Duclos, Claude Vincent.
PERFORMANCE OF WORK: Alec Bass and Frédéric S Dumont for data collection.
INTERPRETATION OR ANALYSIS OF DATA: Frédéric S Dumont.
PREPARATION OF THE MANUSCRIPT: Claude Vincent.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: All.
SUPERVISION: Dany H Gagnon and Mylène Aubertin-Leheudre supervised Alec Bass.
Ethical considerations
This project received ethical approval on March 14, 2019, from the CRIR ethics committee and was registered on June 7, 2019, with the US National Library of Medicine at ClinicalTrials.gov (NCT03989752).
Footnotes
Acknowledgments
Special thanks are extended to Florian Bobeuf for his substantial contribution in the coordination of this project and during the training sessions, as well as Martin Vermette and Manual Escalona for their expertise and assistance with the exoskeleton. Thank you to Manon Rogers and Tiffany Hu, both students supported by the Cirris who have first computed part of the results of the MWESP-Q during the first year of the COVID in 2020. Dany Gagnon and Sara Ahmed co-chair the Initiative for the Development of New Technologies and Practices in Rehabilitation (INSPIRE) funded by the LRH Foundation and co-leads the Rehabilitation Interventions for Individuals with a SCI in the Community (RIISC) research team funded by the Ontario Neurotrauma Foundation and the Quebec Rehabilitation Research Network.
Conflict of interest
The authors have no conflicts of interest to report.