
Abstract
PURPOSE:
Collaboration between physical therapists and caregivers of children who receive physical therapy is integral to providing family-centered care. Successful collaboration depends upon the therapeutic relationship built within the caregiver-therapist dyad. However, the nature of these relationships is not well understood. The purpose of this study was to explore the caregiver-pediatric physical therapist relationship from the perspectives of the caregiver and pediatric physical therapist.
METHODS:
A qualitative multiple case study methodology was used; a caregiver and pediatric physical therapist represented a bounded case. Each caregiver and therapist engaged in separate, semi-structured, in-depth interviews.
RESULTS:
Through within- and cross-case coding, three themes were identified: physical therapist as a guide, the caregiver-pediatric physical therapist connection, and professional qualities and performance.
CONCLUSION:
These themes help to provide an understanding of the therapeutic relationships that can occur between caregivers and pediatric physical therapists, which can help support effective collaboration as part of providing family-centered care.
Introduction
Pediatric physical therapists (PPTs) work with children and families to improve independence, participation, and function in a variety of settings [1]. When a child begins physical therapy, a relationship is established between the child and the PPT, but also between the child’s primary caregiver(s) and the PPT; the child cannot access therapy or make decisions about care on their own. In some practice settings, the PPT and caregiver may interact frequently, whereas in others, the opportunities for interaction may be limited. The caregiver-PPT relationship also differs based on the characteristics of each family and PPT. A family-centered approach highlighting good communication and consideration of the family’s needs is considered best practice in pediatric physical therapy [2]. A child’s primary context is within their family; therefore, to consider what is best for the child, the PPT should assist in helping to determine what is important to the family [3]. Each family is unique, which must be taken into consideration for all aspects of pediatric physical therapy [4].
Collaboration is a key component to family-centered care [5] and has been shown to increase parents’ confidence in caring for their child with special needs [5], decrease stress, improve functional outcomes, and improve satisfaction with healthcare services [5, 6]. Collaboration has been identified as important to therapists and their attitude toward it positive, but implementing it into practice can be challenging [5, 8]. This challenge is in part due to limited research on specific processes to promote collaboration [5, 9], differing strategies among various practice settings [10], and an inadequate delineation of roles, including recognizing the parent as the expert on their child [11]. Ineffective communication can also be a root cause of limited collaboration [5, 12].
An understanding of the caregiver-PPT relationship from the perspective of both caregivers and PPTs could be useful in mitigating obstacles to collaboration and in promoting family-centered care. Current literature providing insight into how caregivers and PPTs perceive their relationship is limited. One recent qualitative study highlighted the importance of the therapeutic alliance within the parent-child-PPT triad [13], but this concept could benefit from further research. Studies that explore the caregiver-therapist relationship have been conducted, but it is often a minor aspect of a study with a different focus, such as the burden of care experienced by caregivers of medically complex children [14], caregivers’ views on their child’s activity and participation levels [15], or therapists’ perspectives on care coordination [16]. There have been studies that explore characteristics such as trust, confidence, and respect, but the use of a survey format limits the ability to gain deeper knowledge from the caregiver’s or PPT’s perspective [7, 17]. Other studies that have explored the caregiver-PPT relationship lack detail and/or are outdated [18, 19].
The purpose of this qualitative case study was to explore caregiver-PPT relationships from both the caregivers’ and PPTs’ points of view to provide deeper insight into the caregiver-PPT relationship.
Materials and methods
A qualitative multiple case study methodology was used to explore the lived experience of caregivers and PPTs who, as a dyad, represented a bounded case. Using bounded cases required that the two individuals participating were connected through their shared experience, meaning the case could not be appropriately studied without both parties. A multiple case study approach allowed for in-depth exploration of real, in-progress partnerships [20, 21]. Each case essentially served as a study within itself, providing information unique to each case, while also providing information in the aggregate across all cases [21]. A postpositivism paradigm was used as the basis of this study to allow for multiple perspectives and rigorous research methods [22] to help identify patterns in the human experience. This study does not aim to capture a universal truth, but rather the truths of the participants in this study [23].
Data collection took place from January 2018 to August 2018. The study was approved by the Institutional Review Board at the University of Indianapolis and Midwestern University. The primary researcher was a pediatric physical therapist with a Doctor of Physical Therapy degree and in the process of obtaining a Doctor of Health Science degree. The primary researcher had prior experience with qualitative research.
