
Abstract
PURPOSE:
To assess the performance of premature infant oral motor intervention for transition from gavage to full spoon feeding in preterm infants.
METHODS:
Preterm neonates born between 28 + 0–32 + 6 weeks gestation (n = 32) were randomised into an intervention group (premature infant oral motor intervention) for five minutes twice a day along with routine care (n = 16) and a control group (routine care, n = 16) once they reached a feed volume of at least 150 ml/kg/day administered by gavage method. The primary outcome measure was time (in days) to transition from gavage to full spoon feeds.
RESULTS:
The mean (SD) time to transition from gavage to full spoon feeds was attained significantly earlier in the intervention group than the control group (9.93 [5.83] vs 16.43 [10.46] days; mean difference, -6.5 days; 95% CI, -12.58 to -0.41). There was no significant difference between the two groups in terms of the duration of hospital stay, rates of physiological stability, and culture positive sepsis.
CONCLUSION:
Premature infant oral motor intervention, as used in this specific population, significantly reduces the time to transition to full spoon feeds without increasing culture positive sepsis and physiological instability.
Introduction
Globally, an estimated 15 million births per year are preterm (before 37 week’s gestation) with the majority (two-thirds) of them in Africa and South Asia [1, 2]. Although advancements in medical technologies in neonatal intensive care units (NICUs) in the last few decades have greatly increased survival rates of preterm neonates. Yet, many of them still need to remain admitted in NICU because of variety of medical and developmental complications [3].
Assisted feeding is one of the most common nursing care practices in the NICU. Feeding is a complex, developmentally regulated skill. The choice mode of feeding depends upon gestational age, sucking pattern, and the coordination between swallowing and breathing [4, 5]. Those born at < 32 weeks of gestation are fed by gavage due to immature sucking pattern and lack of coordination between swallowing and breathing. However, between 32-34 weeks gestational age, healthy preterm infants may begin to feed from a spoon or paladai as shown in Fig. 1 (due to a slightly more mature sucking pattern and establishment of coordination between swallowing and breathing). Independent oral feeding in a healthy preterm infant is typically achieved by 36 to 38 weeks of gestational age due to complete maturation of oral feeding reflexes [6, 7].

Paladai used for oral feeding.
Acquisition of mature sucking pattern along with the development of coordination between swallowing and breathing in neonates born very preterm (<32 weeks gestation) is a complex process. Hence, this subgroup of preterm neonates frequently have lengthy initial hospital stays until they achieve these skills and maintain enteral nutritional intake to support growth and development, consequently imposing additional costs on the families and the health care systems of the country [5].
Oromotor stimulations are designed to normalise oropharyngeal sensation by restoring reflexes required for oral feeding. In turn, they elicit normal oral movements of lips, tongue, jaw, and pharynx for development of sucking and swallowing [8, 9]. This facilitates the development of oral feeding skills and hence accelerates the transition from gavage feeding to spoon feeding [3].
Premature Infant Oral Motor Intervention (PIOMI) was developed by Lessen specifically for younger preterm infants, and adapted from the original Beckman’s Oral Motor Intervention (BOMI) as the BOMI is complex, takes a longer time to implement, and is not tolerated well in very preterm neonates [10]. Further, PIOMI is the only oral motor stimulation programme that has established intervention fidelity. It requires formal training to ensure it is easily taught to the healthcare providers as well as parents and can be reliably and consistently performed [3, 12].
Recent studies have shown that the PIOMI applied to preterm infants can facilitate their oral feeding progress with reduced transition time to independent oral feedings, better weight gain, and decreased length of hospital stay [10, 13–15].
