
Abstract
PURPOSE:
This study assessed concussion knowledge in concussed youth and parents treated at a multi-disciplinary concussion center.
METHODS:
Youth (n = 50) and parents (n = 36) were approached at the beginning of a clinical visit. Participants completed a 22-item, previously published concussion knowledge survey before the visit.
RESULTS:
Responses were compared with previously collected, published data from adolescents in a high school setting (n = 500). The patient group was divided into those with one (n = 23) vs. two or more concussions (n = 27). Chi-square analyses compared total correct responses between youth, parents, and the high school sample. T-tests assessed differences in knowledge based on prior concussions, age, and gender. All groups showed high accuracy for return-to-play guidelines (>90%) and similar knowledge of concussion-related symptoms (72.3% vs. 68.6%). Significant knowledge gaps about diagnosis, neurological consequences, and long-term risks were present across groups (19% to 68% accuracy). The patient group more often misattributed neck symptoms to concussion (X2 < 0.005). Prior concussion and gender were not significant predictors of concussion knowledge (p > 0.5).
CONCLUSION:
Community and clinically-based educational techniques may not be effectively communicating knowledge about concussion diagnosis, symptoms, long-term risks, and neurological implications of concussion. Educational tools need to be tailored to specific settings and populations.
Introduction
Sports-related concussions affect over 300,000 people annually, with most occurring in athletes between the ages of 15–24 years old [1–3]. In reality, the number of concussive injuries for adolescents and children may be much higher when injuries occurring in unstructured recreational activities are considered [4]. More than 500,000 adolescents and children under 19 years of age are estimated to present to the emergency department (ED) for evaluation of head injury, and > 90% of these patients diagnosed with a concussion are discharged to home [5]. An increase in concussion-related research and public education efforts over the last 10 years has led to greater public awareness about concussions and greater attention to the consequences of mild traumatic brain injury/concussion [6–10]. Despite these efforts, as many as 50–70% of concussions may go unreported, undetected, or mismanaged due to the lack of understanding about concussion symptoms and proper management [11–15]. In addition to physical and neurological observations, diagnosis of concussion relies heavily on subjective, patient-reported symptoms, as do decisions about recovery and return to play. As such, providing patients and families with clear and accurate information about the mechanisms, diagnosis, and recovery from concussion is essential.
Between 2001 and 2016, there have been five consensus statements released by the concussion in sport group regarding best practices in concussion diagnosis and treatment, reflecting the significant increase in the published literature and shifts in recommendations for appropriate treatment. The Centers for Disease Control and Prevention (CDC) created the HEADS UP Concussion in Youth Sports (HEADS UP) initiative to offer a more standardized approach for disseminating concussion information to health care providers, coaches, parents, and athletes involved in youth sports [16, 17]. HEADS UP materials are free and include presentations, handouts, an app, podcasts, videos, social media, and a website; all are intended to promote education about diagnosis, treatment, and prevention of head injuries. HEADS UP highlights concussion danger signs such as “one pupil larger than the other,” “drowsiness or inability to wake up,” or “a headache that gets worse and does not go away.” HEADS UP also presents concussion symptoms that are observed, such as “can’t recall events prior to or after a hit or fall,” “appears dazed or stunned,” or “moves clumsily,” along with symptoms reported by the individual, such as “balance problems or dizziness,” “bothered by light or noise,” or “feeling sluggish, hazy, foggy, or groggy.”
Most youth sport programs require athletes and parents to complete some portion of the HEADS UP educational curriculum. However, despite increasing awareness about concussions, inaccuracies and misperceptions about concussions remain in the public domain [6–8, 19]. Studies have demonstrated that players, parents, coaches, and trainers have misconceptions or lack knowledge about the symptoms of concussion and management after injury [9, 20–22]. In a 2017 study of coaches, parents, and players, Nanos et al. found that only 34.3% of all respondents were able to define a concussion as a brain injury [22]. Knowledge rates about concussion symptoms and treatment guidelines among high school athletes varied substantially (between 50% to 70%), with youth better able to recognize certain types of symptoms, such as cognitive symptoms, over others such as mental health symptoms [1, 23]. Mrazik and colleagues reported in 2015 that personal history of exposure to head injury and contact sport resulted in higher concussion knowledge among youth, but this has not been consistently replicated in other studies [24, 25].
