
Abstract
PURPOSE:
This study aimed to examine outpatient hospital utilization (number of specialties seen and number of visits to each specialty) in the year after single event multi-level surgery (SEMLS) in children with cerebral palsy (CP), and to determine if utilization differs across the medical center in the year after compared to the year before SEMLS.
METHODS:
This retrospective cross-sectional study used electronic medical record data of outpatient hospital utilization in children with CP who underwent SEMLS.
RESULTS:
Thirty children with CP (Gross Motor Function Classification System Levels I–V, mean age of 9.9 years) were included. In the year after surgery, a significant difference (p = 0.001) was found for the number of specialties seen, with non-ambulatory children seeing more specialties than ambulatory children. No statistically significant difference was found between the number of outpatient visits to each specialty in the year after SEMLS. Compared to the year before SEMLS, fewer therapy visits occurred in the year after SEMLS (p < 0.001) but significantly more visits to orthopaedics (p = 0.001) and radiology (p = 0.001).
CONCLUSION:
Children with CP had fewer therapy visits but more orthopaedic and radiology visits the year after SEMLS. Nearly half of the children were non-ambulatory. Examination of care needs in children with CP undergoing SEMLS is justified with consideration of ambulatory status, surgical burden, and post-operative immobilization.
Introduction/Background
Cerebral palsy (CP) is a non-progressive disorder of movement and posture following an insult to the developing brain [1] affecting 3.1–3.2 per 1000 births in the United States [2, 3]. Children are often classified by severity of motor function into five levels based on the Gross Motor Function Classification System (GMFCS) [4, 5]. GMFCS levels are defined as Level I (walks without limitations), Level II (walks with limitations), Level III (walks using a hand-held mobility device), Level IV (self-mobility with limitations, which may include power mobility), and Level V (transported in a manual wheelchair) [4, 5]. Due to the associated comorbidities of CP such as pain, hip displacement, epilepsy, intellectual disability, and sleep disorders [6], children often require care from many specialties throughout their lifespan [7]. Although CP is nonprogressive, as children grow, musculoskeletal morphology changes can cause muscle contractures, torsional deformity of the long bones, and joint instability. Historically, yearly single level surgery of soft tissue or bones at one anatomical level was common practice. Currently, the standard of care for children with CP is orthopaedic single event multi-level surgery (SEMLS) defined as one orthopaedic surgical event involving two or more soft tissue and/or bony procedures at two or more anatomical levels during one hospital admission requiring one episode of rehabilitation [8–10]. SEMLS addresses deformities and pain that occur as the child grows, prevents deterioration in function, and improves quality of life [9, 10].
SEMLS can be categorized into high surgical burden or low surgical burden depending on how many bony procedures are performed during the surgery [11, 12]. Low surgical burden is defined as a single osteotomy (cutting of the bone on one leg) and/or any number of soft tissue procedures on one or both legs. High surgical burden is described as two or more osteotomies on one or both legs with any number of soft tissues on either or both legs. There is emerging evidence that surgical burden is associated with outcomes after SEMLS [11, 12] and should be considered when developing post-operative rehabilitation guidelines for care.
While it is recommended that a multidisciplinary team of hospital specialists, including orthopaedics, physical medicine and rehabilitation, and physical therapy contributes to pre-operative decision-making for individuals with CP undergoing SEMLS [13], there is a lack of recommendations for organizing care after SEMLS. An organized approach to care could be particularly useful given that recovery of function after surgery can take from six months [14] to 2 years [15, 16]. The lack of evidence-based recommendations for organizing care after SEMLS contributes to unnecessary variation in care, client dissatisfaction, and poor outcomes [17].