Participants
All participants were either a caregiver or a PPT. Participants self-identified their role as primary caregiver, which was confirmed in the interview. A PPT could participate if they were a licensed, practicing physical therapist who had been engaged in a therapeutic relationship with the caregiver participant and their child for at least six months. Individuals could not participate if they did not speak English or had any cognitive deficits that resulted in an inability to provide consent or answer a series of questions in an interview format. A total of five cases equaling 10 participants was involved in this study. This number allowed themes to be developed within and across cases. Participants had no prior relationship with the primary researcher and were informed that the primary researcher was a pediatric physical therapist with 15 years of experience in settings such as outpatient, school, and home health.
Procedures
Criterion and convenience sampling were used, which allowed the researcher to determine if the potential participants fit the criteria and needs of the study [22]. A recruitment email was sent to PPTs practicing in the same city as the primary researcher to request assistance in identifying potential participants. When this yielded limited results, recruitment was expanded by sending an email to the listserv of the Academy of Pediatric Physical Therapy. Additionally, caregivers were recruited through an internet message board for parents of children with special needs. These avenues of recruitment were intended to reach PPTs from diverse settings and states with varying levels of experience. Initially, eight people responded with interest; of those, five chose to move forward with the study and three did not follow up after being contacted by the primary researcher. Two caregivers who wanted to participate contacted their child’s PPT to discuss the study and request participation. Three PPTs interested in being a part of the study each chose a caregiver of a current patient and inquired about participation; this yielded a total of 10 participants in five dyads. Once both partners of a case were established, no one dropped out of the study.
Informed consent was obtained from all participants prior to data collection. The primary researcher conducted all interviews; four interviews were conducted face-to-face, and six were on the phone. All interviews were audio recorded. Face-to-face interviews took place in participant homes and public areas such as coffee shops; efforts were made to minimize distractions. Each interview ended when no new information was revealed [24, 25]. Interviews were conducted using a semi-structured interview guide (Appendix 1) comprised of open-ended questions designed to facilitate discussion [22]. The guide was constructed by the primary researcher and refined based on input from three additional researchers, all faculty members with decades of combined experience in designing, implementing, and disseminating qualitative research. Participants were also asked general background and demographic information (Appendix 2).
Data analysis
Interviews were transcribed verbatim by hand to allow the primary researcher to be more fully immersed in the data [25]. Data analysis software, Dedoose [26] (version 8.1.8), was used to store audio recordings and de-identified transcripts in a secure, password-protected manner. Participants received a copy of their transcript to review for accuracy. One participant requested a portion of their transcript not be used, which was honored. All other participants approved their transcript as it was. This process of member checking enhanced the study’s credibility [27].
The primary researcher initially reviewed transcripts and used memoing to record initial interpretations and perceptions about the data, followed by a process of open coding [28]. Next, a secondary researcher reviewed and coded one-page excerpts from two cases independent from the primary researcher to enhance the trustworthiness of the results. Though the secondary researcher’s codes were not identical to the primary researcher’s, both agreed the codes were very similar and captured the essence of the transcript excerpts. Axial coding was then conducted to categorize the codes and establish relationships among codes. A codebook, which contained a list of the codes, descriptions, and sample data for reference [28] was maintained within Dedoose [26].
After open and axial coding were completed, the codes were combined into categories representing themes that emerged [28]. A third researcher reviewed the codebook and assisted the primary researcher with finalizing the themes by refining the wording. This process of triangulation helped verify the credibility of the results [28]. The process of coding and developing themes was done both within each case and among all the cases to better capture the experiences of each bounded case as well as the cases in aggregate. Potential biases were limited through the use of field notes before, during, and after interviews [28]. Additionally, the researcher maintained an audit trail in Dedoose [26]. and in hardcopy form. The audit trail provided details regarding the decision-making process so that any future researcher could follow it and be able to produce similar results. This transparency enhances the study’s trustworthiness [27].
Results
The mean length of caregiver-PPT relationships explored in this study was 3.3 years (range of 2–9 years); PPTs’ years of experience ranged from 15 to 30 years (mean 24.8 years). The age of children receiving physical therapy was between two and 9 years (mean 4.7 years). Two children received physical therapy only in the home, two only in an outpatient physical therapy clinic, and one child received physical therapy both at home and in an outpatient clinic. Participants were from various locations throughout the United States. Interviews ranged from 21 to 30 minutes (mean 26 minutes).