Parent characteristics are also linked with varying levels of concussion knowledge and differing attitudes toward concussion risks in youth sports. Lower levels of parent education and household income have been correlated with lower levels of concussion knowledge and a less concerned attitude regarding concussion risk in youth sports [18]. Parents who exhibited greater parental sport pressure were also found to have lower odds of encouraging their child to report symptoms, while parents with children who had a history of concussion were more likely to encourage symptom report [26]. Sensationalized media coverage of concussion without discussion of expectations for recovery may also contribute to confusion among parents and youth about the long-term sequelae following concussion [27].
It is unclear whether the current educational approach in acute care and primary care settings for patients with concussion translates to increased knowledge about concussion symptoms and management among patients and parents. The aim of this study was to examine the general understanding of concussions among youth athletes and their parents who had recently received concussion education or information as part of treatment for a concussion. The entire study cohort, who had been diagnosed and treated for a concussion before being evaluated in a multidisciplinary concussion clinic, had already received concussion education from a referring medical or health care provider. Concussion knowledge was assessed among these youth patients and their parents, comparing their concussion knowledge to each other and then to a previously published cohort of high school athletes, in which the majority (76.6%) had not reported a history of concussion. The high school athlete sample data was culled from a previously published paper, and no parent data was available within this sample. It was expected that the current cohort, all of whom had been diagnosed with a concussion and had received concussion education/information, would have greater knowledge about concussions compared to the previously published sample composed of high school athletes who mostly had no reported history of concussion.
Materials and methods
Participants
Participants were 50 adolescent patients being treated for concussion (mean = 14.5 years +/–0.3, range 10–18; 52% male) and 36 parents of those youth (not all parents opted to participate in the study with their children). Eligibility criteria included being a patient of the multidisciplinary concussion center between the ages of 10 and 18 years. All participants had a history of concussion, with over half (54%) of the youth having a history of two or more concussions. Parents and patients all had contact with a healthcare provider about the most recent concussion before study participation.
Methods
Statement of informed consent
Human subjects approval was obtained from the Institutional Review Board. All participants provided informed consent to participate in research, with minors providing written assent and their parent providing written consent.
Procedures
Parents and patients completed a demographic survey, including report of where participants received concussion education, and a concussion knowledge survey culled from a previously developed survey by Kurowski et al., based on the CDC’s HEADS UP education program materials [23]. The knowledge survey was administered at the beginning of a standard follow-up clinical visit, and no specific education was provided prior to survey administration. Most patients had been previously evaluated within this clinic setting and had received some type of education from an outside source, including the local ED, an athletic trainer, or a primary care physician. Patients were referred to this clinic from throughout the region, and thus the type of education previously received varied widely. Once a patient was at the concussion center, they were seen by one of seven physicians and may have been paired with several different trainers, therapists, or other medical trainees. Typical new visits were 60 minutes long and included verbally provided concussion education as needed. Return visits were typically a 45-minute visit with a physician and often a paired visit with an athletic trainer or physical therapist. Most physicians provided an after-visit summary that included evidence-based concussion education handouts developed by the clinic and in line with the current consensus guidelines as well as a written return to play guideline, though this practice was not formalized or required across providers. Educational handouts were also provided at this institution’s emergency room. Patients were approached for participation in the study at a follow-up visit to ensure that the opportunity for clinical education within this clinic had been present for all patients. Patients in this clinic are followed as long they report concussion symptoms, and as such, the time since injury and timing of any concussion education was highly variable across patients.
The knowledge survey included 10 true/false general knowledge questions and 12 yes/no symptom knowledge questions. An example true general knowledge statement was “an athlete should not continue to play sports while having a concussion;” an example of a false general knowledge statement was “a concussion is any injury to the head.” Examples of true symptoms of concussion included “difficulty concentrating” or “headache;” and examples of false symptoms of concussion were “neck pain” or “tingling in feet.”