A recent systematic review of clinical trials (eight trials included PIOMI as an intervention) to explore the efficacy of pre-feeding oromotor stimulation in preterm infants demonstrated that the use of oromotor stimulation is effective in improving feeding progression of preterm neonates. However, its effect on weight gain and duration of hospital stay was not uniform [16]. The authors of the review have suggested that further studies are needed to determine the ideal timing of initiation, duration, and frequency of the intervention as well as to explore its effect on preterm neonates with medical complications [16]. Therefore, the present study aimed to evaluate the effect of PIOMI along with routine care compared with routine care alone for transition from gavage to full spoon feeds in preterm neonates. Further, it was hypothesised that those preterm babies who are provided PIOMI along with routine care will have reduced time to transition from gavage to full spoon feeds compared with a similar group in whom routine care is provided alone.
Study design and participants
The present randomised controlled trial (RCT) was conducted from December 2018 to November 2020 in the outborn NICU of ABVIMS & Dr. RML Hospital, New Delhi. The outborn NICU is for babies who are not born at the hospital but are referred for admission for advanced neonatal care. The protocol was approved by the ethics committee, ABVIMS & Dr. RML Hospital, New Delhi. An informed written consent was obtained from the parents of the babies before enrolling in the study. A total of 32 premature infants born at a gestational age of 28 + 0–32 + 6 weeks were included. The inclusion criteria were as follows: born with a gestational age of 28 + 0–32 + 6 weeks, physiologically stable at the time of receiving the intervention, having reached full gavage feeding (at 150 ml/kg/day) and in transition from gavage to spoon feeds, receiving non-nutritive sucking and kangaroo mother care (KMC) as a part of routine care. During the stimulations, the baby was off ventilatory support (either invasive or non-invasive). However, the infants could receive respiratory support by Heated Humidified High Flow Nasal Cannula (HHHFNC) with flow up to 6 litres/minute or nasal prong. The exclusion criteria were as follows: intraventricular haemorrhage (IVH) grade 2 or beyond, necrotizing enterocolitis (NEC) stage 2 or beyond, periventricular leukomalacia (PVL), bronchopulmonary dysplasia (BPD), and having chromosomal anomalies or congenital malformations, history of perinatal asphyxia, and neonatal jaundice necessitating exchange transfusion.
a Study procedure
Randomisation was done using variable block size of 4 to 8 in a 1 : 1 ratio. It was also done by an investigator who had no further role in collecting baseline variables, applying intervention and measurement of outcome or analysis of data and used the https://www.randomizer.org site.
Random treatment assignments were placed in serially numbered, opaque, and sealed envelopes. After parental consent had been obtained, the researcher opened the envelope and recorded groups when infants met the inclusion criteria.
Blinding of the primary caregivers or the investigators to the intervention was not possible because of the nature of the intervention. However, the secondary outcomes, i.e., episodes of bradycardia or desaturation during feeding sessions, were noted from the nursing chart, which was filled in every second hour by nursing staff who were blinded to the study aims.
b Intervention
The neonates enrolled in the study were continuously monitored for vital signs and oxygen saturation in the NICU. Although behavioural states of the infants were not evaluated, behavioural cues (signs of stress), physiological cues (apnoea or bradypnea, bradycardia or tachycardia) and vital parameters were continually monitored. In this study, the PIOMI was implemented once the baby was hemodynamically stable and off ventilatory support (either invasive or non-invasive).
The intervention (PIOMI) was administered to the neonates at least 30 minutes before the next feeding schedule twice a day for five minutes by an early interventionist trained in PIOMI. It was initiated once the infants were tolerating full gavage feeds (150 mL/kg/day) and continued until the day of full spoon feeding. Before providing the stimulations, the therapist washed their hands with either soap and water or hand sanitizer and put on sterile gloves.
After administration of the intervention, the initiation and advancement of spoon feeds were decided based on the assessment of sucking bursts and physiological stability during spoon feeding, i.e., absence of desaturation, apnoea, or bradycardia (recorded from nursing chart). The sucking bursts were assessed by the primary investigator using gloved hand for two minutes, who was blinded to group assignment, every third day till the baby could be fed independently with spoon feeding [17, 18].