Three major themes emerged: 1) PPT as a guide, 2) the caregiver-PPT connection, and 3) professional qualities and performance. Themes were consistent among all dyads and helped create a picture of the caregiver-PPT relationships in this series of case studies. Each of these themes included sub-themes, which along with selected participant quotes, can be found in Table 1. Pseudonyms or codes were used in place of participant names to protect privacy. A graphic representation of themes can be seen in Fig. 1.
Themes
Themes
PPT = Pediatric Physical Therapist; PT = Physical Therapist.
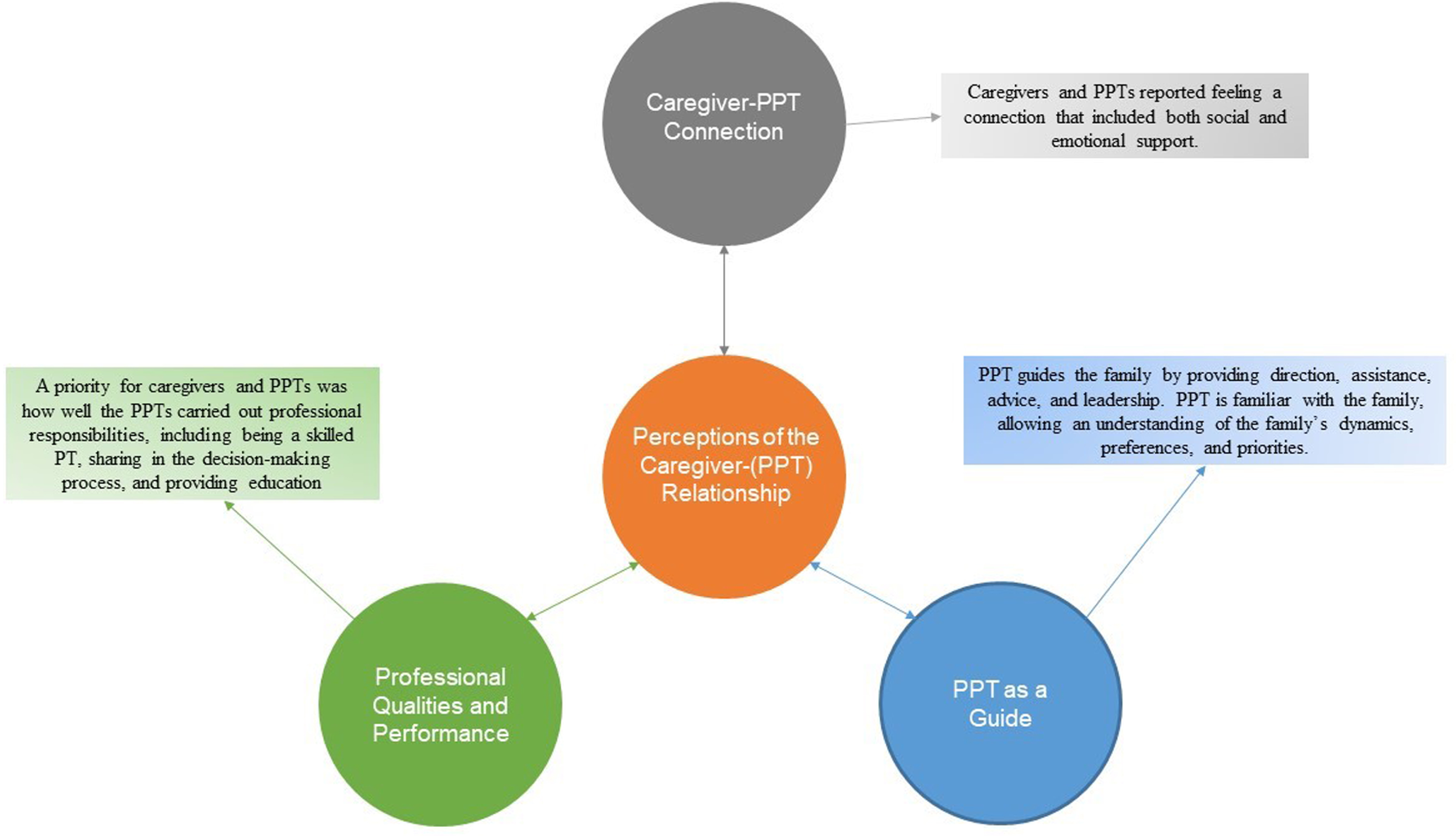
Perceptions of the Caregiver-Pediatric Physical Therapist Relationship: Themes. PPT: Pediatric Physical Therapist.