Statistics
Statistical analyses were completed using a 2×2 chi-square comparison approach with the published results of Kurowski et al. [23] from 500 high school athletes [23] compared to data collected from the current patient sample of previously concussed youth and their parents. Specific comparisons included the following: concussed youth (i.e., patients) compared to high school athletes, concussed youth patients compared to their parents, and high school athletes compared to the parents of the concussed youth patients. To evaluate for predictors (i.e., sex, age, and multiple concussions) of increased knowledge of concussion in the patient population, summary variables were created reflecting the total of correct general knowledge items and the total of correct symptom items.
The multiple concussion groups were defined as follows: Multiple Concussion, patients with a history of at least one concussion prior to the injury for which they were currently receiving treatment (n = 27); and Single Concussion, patients who were being treated for their first concussion (n = 23). Paired t-tests were calculated to determine if patients with multiple concussions had a more substantial knowledge base than those with a single concussion.
Results
Demographics of the clinical sample and the comparison group of high school students are provided in Table 1. Table 2 presents self-reported education sources. Youth in this cohort performed similarly to the previously published sample of high school athletes at correctly identifying concussion-related symptoms, with an overall accuracy of 72.3% in the current sample (Figs. 1 2). However, youth in the study cohort incorrectly identified neck pain as a concussion-related symptom (X2 < 0.001) and were less likely than the published sample of high school athletes to correctly associate slowed reaction time with concussion (X2 = 0.03). In both samples, a majority (68% of the clinical patient group and 81% of the high school athletes) incorrectly reported that concussion causes physical brain damage that can be seen on magnetic resonance imaging (MRI) or computed tomography (CT) scans. In both samples, youth incorrectly reported that any injury to the head causes a concussion (64% of the clinical patient group and 76% of the high school athletes).
