
Abstract
PURPOSE:
This initiative aimed to assess adherence to Scottish Rite for Children’s serial casting protocol for children with idiopathic toe walking (ITW), factors related to adherence, and outcomes after education regarding the protocol.
METHODS:
60 patients aged 7.1±2.7 years who completed serial casting were examined at baseline phase (n = 30) and post-education phase (n = 30). Protocols include weekly serial casting for 4 to 6 weeks to achieve 10° of ankle dorsiflexion (ADF) passive range of motion (PROM) with knees extended (KE), assessing the foot posture index (FPI-6) and single leg stance (SLS). Baseline phase evaluated adherence to protocols. Education phase evaluated factors related to adherence and education regarding serial casting findings. Post-education phase evaluated the impact of the education phase.
RESULTS:
Serial casting averaged 4.8±1.5 weeks (n = 60). ADF PROM was measured with 100% adherence. ADF PROM KE averaged –10.7° pre-cast and significantly improved to +6.5° post-cast (n = 60), and it significantly improved post-cast post-education (p = 0.04). FPI-6 and SLS adherence significantly improved post-cast post-education. FPI-6 total score averaged +5.3 at baseline and +5.8 post-cast (n = 35).
CONCLUSION:
Education of staff in serial casting protocols improved adherence and patient outcomes. Patients with ITW and ADF PROM KE –10° benefit from serial casting to improve PROM and to allow for orthotic use post-casting.
Introduction
Toe walking is defined as the inability to achieve a heel strike at initial contact of the gait cycle, along with the lack of full foot contact during stance phase, thus resulting in an individual ambulating on their toes [1]. Toe walking in children can be a sign of a neurologic disorder and sometimes presents in children with language or cognitive delays. However, in approximately 5% of healthy children, no cause or condition can be found for the child’s toe walking; this is defined as idiopathic toe walking (ITW) [2]. Treatment options for ITW include therapeutic exercises, sensory-based interventions, locomotor training, botulinum toxin A injections, orthotics, serial casting, and surgery. Physical therapists (PTs) routinely perform serial casting as a conservative treatment approach for patients with ITW who have developed secondary ankle plantarflexor contractures. Serial casting is recommended in children who toe walk and who have limited ankle dorsiflexion (ADF) [3], as this treatment method is effective in improving ADF passive range of motion (PROM) [4–7]. Serial casting lengthens the components of calf musculotendinous units and restores the normal muscle length tension relationship at the ankle, which ultimately allows for plantigrade gait [8]. Serial casting has been a controversial topic over the years, as it has demonstrated improvements in ADF PROM in children with ITW, but the gains have been short term in current published studies [9, 10].
This clinical quality improvement (QI) initiative was designed to assess if serial casting outcomes adhered to Scottish Rite for Children’s serial casting protocols (baseline phase), assess factors related to adherence and education regarding serial casting findings (education phase), and assess the impact of the education phase (post-education phase). Specifically, this initiative aimed to report on the physical therapy department’s adherence at baseline and post-education to 1) the recommended number of weeks of serial casting, 2) achieving 10° of ADF PROM with knees extended (KE) post-casting, and 3) assessing ADF PROM, Foot Posture Index (FPI-6), and timed single leg stance (SLS) pre- and post-cast. The secondary aim was to report outcomes (ADF PROM, FPI-6, and SLS) pre- and post-serial casting.
Methods
Setting and context
A QI team was established in October 2019 with the specific, measurable, achievable, relevant and time bound (SMART) aim of assessing adherence to the current clinical serial casting protocols and the ultimate goal of deciding whether to change Scottish Rite for Children’s protocols and/or to further educate PTs regarding serial casting findings. The team consisted of the medical doctor who oversaw the toe walking clinic, a QI program manager, and 2 PTs. The QI core team met for several months to decide on the scope of the project and needed steps. The team identified 30 patients who had completed a series of serial casting from October 2017 when the clinical protocols were implemented until December 2019. In January 2020, the PTs collected retrospective data from the 30 most recent patients with a diagnosis of ITW who completed serial casting performed by a PT at this tertiary-care pediatric hospital. In February 2020, after assessing adherence to protocols, the QI team focused on improving adherence by educating serial casting PTs on the findings from this project. In December 2021, the team reviewed the next 30 charts of patients with ITW to assess the impact of the education for the post-education implementation phase from March 2020 to July 2021.
Patients with ITW from Scottish Rite for Children’s toe walking clinic were referred to PTs for serial casting when their ADF PROM KE was –20° to 0°. The medical providers in the toe walking clinic performed a comprehensive neurological evaluation to rule out possible neurological causes of toe walking. Children who were found to have a neuromotor etiology for toe walking were excluded from the ITW casting protocol. Neuromotor etiologies included patients with abnormal tone seen in cerebral palsy, tethered cord, developmental delay, autism, or a neuropathy such as Charcot Marie Tooth. Other patients who had learning differences such as attention-deficit/hyperactivity disorder and dyslexia were excluded due to concerns that these factors may also influence serial casting duration and outcomes. Patients were identified by their diagnosis of “idiopathic toe walking” and PT visit type of “serial casting” in the electronic medical records. This project was undertaken as a QI initiative at Scottish Rite for Children and, as such, was not formally supervised by the Institutional Review Board per their policies.