The role of the PPT as a guide surfaced as a theme within and across all cases. For participants, a guide was someone who showed the way to a path or purpose by providing direction, assistance, advice, and leadership. Caregivers reported seeking guidance from their child’s PPT about numerous issues. Some were directly related to physical therapy, such as decisions about assistive or orthotic devices. Others were related to health insurance, medical decisions, other therapy disciplines, and social situations for the child.
Familiarity
A subtheme of familiarity emerged within the theme of PPT as a guide. In this study, PPTs worked with families for a range of 1–9 years, which allowed the PPT to have a high level of familiarity with the child and family. This familiarity was not just diagnosis- or disability-related but also encompassed an understanding of the family’s dynamics, preferences, and priorities. This intimate knowledge put PPTs in a unique position to guide a family through many processes and decisions. Regarding the PPT’s familiarity, one caregiver reported:
And my husband says to me all the time ‘you’re the only other person in the world who understands how I feel about it and how much we love this child of ours and how much, how special he is . . . and I have to tell you that I think our physical therapist is a close second in there, about understanding all of that . . . she knows what a great kid he is, she knows what he came from . . . and sees how far he’s come.
PPT guidance in this study encompassed many domains and, while each family had unique concerns and challenges, similarities could be seen across the cases.
Theme 2: The caregiver-PPT connection
Caregiver and PPT participants consistently reported the presence of a connection or bond between the caregiver and PPT, which became the second theme that emerged from this study. As reflected in the subthemes listed below, this connection had elements of a social nature as well as an emotional one.
Social
At times, a personal relationship formed between caregivers and PPTs. PPTs and caregivers often connected over their shared interest in the child receiving therapy. A connection was sometimes the result of mutual interests such as hobbies, personal values, and acquaintances, which helped forge a bond. One mom of a two-and-a-half-year-old child who had been working with the PPT for two years indicated, “I like to have a personal relationship with them. You know, I share...a lot of our stuff with them, you know . . . Charlie, being my child, is the biggest part of my life, so they know an intimate part of my life.”
Additionally, participants reported that a social connection formed during time spent together over the course of the child’s physical therapy. Caregivers and PPTs often engaged in social talk (conversation not directly related to physical therapy) in the natural course of the PPT-child-family relationship. Social talk also occurred because it was indirectly related to physical therapy. For example, caregivers shared that they talked to their PPT about family vacations because they wanted advice on how best to navigate a vacation with their child who had different mobility or sensory needs. In turn, PPTs reported that they discussed personal social activities as a byproduct of keeping the family informed, such as needing to cancel due to an illness or family event. Participating in these types of conversations seemed to help the PPTs gain a better understanding of the family and the child’s role in it. One of the PPT participants said, “I think it’s part of getting a whole picture of the family...I think it’s important to engage, like, so that I can better support the family . . . ”
Caregivers and PPTs sometimes referred to their relationship as a friendship, while also indicating this was secondary in priority to the child’s therapy. A friendship may have formed but was not necessary for a meaningful, successful therapeutic relationship. Participants also discussed that it was important to maintain professional boundaries. One example that was cited several times by caregivers and PPTs was a preference not to be connected on social media while actively engaged in a therapeutic relationship. According to one caregiver, “All that matters is that they’re a good therapist. A lot of our therapists we’ve had for years and you do develop a friendship, but we don’t initiate that from the beginning. I would much rather someone be our daughter’s therapist than be our friend if there is an either or...”
Emotional
The idea of an emotional connection between the caregiver and PPT surfaced as an additional subtheme of connection. The caregiver-PPT relationship often involved elements of emotional support during stages of the diagnostic process, difficult treatment decisions, and celebrating the child’s successes. In addition, both caregiver and PPT participants reported that the PPT offered a supportive space for the caregiver to express ideas and emotions, while also providing validation. One PPT with 30 years’ experience stated, “ . . . when she [mom] has questions and ideas, I feel like I’m telling her ‘oh yeah, those are great ideas . . . you’re right on.’ . . . I reiterate that she’s doing all the right things for her daughter.”
For caregivers and PPTs in this study, emotional and social support seemed to move the relationship forward in a positive way and set the stage for other aspects of the therapeutic process such as treatment planning and shared decision-making. “It would be harder for me to take advice from them if my personality didn’t match as well,” said the mother of a three-year-old who had been seeing the PPT for one year.
Theme 3: Professional qualities and performance
Within each case as well as across all cases, a high priority for both the caregiver and the PPT was how well the PPT carried out their various professional responsibilities. Within this theme, several subthemes emerged: skill as a physical therapist, shared decision-making, education, and progress in therapy.