Caregivers report the need for clear information and support from qualified healthcare workers to prepare for the surgery as well as rehabilitation following the surgery [18]. Further, both mental and physical burden have been reported by caregivers during the post-surgical rehabilitation phase after SEMLS [18]. Outpatient hospital utilization during the post-operative period is unknown [10, 13]. Understanding outpatient hospital utilization following SEMLS would provide insight into the coordination and care required for children after SEMLS and identify patterns of care for subgroups of children with CP. This information could be useful to families when planning for upcoming surgery and clinicians when coordinating across specialties within the hospital. Improved coordination of care following surgery may decrease burden, improve satisfaction, and optimize outcomes.
The aims of this study were to [1] examine outpatient hospital utilization (number of specialties seen within the hospital and number of visits per child to each specialty) in the year after SEMLS across ambulatory status and surgical burden categories, and [2] determine if utilization (number of specialties seen and number of visits per child to each specialty) differs across the medical center in the year after SEMLS compared to the year before SEMLS. In addition, the total number of visits in the year after SEMLS compared to the year before SEMLS was examined.
It was hypothesized that in the year after surgery: Children who were ambulatory before surgery would demonstrate higher service utilization than non-ambulatory children, based on the need for ambulatory children to return to prior function. Children with high surgical burden would demonstrate higher service utilization than children with low surgical burden due to the number and type of procedures performed.
Last, compared to the year prior to surgery, it was hypothesized that service utilization in the year after surgery would be greater, as all children would require increased visits to specialties involved with the surgery and rehabilitation to support the child and caregiver during the recovery process.
Methods
This was a retrospective cross-sectional study of outpatient hospital utilization in children with CP who underwent SEMLS. All children were identified from the Department of Pediatric Orthopaedic Surgery clinic list with the diagnosis of CP who underwent SEMLS between October 2017 and June 2018. Demographic information (gender, race [White, Black/African-American, Asian, Biracial/Multi], and ethnicity [Non-Hispanic and Hispanic]), child characteristics (GMFCS Level, spasticity management history [Intrathecal Baclofen Pump, Selective Dorsal Rhizotomy], type of procedure [soft tissue only, bony only, soft tissue and bony], level of procedure [unilateral and bilateral], spasticity management during surgery [Botulinum Toxin, nerve block, combination of nerve block and Botulinum Toxin], surgical burden [low and high], and outpatient in-person visits to the most frequent specialties across the medical center) was extracted from the electronic medical record for a year prior to surgery (year 2016) and the year following each child’s date of surgery. This study defined utilization as the number of specialties seen and the number of visits per child to each specialty. It included specialties if visits to that specialty made up at least 1% of the total visits. Children were categorized according to pre-surgical ambulatory status (GMFCS Levels I–III = ambulatory or GMFCS Levels IV-V = non-ambulatory) and surgical burden (low or high) due to expected differences between groups. Ambulatory status and surgical burden were determined by the authors via manual chart review. The hospital’s Institutional Review Board provided approval prior to conducting this study.
Data analysis
Descriptive statistics were utilized for demographic and clinical characteristics of the children who underwent SEMLS during the study period. A Fisher’s Exact Test was used to assess for an association between ambulatory status and surgical burden categories. For the first aim, the number of specialties seen along with the number of visits per child to each specialty in the year after SEMLS were analyzed. The effects of ambulatory status and surgical burden were assessed separately for the number of specialties seen and the number of visits per child to each specialty in the year after SEMLS using a Wilcoxon signed-rank sum test. Generalized linear mixed effect models were used to examine the effect of ambulatory status, surgical burden, and their interactions on the number of specialties seen and the number of visits per child to each specialty in the year after SEMLS. A child-specific random effect was included to account for potential dependence of the number of visits for each specialty. For the second aim, generalized linear mixed effect models were used to characterize utilization (number of specialties seen and number of visits per child to each specialty) by including time (before and after SEMLS) and specialty interactions with ambulatory status as a confounding factor. Post-hoc comparisons were used to compare the differences in utilization before and after SEMLS for each specialty; Holm’s method was used to adjust for multiple testing for each specialty. The data were analyzed using SAS/STAT® software 9.4 (Cary, NC) and R software [19] version 3.5.3, and the plots were generated with RStudio [20] version 1.4.1717. Statistical results were interpreted at a 95% confidence interval with statistical significance of p < 0.05 (two-tailed).