Demographics for All Patients and Previously Published Comparison group
Demographics for All Patients and Previously Published Comparison group
Self-reported Previous education received (% of sample receiving education in any fashion from the following sources)
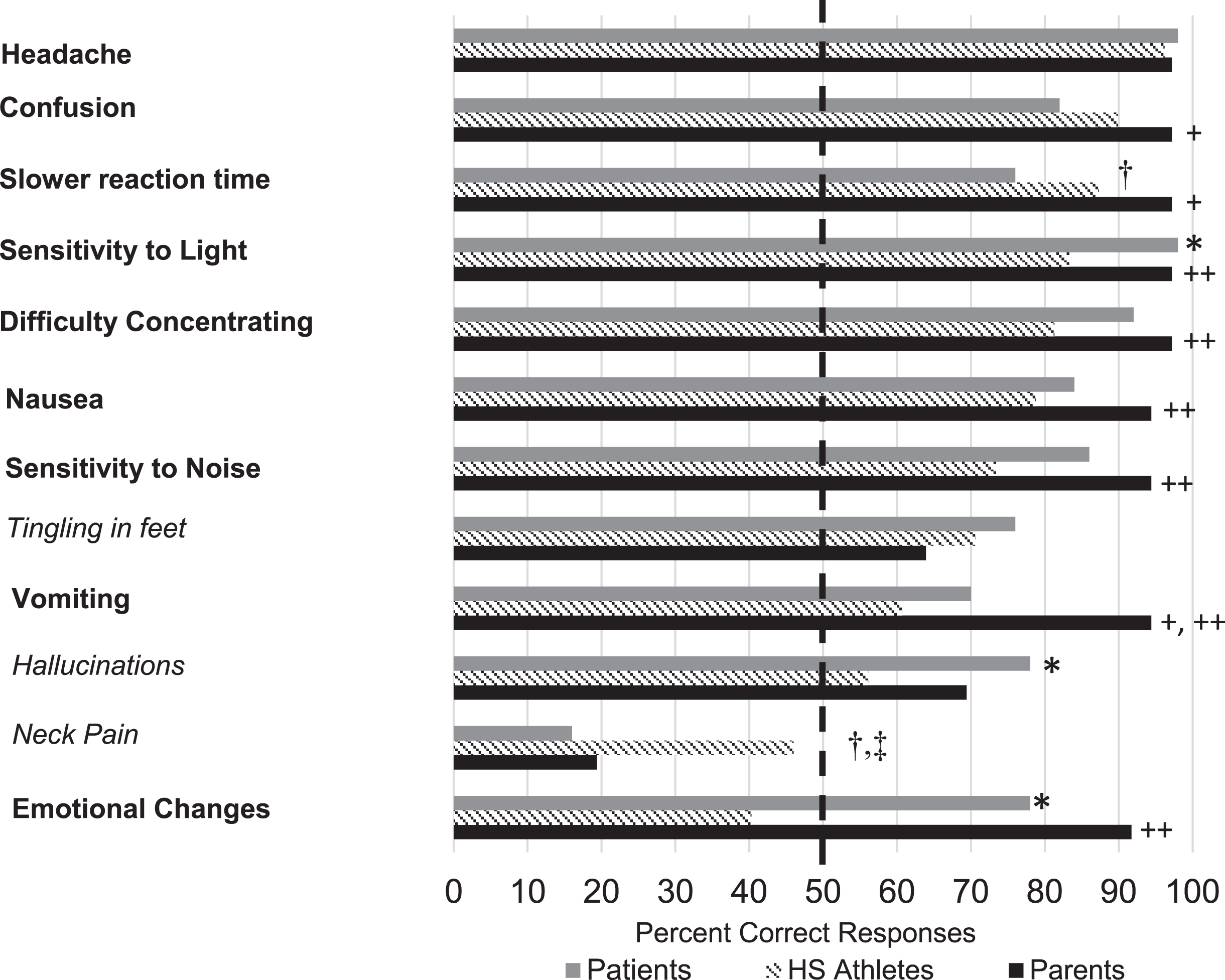
Percentage of correct responses across groups for the Concussion Symptom Survey. Note. Symptoms presented in bold are true and those presented in italics are false. The dotted line reflects the 50th percent. HS = high school. *Comparison with concussed youth having greater accuracy than high school athletes, p < 0.01. †Comparison with high school athletes having greater accuracy than concussed youth, p < 0.05. ‡Comparison with high school athletes having greater accuracy than parents of concussed youth, p < 0.01. +Comparison with parents of concussed youth having greater accuracy than concussed youth, p < 0.05. ++Comparison with parents of concussed youth having greater accuracy than high school athletes, p < 0.05.
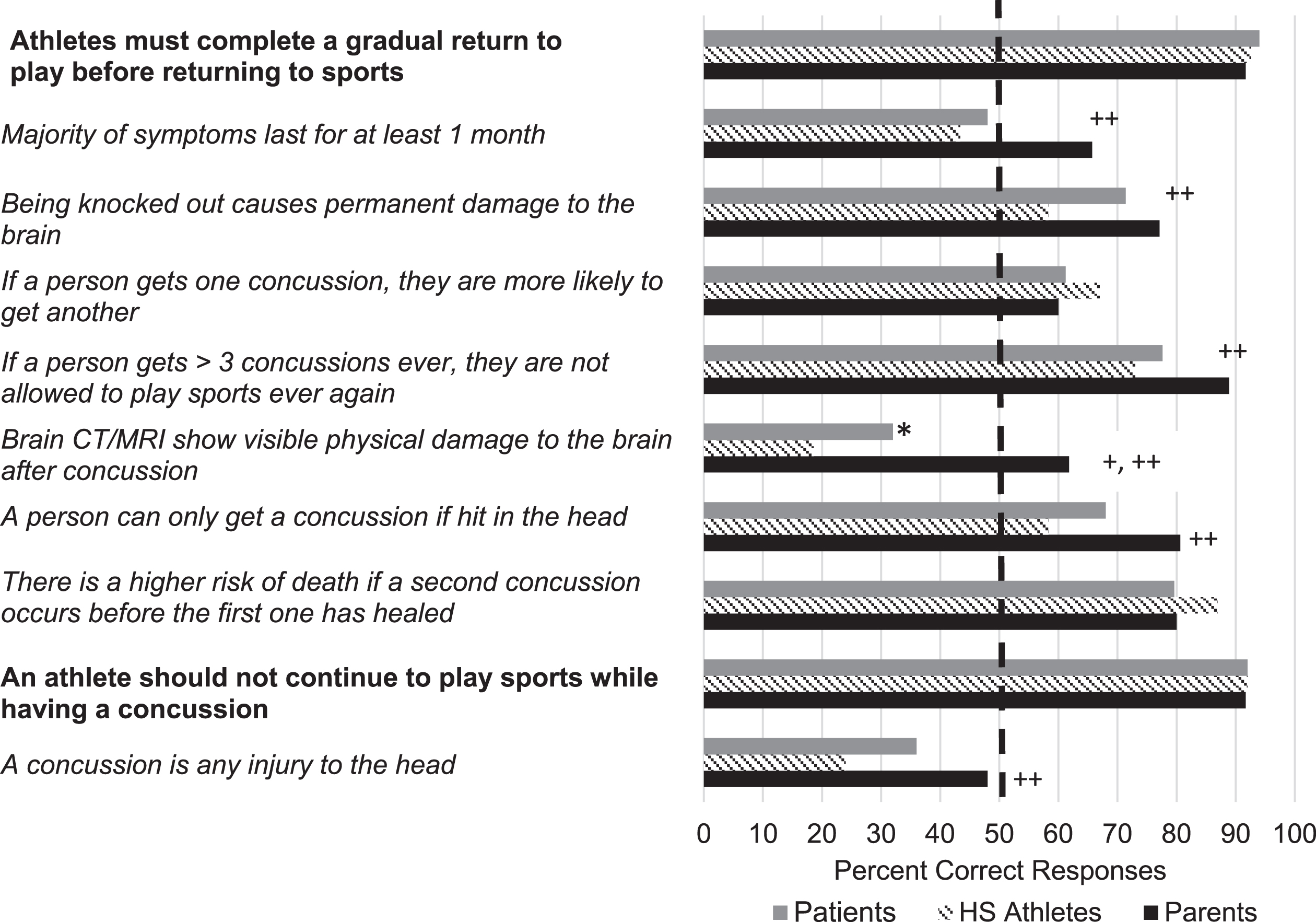
Percentage of correct responses across groups for the Concussion General Knowledge Survey. Note. Those statements presented in bold are true and those presented in italics are false. The dotted line reflects the 50th percent. HS = high scool. * Comparison with concussed youth having greater accuracy than high school athletes, p < 0.01. +Comparison with parents of concussed youth having greater accuracy than concussed youth, p < 0.05. ++Comparison with parents of concussed youth having greater accuracy than high school athletes, p < 0.05.
Figures 1 2 display the proportion of the sample that responded correctly to symptom-focused knowledge questions and the percent correctly responding to true/false concussion statements, respectively. Across all three groups, the majority incorrectly answered that concussion is separable from injuries to the head (45% or less of each group answering items correctly) and that most symptoms should not last longer than one month (parents, 65.7%; patient group, 48%; high school athletes, 43%) (Figs. 1 2). Low correct response rates were noted concerning the recognition of