Skill as a physical therapist
For caregivers, having a skilled, knowledgeable therapist who engaged well with their child was of utmost importance. While the lack of a personal relationship was not mentioned as a reason for selecting or keeping a PPT, a lack of skill or knowledge as a PPT was important enough to caregivers that it would cause them to pursue a new therapist. PPTs also discussed how it was important to them that they provide patients and families with care that is based on a combination of current available evidence, their clinical experience, and patient/family experiences and preferences.
Shared decision-making
The caregiver-PPT relationship was often described in terms such as “partnership,” “teamwork,” and “collaboration.” When decisions needed to be made, caregivers and PPTs engaged in dialogue during which the caregiver could ask questions and the PPT offered advice. After an exchange of information and ideas, the child’s family (and the child, if old enough) ultimately made the decisions. One caregiver stated, “I think she’s done a good job of empowering me to make sure-to remind me that I can say no, but she always will give me her opinion and will always remind me that I can-I can disagree with whatever she’s saying, you know . . . ”
Education
Another important area of the PPT’s professionalism that participants discussed was the provision of education. Caregivers valued when their PPT educated them about their child’s condition or provided information based on past experiences and research. As one mother who had known her child’s physical therapist for three years reported, “We didn’t understand body awareness and how that’s not just a sensory processing disorder but you know how that goes in to her low muscle tone, so her educating us has been really crucial for us understanding this side of our daughter that we didn’t before.” PPTs in this study also reported that providing education and resources to families was an important aspect of the care they provided.
There was a considerable amount of consistency within each case. The caregiver and therapist often shared the same story, though interviews were done separately. They each described their relationship in similar terms. While each participant’s experience was never exactly like another’s, the themes arrived at through the coding process are a good representation of both caregivers’ and PPTs’ experiences.
Discussion
Current literature does not offer a full picture of how caregivers and PPTs perceive their relationship with one another. This study sought to reveal the perceptions of the caregiver-PPT relationship from both caregivers’ and PPTs’ points of view. This exploration of five caregiver-PPT dyads provided that insight and revealed themes of guidance, connection, and professional PPT qualities.
A past study found that PPTs highly ranked their role as a resource to the families they serve [29], but no specifics were provided. The ability to be a resource to families is enhanced by the PPT’s familiarity with the child and family, characteristics that were identified as critical to the provider-caregiver relationship in a study on the perspectives of parents with chronically ill children [30]. The findings of this current study are in line with these previous studies and expand upon them by providing greater detail as to how PPTs are a resource to families and how knowing the family well can assist in that.
The finding that an emotional and social connection between a caregiver and their child’s PPT is important aligns with other studies that indicated such support can improve care [16], lead to deeper relationships [18], and help validate the caregiver’s abilities [12]. Studies have also found that a child’s therapist may be viewed as an advocate, a mentor, or part of the family [18, 19]. However, characteristics of the relationship associated with these feelings have not been fully explored until now. The caregiver-PPT relationships in this study had many qualities in common with a friendship such as trust, honest communication, and shared interests, which all support family-centered care.
In a qualitative study of physical therapists and adult patients conducted by Miciak et al. [31], both parties indicated that relating to each other on a personal level helped put them at ease and enhanced the therapeutic relationship. There is a spectrum of how physical therapists choose to interact on a personal level with their patients, and it is up to each individual to decide where on that spectrum they prefer to be [31]. Though the Miciak study was done with adult patients, the findings are similar to this study in that an investment (social/emotional connection) is important to the therapeutic process. At the same time, PPTs recognized the need to be mindful of the obligation to maintain appropriate boundaries so there are no conflicts of interest that may impair professional judgment [32].
Caregiver and PPT participants in this study indicated that open communication and exchanges of ideas are important to the relationship, especially with regard to making decisions. Past studies have indicated that communication and trust are important to families of children receiving physical therapy [13, 34], and this study furthers the idea that this is important to families and PPTs.
Though not prevalent enough to be considered a theme, some caregivers did suggest that their relationship with their PPT could have an effect on the child’s progress toward goals. In a study about parent perceptions of home exercise programs (HEPs), caregivers reported that when the PPT communicated well, spent time engaged with them, and answered questions, the caregivers felt more confident in carrying out the HEP [33]. However, a direct connection between the caregiver-PPT relationship and outcomes has not yet been explored and could be a potential direction of future research.