Results
A total of thirty children with CP were identified as having SEMLS during the study period. See Table 1 for details of child demographics and characteristics. Children were 50% male, 67% White, and 93% Non-Hispanic, with a mean age of 9.9 (3.5 SD, range 3–16) years old at the time of surgery. Ambulatory children made up 53.3% (GMFCS I 10%, II 16.7% and III 26.7%) of the group, while 46.7% were non-ambulatory (GMFCS IV 40%, V 6.7%). The mean number of procedures per child was five (2.3 SD), and for 21 (70%) of the children, surgery was categorized as high surgical burden.
Demographics and characteristics of children who underwent SEMLS
Demographics and characteristics of children who underwent SEMLS
SEMLS: Single event multi-level surgery. GMFCS: Gross Motor Function Classification System.
A preliminary analysis found a statistically significant association between ambulatory status and surgical burden (p = 0.017). Non-ambulatory children were more likely to have high surgical burden than children who were ambulatory (Odds Ratio = 13, 95% CI: 1.36–124.30; proportion of high surgical burden: 92.9% vs. 50.0% for non-ambulatory children and ambulatory children, respectively). The top twelve specialties seen included therapy (combining physical therapy, occupational therapy, and speech language pathology), orthopaedics, radiology, pediatric rehabilitation medicine, neurology, laboratory draws, complex care, ophthalmology, otolaryngology, gastroenterology, neurosurgery, and behavioral psychology (See Table 2). Details for the total number of specialties seen, number of outpatient visits by specialties, and the mean number of visits per child to each specialty in the first year after SEMLS are reported in Table 2 and were examined based on ambulatory status and surgical burden as shown in Figs. 12. A statistically significant difference was found for the number of specialties seen and ambulatory status (p = 0.001). Children who were non-ambulatory saw more specialties (median eight, IQR 6–8) than those who were ambulatory (median four, IQR 3.–5.5). No statistically significant difference was found between the number of outpatient visits per child and ambulatory status (p = 0.383). Also, there were no statistically significant differences between number of specialties seen and surgical burden type (p = 0.218) or number of outpatient visits per child and surgical burden type (p = 0.147).
The number of children seen by each specialty and the total number of visits for the year before SEMLS and the year after SEMLS
The number of children seen by each specialty and the total number of visits for the year before SEMLS and the year after SEMLS
SEMLS: Single event multi-level surgery. †Therapy includes combination of physical therapy, occupational therapy, and speech therapy. *p-value comparing before to after SEMLS in the generalized linear mixed effect model of the number of visits for each specialty per child; Holm’s method used to correct multiple testing.

Number of specialties seen by ambulatory status and surgical burden. The white line represents the median, and top to bottom box signifies the interquartile range. A statistically significant difference was found for the number of specialties and ambulatory status (p < 0.01) using a Wilcoxon signed-rank sum test.