neurological consequences after injury. The proportion of correct answers was low for additional items: 1) Imaging may not show significant changes even when a concussion had occurred (61.8% parent group correct, 32% patient group, 19% high school athletes), 2) Concussion risk increases with multiple injuries (parent and youth groups 60–68% correct), and 3) Being “knocked out” does not necessarily cause permanent brain damage (58–77%). Paired t-test comparisons between youth in the Multiple Concussion and Single Concussion groups found no significant difference (p > 0.5). No significant differences in total score were observed based on gender or age within the clinical youth sample (p > 0.3).
Parents and patients in the cohort were equally accurate in identifying most concussion-related symptoms (Figs. 1 2), except that more parents correctly identified emesis and slowed reaction time related to concussion (X2≤0.006). Compared to the high school athlete sample, parents in the cohort were significantly more accurate in identifying most concussion-related symptoms, except for neck pain (X2 = 0.003).
This study found that most subjects correctly answered questions about the primary symptoms of concussion and return-to-play protocols. However, this research found significant knowledge gaps about the definition, diagnostic processes, comorbid conditions, and long-term risks/outcomes of concussion among subjects recently exposed to concussion education in the primary care or acute care settings. Regarding overall accuracy on the knowledge test, the sample’s performance (72.3%) was comparable to the published sample of high school athletes (68.6%) with regard to overall accuracy. These findings support the idea that current educational approaches of youth athletes in the community through school personnel, coaches, or resources like HEADS UP are as effective as direct medical care in educating youth about symptoms, the need for follow-up, and guidelines for return to play [16]. The results may also suggest that current concussion educational approaches for children with suspected or diagnosed concussions may fall short in addressing a patient or parent’s overall understanding of concussive injury and prognosis in several ways.