The enrolled neonates in both groups also received non-nutritive sucking (NNS) prior to gavage feeding when they were physiologically stable and reached full gavage feeding (at 150 ml/kg/day). In this technique the neonate was put to the breast after expression of milk and allowed to suck on it. Initially, the intervention was carried out for a brief period once a day and gradually increased to suck for at least five minutes about 4-6 times per day [19]. Kangaroo mother care (KMC) was provided as a part of standard care for preterm infants in both groups [20].
Outcomes
The primary outcome of the study was time to attainment of full spoon feeding, defined as the number of days taken to make the transition from complete gavage feeding to spoon feeding.
The secondary outcomes included episodes of bradycardia or desaturation during or immediately after spoon feeding, episodes of blood culture positive sepsis, duration of hospital stay calculated from the recorded date of admission to the date of discharge, and duration of hospital stay after enrolment calculated from the recorded date of enrolment to the date of discharge.
The trial was registered with CTRI (number: CTRI/2019/06/019853).
Statistical analysis
Sample size was calculated on the basis of a previously published study [13]. A sample size of 32 (16 in each group) was necessary to achieve 90% power to detect a difference of three days in transition from gavage to full spoon feeds between the PIOMI and the non-PIOMI group at a significance level of 0.05 and a standard deviation of 2.6. Allowing up to 20% attrition, a final sample size of 39 was calculated.
Demographic and clinical characteristics were summarized at baseline as counts and percentages for categorical variables and as means (±SD) for continuous variables. The Student’s t-test and chi-square test (or Fisher’s exact test as appropriate) were used for the analysis of continuous and categorical variables respectively.
SPSS version 21 was used for statistical analysis.
Results
A total of 62 preterm neonates were screened for eligibility, and 41 were eligible for randomisation. Nine infants were excluded post randomisation: four for severe BPD, three for IVH grade ≥ 2 and two NEC stage ≥ 2. Finally, 32 babies were analysed in the study (Fig. 2).
There was no significant difference in the baseline characteristics between the two groups as shown in Table 1.
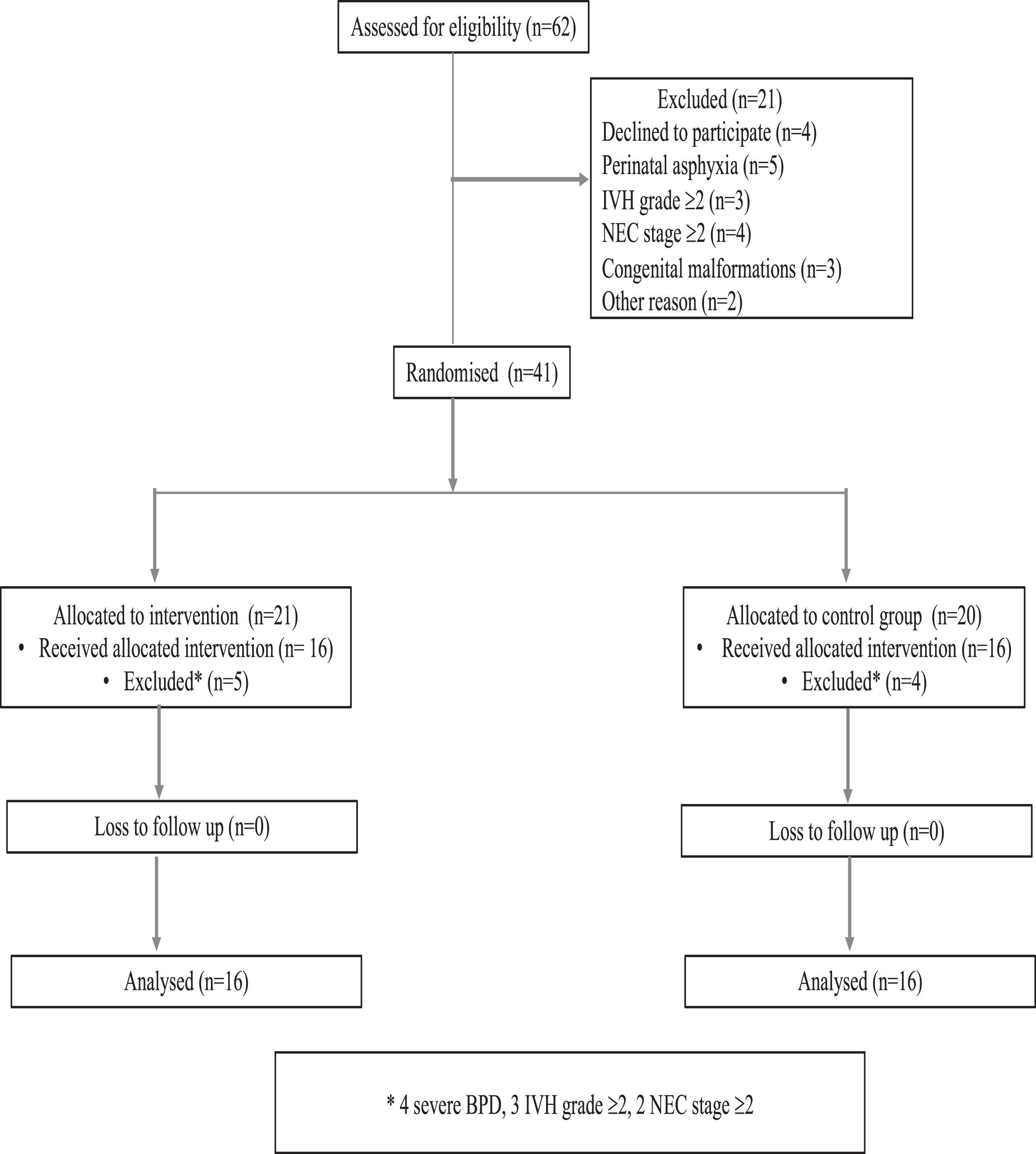
Participant flow chart.
Baseline characteristics of the study participants