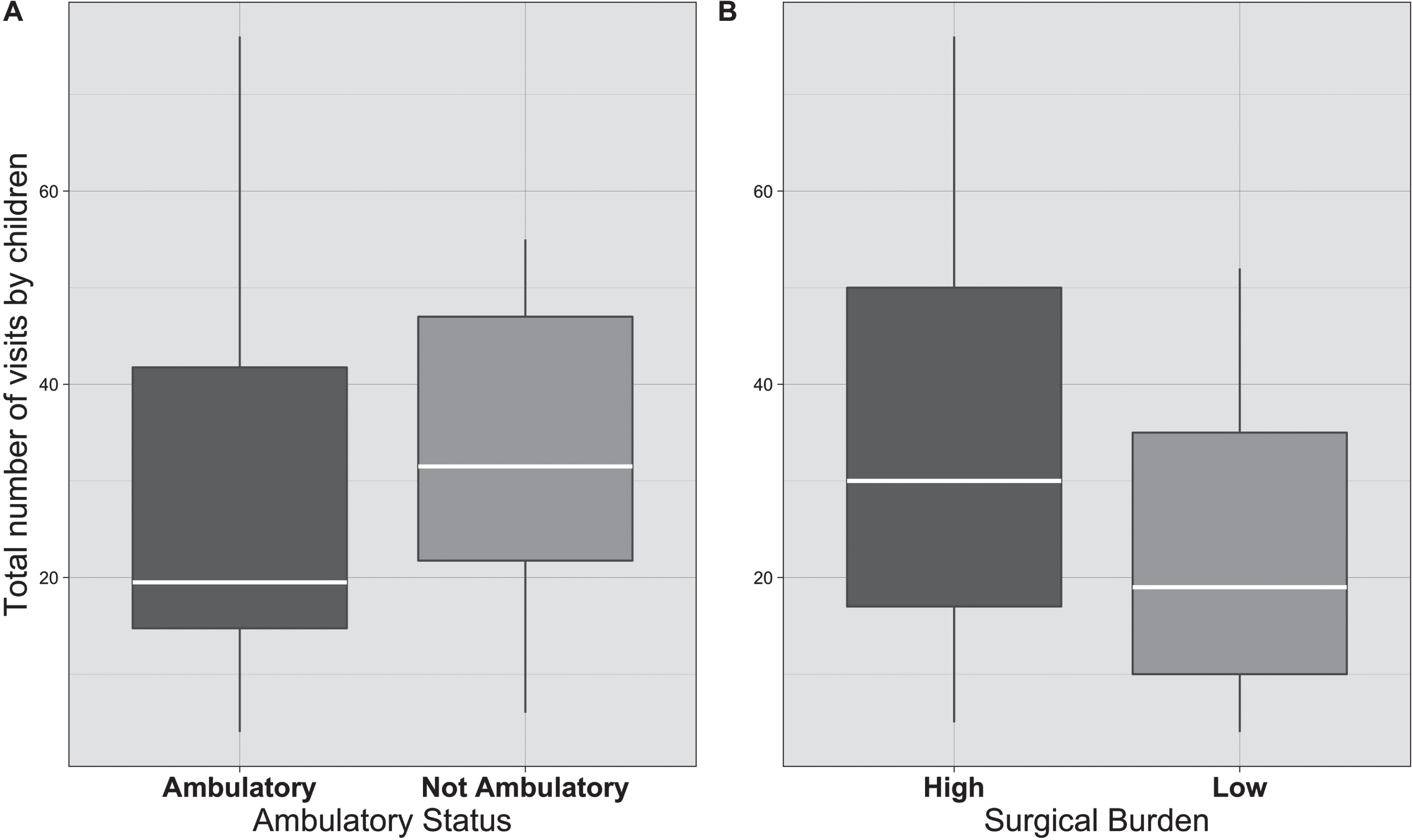
Total number of outpatient visits by ambulatory status and surgical burden. The white line represents the median, and top to bottom box signifies the interquartile range. There were no statistically significant differences between number of specialties and ambulatory status or number of specialties and surgical burden type using a Wilcoxon signed-rank sum test.
Details for the number of specialties seen and visits to each specialty across the medical center for children with CP in the year before and year after SEMLS are presented in Table 2. There was no significant difference in the number of specialties the children saw before SEMLS (median of five, IQR 4–6) compared to the year after SEMLS (median of five, IQR 3–7). The generalized linear mixed model did not reveal a significant interaction between specialty and time (F = 25.61, p = 0.153); however, post-hoc analyses showed children had less outpatient visits to therapy and significantly more visits to orthopaedics and radiology after SEMLS, compared to the year before SEMLS (adjusted p-value = 0.001). See Table 2. The sample of children had a total of 1571 unique outpatient visits the year prior to SEMLS (median 16, IQR 7–61) and 807 unique outpatient visits the year after SEMLS (median 28, IQR 16–49); this difference did not reach statistical significance (p = 0.106) as shown in Fig. 3.