Neck-related injury symptoms were not recognized as separate from concussion by the majority of the study subjects, and the study cohort performed worse than a previous study of high school athletes. The specialized multidisciplinary clinical approach allowed for concurrent treatment of a neck injury as part of the comprehensive model and may partially explain the misattribution of neck pain as a post-concussive symptom in patients. While patients likely benefit from the comprehensive and coordinated clinical care available, this highlights the possibility that patients may require specific education within comprehensive care settings to help them differentiate between concussion symptoms, symptoms of concurrent injuries, and the potential for overlapping symptom profiles. The Sport Concussion Assessment Tool - 5th Edition (SCAT5 [28]) is a commonly used sideline assessment tool for evaluating concussion and includes a list of common concussion symptoms along with brief physical and neurological assessment. The SCAT5 is used only by physicians and licensed health care providers, who may also use the symptom checklist as a part of follow-up care and serial assessment. In addition to common signs and symptoms of concussion in HEADS UP education used widely in schools, the SCAT5 also asks about neck pain and advises evaluation of the neck during sideline assessments when concussive injury is a concern. Individuals evaluated for concussion by medical providers therefore also likely received assessment and follow-up questioning about neck pain/function, which may lead to confusion among patients.
Significant knowledge gaps were also seen in how youth and parents understood the definition and prognosis of concussion. The majority of youth patients incorrectly endorsed that a concussion occurs from “any hit to the head,” that brain damage from concussion can be seen on an MRI/CT scan, and that symptoms from concussion typically last longer than one month.
Other studies have identified similar knowledge gaps in youth, parents, and coaches regarding concussion diagnosis, evaluation, and symptom resolution presentation [11, 29]. Merz and colleagues surveyed a sample of adults in the general public and found an approximate 60% accuracy rate on a wide-based concussion knowledge questionnaire [21]. This clinical sample of individuals being treated in a specialty clinic for a diagnosed concussion unexpectedly performed worse than the published sample in identifying symptoms and accurate general information about concussion. This may suggest that increased exposure to concussion information results in an increase in conflicting or overlapping information, hampering educational efforts. The HEADS UP literature often used by school programs does not focus on how concussion is diagnosed, medical evaluation techniques and purposes, or long-term neurological outcomes of concussion [16]. Following injury, concussion education is provided in EDs and outpatient clinical settings, where providers must focus education on the needs of the referral complaint, often with strong emphasis on symptom management. As a result, education efforts may not address the purpose and limitations of diagnostic tools or expectations for prognosis, leaving families to explore other information sources.
The heavy emphasis of educational efforts on improving identification of injury may lead athletes and families to misinterpret or generalize risks associated with concussions. Many early efforts to improve concussion education stemmed from concerns that concussion severity and brain injury risk were underappreciated in youth who were not pulled quickly enough from sport [7, 10]. One potential consequence of this attempt to increase awareness about concussions may be an inflated sense of risk by the public. Patients and families have also been shown to interpret educational information in light of personal history and concussion beliefs [3, 30]. In a sample of the general public, the term “brain injury” was associated with more negative attributes than “head injury,’ and this pattern was also seen in participants with a previous history of concussion [19]. Additional sensationalized cautionary tales in the media and anecdotal examples further complicate the picture for families seeking education [27]. Evidence suggests that there is an increased risk for prolonged recovery in patients who withdraw from safe re-entry to sports or school due to inaccurate knowledge about concussion diagnosis and prognosis [31]. Given this complexity, the type and timing of education provided to patients with concussion needs to be carefully considered. The type of education required to teach concrete guidelines related to symptom management and return to play may be separable from the most optimal type of education needed to discuss prognosis and long-term outcomes following concussion in youth athletes.