RDS: respiratory distress syndrome, HHHFNC: Heated Humidified High Flow Nasal Cannula. Full gavage feeds were defined as a feed volume of at least 150 ml/kg/day administered by gavage method.
Table 2 shows the study outcome variables for the two groups. The mean (SD) time taken to make the transition from complete gavage feeding to spoon feeding in the intervention group was significantly earlier than in the control group (9.93 [5.83] days vs 16.43 [10.46] days; mean difference, -6.5 days; 95% CI, -12.58 to -0.41; p = 0.038).
Study outcome variables for the two groups
*p value significant by Student’s t test at 5% level of significance.
The PIOMI group had a mean (SD) hospital stay of three days less than the control group (21.75 [22.59] days vs 24.75 [17.57], mean difference, -3.00 days; 95% CI, -17.61 to 11.61; p = 0.849). There was no significant difference in the total duration of hospital stay, episodes of bradycardia, desaturation during or immediately after spoon feeding, and episodes of culture positive sepsis.
This randomised controlled trial showed when additional PIOMI is combined with routine practices of KMC and NNS, it further improves feeding abilities in preterm neonates. The transition from gavage to full spoon feeds was achieved significantly earlier without increasing episodes of culture proven sepsis and physiological instability. The result is consistent with previous studies which found that pre-feeding oromotor stimulation significantly improves feeding skills in an interventional group compared with controls [3, 21–23]. However, the study by Bache et al. reported that oral stimulation does not significantly shorten the transition period to full oral feeding [23]. This discrepancy may be due to the different population characteristics, timing of initiation of the intervention, or type and number of oral stimulations per day, all of which contribute to proper development of oral feeding skills [23].
In the present study, the mean age at enrolment of participants in the PIOMI group was three days later as compared to the non-PIOMI group. However, the difference was not statistically significant. The babies enrolled in the PIOMI group were smaller (birthweight 1269.25±276.60 g vs1348±300.67 g) and sicker, evidenced by increased incidence of requiring resuscitation at birth, incidence of RDS and mechanical ventilation. For additional information, see Table 1. The gestational age at enrolment was similar across both the groups.