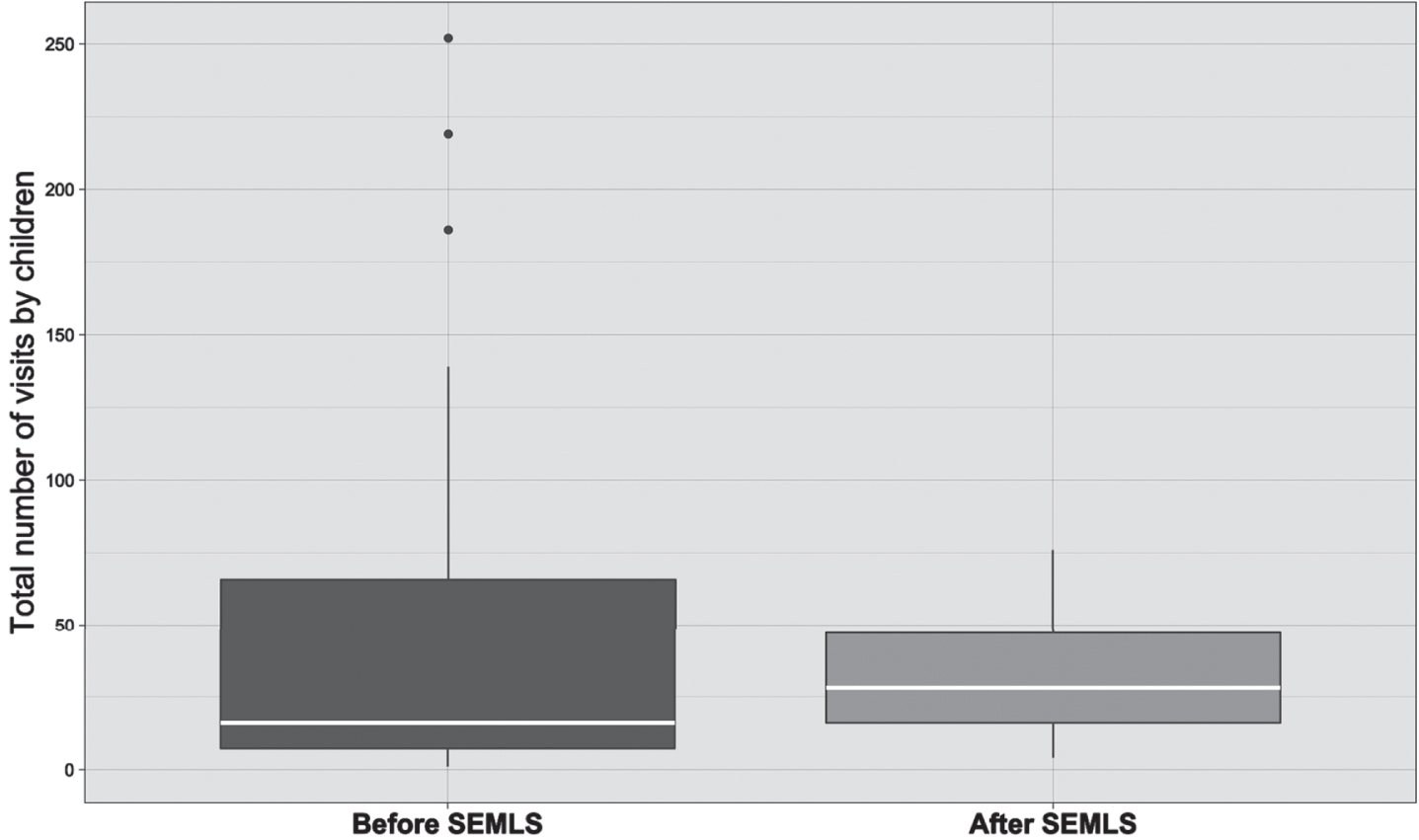
Total number of visits to all specialties before SEMLS and after SEMLS. The white line represents the median, and top to bottom box signifies the interquartile range. There were no statistically significant differences (p = 0.106) using a Wilcoxon signed-rank sum test for total number of visits to all specialties before and after SEMLS.