Limitations
Conclusions drawn from this study need to be interpreted considering several limitations. First, the sample size within the study was relatively small and, as a result, it was not possible to examine the effects of age or injury factors as they related to knowledge base. Moreover, the power was limited by small sample size and, thus, lack of significant findings about gender differences or differences based on concussion history may also reflect low power as opposed to absence of a genuine difference. Additionally, due to this project’s natural clinic environment, the way in which clinical education was provided to patients was not accounted for or controlled within the study. Education about concussion primarily relied on conversation between provider and patient and/or handouts given during previous visits. Depending on patient needs, some patients would have been seen only by a physician; however, others may also have been seen by a combination of team members, including athletic trainers, physical therapists, neuropsychologists, and medical assistants, all of whom provide various levels of education within the clinic. It was not possible within this study to evaluate the exact nature of the education offered to each patient either from within the clinic, from their online research, or from the school and/or primary or acute care settings (e.g., pediatrician, school athletic trainer). Further analysis of the content, timing, and focus of the education would be necessary to fully understand the effect of clinic-based psychoeducation for concussion. In the authors’ view, the purpose of the study was to look at the “real world” education within a physician clinic rather than a controlled study examining the effectiveness of any specific educational material on any specific patient population. Limited conclusions can be drawn about best practices in education from this study, but they may be generalizable to other real-world clinical formats and provide at least a reasonable commentary on how “practice as usual” may not be meeting intended concussion education goals.
Another important limitation to address is related to the psychometric properties of the survey. To the authors’ knowledge, the survey has not been evaluated for its psychometric properties and so methodological problems related to specific items cannot fully be ruled out. It may be questioned whether items answered incorrectly were confusing or misunderstood. If the item wording was problematic, then lower accuracy rates are not necessarily indicative of knowledge gaps on the part of the study participants. As noted in the discussion, other studies have shown similar knowledge gaps using other approaches to measuring concussion knowledge, and therefore the study findings fit a pattern that exists in the wider literature examining concussion knowledge; however, specific item level evaluation of the survey is needed to rule out potential methodological weaknesses.
Future directions
The study findings highlight the continued knowledge deficit among youth and parents even in patients who have been treated by a medical provider for concussion. There is a need to evaluate and analyze the educational content and methods provided by outpatient clinics and acute care settings that manage and assess concussions. The substantial variability in patient and parent knowledge surrounding concussion definition, diagnostic processes, long-term risks, and prognosis suggests that the types of education traditionally focused on in acute care settings do not fully address the comprehensive education needs critical to improving long-term concussion outcomes. Educational materials may need to be tailored to the patient’s stage of recovery, developmental level, and specific symptoms profile to help ensure all youth and family members receive accurate information that is well understood. The delivery method should also be based on recovery-related factors, including parent and child attitudes toward concussion, the youth’s goals concerning return to play, and previous clinical education by health care providers. In scenarios where comprehensive treatment is provided, it may be important to provide education about which treatments are meant to address which symptoms. Specifically, treatment of neck injury should be differentiated from treatment for concussion, and education should be provided about the reasons that both treatments are important (e.g., headaches could be caused by neck injury and then are separable from a headache due to concussion).
The results also suggest that there may be a specific benefit to spending time providing education about what a concussion is from a neurological perspective, how concussion is diagnosed, and what the long-term expectations for recovery are following concussion. This deeper understanding of concussion, rather than simple focus on post-acute symptoms of concern and return-to-play protocols, may be more important in clinics where post-concussion syndrome or complicated recovery is of significant concern. Incorrect beliefs about concussion symptoms have been linked to prolonged symptoms reporting, extended periods of rest, and withdrawal from activity that has potentially iatrogenic effects. For patients with an incorrect understanding of concussion, additional comprehensive education may be essential to prevent iatrogenic effects of education focused solely on risks associated with concussion. Future research that looks specifically at the types and timing of education provided to patients during specific stages of recovery (e.g., acutely injured vs. chronic symptoms) may be helpful in better understanding the role of concussion education in concussion treatment.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors have no conflicts of interest to report. This funding was not supported by any grants.
Ethical considerations
Human subjects approval was obtained from the Institutional Review Board (HUM00123216). Initial study approval occurred on 11/2016. All participants provided informed consent to participate in research, with minors providing written assent and their parent providing written consent.