Family-centered care is considered best practice for pediatric physical therapy [3] and is among the recommended core competencies in PPT education [35]. Past studies indicate that, though therapists understand and value family-centered care, implementing it into practice can be difficult [10]. Caregivers and PPTs in this study both described the presence of many family-centered characteristics that were woven in to the course of physical therapy. This included being mindful of the child’s role in the family, understanding family values when developing goals, and making decisions as partners. Participants recognized a need to feel a sense of relatedness to their therapeutic partner while also maintaining autonomy as a professional or caregiver, which are critical elements to behavior motivation and relationship building [36]. The themes identified reveal how the PPTs in this study engaged in family-centered care and that caregivers recognized and valued these attributes in the caregiver-PPT relationship.
Limitations
This study is not without limitations. There was a risk of bias as the primary researcher is a PPT, thus is personally close to this topic. Strategies to reduce this bias included field journaling, an audit trail, and triangulation.
In addition, due to the case study methodology, only caregiver-PPT dyads who had close relationships were likely represented, since they both needed to feel comfortable participating in the study. As a result, the study’s findings may give the impression that caregiver-PPT relationships are always helpful, supportive, and effective. However, it is important to note that the experiences of the caregivers and PPTs in this study do not reflect all caregiver-PPT experiences.
Though efforts were made to increase trustworthiness of the study by having an additional researcher code transcripts, this process could have been more robust by having the secondary researcher review several full transcripts versus excerpts from two transcripts.
Additionally, there is a limitation to this study in that less-experienced PPTs were not represented. The therapist participants in this study were all experienced (15 years or more), so their insights could also be from years of collective experience, not just the singular experience of their relationship with the participating caregiver.
Lastly, this study could have benefited from a greater number of dyads. An appropriate sample size for case study methodology in qualitative research is not a specified number but is rather left up to the researcher’s discretion [23]. Difficulty with recruitment was one reason the sample size for this study was 10 participants (5 dyads). A greater sample size would have added depth and variety to the data in terms of participant thoughts, experiences, and perceptions.
Implications for practice and future research
This study highlights salient aspects of the caregiver-PPT relationship and may provide insight into how these relationships function. While representative only of the bounded cases explored, the insight provided can be useful for caregivers and PPTs as they develop their working relationship. The need for guidance, an emotional and social connection, and the importance of the PPT’s professional performance are all aspects of the caregiver-PPT relationship that can be explored. While not setting these conditions as a pattern by which all relationships should conform, these insights could be a helpful way to start the conversation between a caregiver and PPT to determine which characteristics of their relationship are most meaningful to them and in what areas they may want to see improvement.
This study’s findings have implications for physical therapy education in addition to clinical practice. Family-centered care is an important component of educating pediatric physical therapy students. This study’s findings could help educators provide students with more specific information on the nature of PPT-caregiver relationships. By doing so, the students can implement techniques when practicing pediatric physical therapy in the future; providing guidance, enhancing social and emotional support, and providing skilled care are shown to be important to families, thus enhancing the provision of family-centered care.
There are ways to expand on this study’s findings through both additional qualitative exploration and quantitative research. For example, future qualitative studies could include other types of caregivers, including those with negative or neutral experiences, or explore specific aspects of family-centered care. In particular, research into negative experiences can help identify ways in which the caregiver-PPT relationship is not always successful. Negative experiences are not always the direct opposite of positive ones, so identifying factors that create unsuccessful caregiver-PPT relationships can also be useful in creating successful ones.
Additionally, a longitudinal study of the caregiver-PPT relationship could explore how these relationships change over time. The various themes identified in this study could also be explored through survey research, which could provide additional data and represent a larger sample of participants. Caregivers in the current study discussed how the relationship with their child’s PPT may affect the child’s performance and goal achievement; future studies could explore this more fully.
Conclusion
A PPT and caregiver of a child who receives physical therapy must form a relationship and work together to support the provision of family-centered care [5]. The specific characteristics of this relationship are unique to each family, and relationship needs may change over time [4]. As supported by the participants in this study, key elements of the relationship are that the PPT provides guidance, forms a connection with the caregiver, and demonstrates skills and expertise. These insights into the caregiver-PPT relationship may help reach the goal of providing family-centered care.
Conflict of interest
The authors have no conflicts of interest to report.
Funding
This study was funded, in part, by a grant from University of Indianapolis Doctor of Health Science Program.
Supplementary material
The appendix is available in the electronic version of this article: https://dx.doi.org/10.3233/PRM-210081.