This study represents the first report of utilization of outpatient hospital-based services following SEMLS in children with CP. Results did not support the hypotheses that ambulatory children with CP would have greater utilization than non-ambulatory children in the year after surgery, children with high surgical burden would have greater utilization than children with low surgical burden in the year after surgery, or utilization would be greater in the year after surgery than the year prior to surgery. Only utilization for orthopaedics and radiology were found to be greater in the year after surgery. Utilization of therapy services (total number of visits) in the year after surgery was the opposite of what was hypothesized, as children had less therapy visits. These findings contribute to the limited literature on care utilization in children with CP after SEMLS.
It is difficult to compare these results to others because published literature related to SEMLS focuses on outcomes after surgery in ambulatory individuals with CP and does not describe hospital utilization [10]. Children in the current study were similar in age to what the literature recommends as the ideal age to undergo SEMLS [21]. Unlike studies that only include ambulatory children [10–12, 22–27], 47% of this sample were non-ambulatory. The number of non-ambulatory children in this sample is similar to Himpens [9], who reported 45% of their sample being non-ambulatory children. In this study, 40% were GMFCS Level IV and 7% GMFCS Level V, and similarly, in the Himpens [9] study, 35% were GMFCS Level IV and 10% were GMFCS Level V. Evidence suggests children who are non-ambulatory have differences in prognosis, function, and parent satisfaction following SEMLS [9, 21]. Similar to others [10], the results of this study support the importance of reporting on ambulatory children (GMFCS I–III) separately from non-ambulatory (GMFCS IV-V) children. This also aligns with a multi-stakeholder developed research agenda stressing the need to include non-ambulatory children with CP in studies in order to generate knowledge to improve their care.
Surgical burden has been included in recent studies as a potential variable to explain variation in outcomes in children with CP after SEMLS [11, 12] and in receipt of inpatient physical therapy after SEMLS [28]. Results from the current study indicate there was no difference in the number of specialties seen and the number of total outpatient visits to each specialty based on surgical burden, which likely reflect the small sample size. Previous studies on ambulatory children report those with low surgical burden have improvement in gait and physical activity after surgery [11, 12] versus those with high surgical burden. This study involved children who were non-ambulatory (GMFCS Level IV and V), whereas Lennon [11] and Niler [12] did not include non-ambulatory children. A study of inpatient physical therapy utilization found children with high surgical burden were more likely to receive inpatient physical therapy following lower extremity orthopaedic surgery but did not examine outpatient services [29]. Not surprisingly, a relationship was found between surgical burden and ambulatory status, with non-ambulatory children more likely to have high surgical burden. Studies with larger sample sizes are needed to understand how surgical burden may mediate the effect of ambulatory status on utilization and outcomes. Surgical burden should be considered when developing post-operative guidelines as individual needs likely vary in regard to pain management and initiation of weight bearing after surgery.