Moderate and very preterm infants experience oral feeding difficulties due to delay in the development of oromotor skills and poor suck-swallow-breath coordination [24]. Development of these skills is necessary for oral feeding and prevention of apnoea, bradycardia, and desaturation. Moreover, feeding dysfunction requires the infant to expend a lot of energy and may lead to delayed development as well [25].
Appropriate sucking and swallowing in preterm infants is a sign of better development. PIOMI achieves these goals through normalization of movements of lips, tongue, jaw, and pharynx for development of sucking and swallowing as well as its coordination with breathing [10].
The present study found a shorter duration of hospital stay in the PIOMI group as compared to the non-PIOMI group after initiation of the intervention. Although this finding did not achieve statistical significance (p = 0.849), possibly due to smaller sample size, it has definite clinical relevance. The finding is consistent with previous studies which found that pre-feeding oromotor stimulation significantly improves the development of oral-motor skills. They led to an earlier achievement of independent oral feeding and hence reduces the duration of hospital stay. Similar findings were also noted in the studies which had included infants below 30 weeks of gestational age as well [3, 10] This finding has definite relevance as PIOMI, takes only five minutes to perform, doesn’t utilize any special instrument and, by reducing the duration of hospitalization, can therefore significantly reduce the cost imposed on families and the health care system.
In a recent clinical trial comparing parent versus professional administered PIOMI, it was found that parent administered PIOMI was as effective in reducing the transition time to independent oral feeding and length of stay [26]. No adverse events were noted in either group. Parental satisfaction was high. In addition, there also was enhanced perception of adequacy to care for their infant. Hence, parent administered PIOMI can additionally reduce the burden of workload on healthcare providers, particularly in developing countries [26].
The present study found lower weight at discharge in the PIOMI as compared to the non-PIOMI group without achieving statistical significance. Ghomi et al. also noted a similar finding. When they analysed the change in weight over time and for interaction of time and group within-subjects, it was found to be significant [3]. Given the weight at enrolment was lower and duration of hospital stay after enrolment was three days shorter in the intervention group in the present study, it can be concluded that the intervention group reached the same weight as the control group in lesser time and at a younger age. However, since the data of daily weight gain of the individual subjects was not collected; hence, this finding could not be better substantiated.
The present study has some limitations as well. First, the participants could not be blinded because of the nature of the intervention. However, this might have had an indirect effect on the assessment of study outcomes. This is because PIOMI has the potential to change the behavioural state of the infant to an active alert state due to handling/manipulation. This change could be easily identified by the caregivers as a readiness for feeding. Second, behavioural state of the neonate pre- and post-intervention was not documented although negative physiological cues (such as apnoea or hypopnea, bradycardia or tachycardia) and behavioural cues (signs of stress) were continually monitored. Third, the primary outcome measure, i.e., transition from gavage to spoon feeding, was considered to be complete if the infant accepted the entire feed volume through spoon without having physiological instability on a particular day. However, this finding was not assessed for 2-3 consecutive days. Fourth, since the gestational age of the enrolled babies spanned different subcategories of preterm birth, a time-to-event analysis would have been ideal to assess the impact of the intervention across various birth strata. Finally, stratification of the effect of the intervention based on gestational age or birthweight couldn’t be done due to small sample size.
Conclusion
PIOMI in preterm neonates born between 28 + 0–32 + 6 weeks gestation improves feeding ability, promotes earlier attainment of spoon feeding and earlier discharge from the hospital after initiation of the intervention without causing physiological instability or increasing episodes of culture positive sepsis. If standardised and practised routinely in NICUs, the intervention has the potential to reduce the cost of preterm care in developing countries.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors have no conflicts of interest to report.
Ethical considerations
IRB no.: 286 (04/2019/IEC/PGIMER/RMLH)/175/19; date: 01/02/2019. Informed written consent was obtained from the parents of the babies before enrolling into the study.
Funding
None to report.