Contrary to the hypothesis, when comparing utilization in the year before surgery to the year after surgery, the current cohort demonstrated no differences in the number of specialties seen among children. However, there were more orthopaedic and radiology visits but fewer outpatient therapy visits in the year after SEMLS compared to the year before SEMLS. Due to limitations in the dataset available from the electronic health record (EHR), therapy visits could not be stratified based on provider discipline. This study followed similar methods of the investigators’ previous work combining physical, occupational, and speech therapies into one category [7]. Despite the widespread acknowledgement of the importance of post-operative rehabilitation [10, 30], there could be several explanations for the finding of less therapy visits in the year after SEMLS. Standard practice at this study’s institution involves immobilizing patients in casts with limited weight bearing during the 6–12 week healing process. Aligned with this timeframe, many children stopped most (or all) therapies during this time. Further, when weight bearing and activity restrictions were lifted, it is possible that the children may have focused on physical therapy for much of the year while reducing visits to other therapies. Based on the current study’s findings, continued monitoring of children through their second year after surgery may be helpful to examine service utilization over a longer period. Another reason could be that increased visits were recommended but did not occur due to caregiver preference, decreased access to therapy visits, or difficulty coordinating visits. The pattern of decreased therapy visits after surgery found in this study may not be observed across other institutions which emphasize early mobility after SEMLS [30]. An alternative explanation for the reduced therapy visits in the year after SEMLS may be that utilization in the year before may have been increased because some children may have received a burst of pre-habilitation physical therapy prior to SEMLS to either attempt to prevent surgery from occurring or improve strength prior to surgery. This approach has shown favorable effects in adult populations [31, 32].
All of the scenarios listed above may have resulted in a difference in outpatient therapy services before and after surgery in the current study. Nevertheless, therapy was the top specialty seen by children in both the year before and the first year after SEMLS regardless of ambulatory status. These findings are similar to the investigators’ previous work including all children with CP [7]. It is known that care coordination can be complex for children with CP when a greater number of unmet needs are present [33], and it is possible that this facility did not have adequate care coordination after surgery to schedule increased visits. A previous report indicates caregiver burden is elevated during the post-operative period [18]. Reasons for increased burden are not known, but the results suggest it is not due to increased visits. Like others [34, 35], these results possibly reflect gaps in care for reasons that are not well understood. Studies to understand parent preferences and needs after surgery are needed to develop post-operative protocols and improve care. Longitudinal studies following children over several years would be beneficial to examine trajectories of utilization across a child’s lifespan but would be costly to conduct. In agreement with McGinley et al. [10] further research is needed on the relationship between details of post-operative physical therapy, time of mobilization after surgery, and outcomes.
Limitations of this study include generalization of the dataset, external variables not collected, and a small sample size. Information from the data utilized from the EHR from one institution cannot be generalized to all facilities. The small sample limited this study’s ability to examine the variation in hospital utilization between individual GMFCS levels or within each group (ambulatory versus non-ambulatory). Therapies were not examined by each discipline, which might provide details to better understand therapy service utilization in children with CP before and after SEMLS. In addition, some children may have received care outside of the study’s facility, including other hospitals, private clinics, or school settings. Only data present in the facility’s EHR was able to be described. These data were collected on in-person visits retrospectively before the COVID-19 pandemic when the use of telehealth for visits was initiated. From experience, some visits are continuing via telehealth and also in-person, which could be looked at in the future. Results from this study support the need for larger studies that examine each therapy separately and consider parent perspectives and preferences on coordination of care and burden following SEMLS.
Conclusion
This study highlights service utilization for children with CP following SEMLS. Despite the limitations of this small study, results demonstrate children had more orthopaedic and radiology visits and less therapy visits in the year after SEMLS, and nearly half of children with CP who undergo SEMLS are non-ambulatory. Further examination of care needs in children with CP undergoing SEMLS are warranted and should consider differing needs for ambulatory versus non-ambulatory children, surgical burden, and post-operative immobilization. Studies across centers would be most useful due to the varying practices across institutions.
Footnotes
Acknowledgments
This study was partially supported by Cincinnati Children’s Patient Services Research Grant.
Conflict of interest
The authors have no conflicts of interest to report.
Ethical considerations
Institutional Review Board approval was obtained for this study with waiver of consent using EHR (IRB 2014-6879 and IRB 2020-0112).