Measurement
The project included 60 patients (43 males, 17 females) with ITW who received serial casting by PTs at Scottish Rite for Children from October 2017 to July 2021 and whose average age was 7.1 years (range: 1.7–12.9 years). No patients previously received botulinum toxin injections. Nine PTs performed the serial casting, all of whom were trained to follow the toe walking protocol and completed serial casting clinical competency training for administration and documentation of the assessments. Clinical competency progresses from observation to direct supervision to indirect supervision to peer support to independence. The clinical toe walking protocols included below-knee serial casting for 4 to 6 weeks with the goal of achieving 10° ADF PROM KE to promote a plantigrade foot position. ADF PROM less than 10° has been defined as an ankle equinus contracture [11, 12]. Cast changes were typically done on a weekly basis. For patients with significant gastrocnemius tightness (–10° ADF PROM KE or less), PTs issued a knee immobilizer after collaborating with the referring provider; knee immobilizers were provided for night-time wear to increase gastrocnemius stretching and were usually worn on alternating legs every night to promote tolerance.
A technician prepared patients for casting with one layer of Delta-Net® Stockinette ringlets donned at the inferior and distal aspect of the cast. Webril™ Cotton Undercast Padding Regular Finish was applied with thicker layers at bony prominences along the toes, ankle, and proximal tibia. Scotchcast™ Soft Cast was then applied in a spiral pattern. Multiple layers of soft casts focused at the foot and ankle were used to increase rigidity. The ankle was kept in subtalar neutral to promote stretching through the ankle and not the midfoot. In patients who pronated, the foot was placed in varus and the first ray was elevated to maintain neutral alignment. For the first cast, patients were not stretched to their end range to promote tolerance to casting. Subsequent casts entailed the PT stretching the patient to their maximal end range position. Caregivers removed the bilateral casts at home the night before the child was casted again. If ADF PROM did not change after 2 successive casts, then serial casting was discontinued.
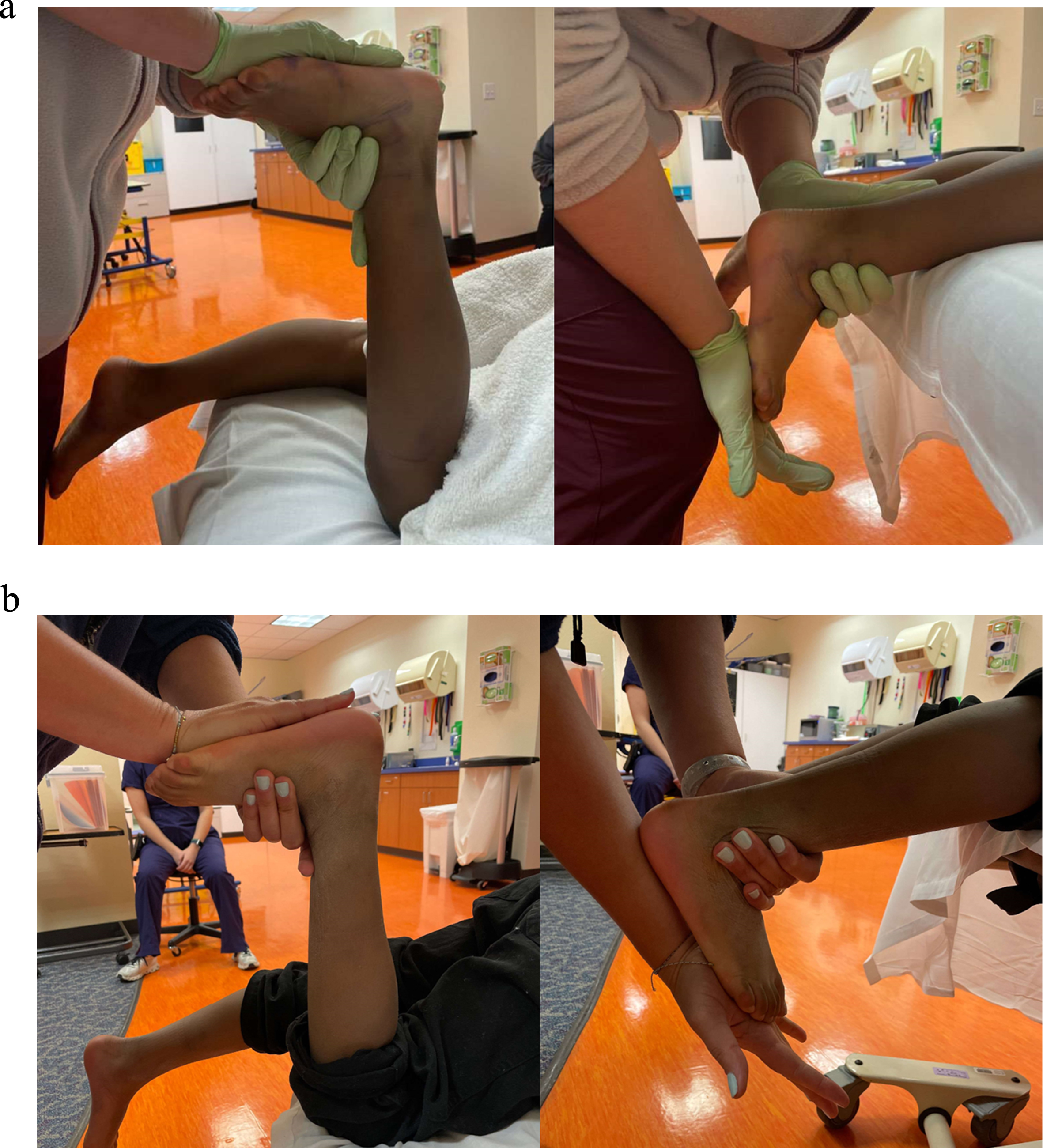
ADF PROM was measured in prone since this was the position that the patient was in when casting. ADF PROM was measured with the axis of the goniometer at the lateral malleolus, the stationary arm parallel to the fibula, and the moving arm along the fifth metatarsal. Prone was preferred to sitting for PROM measurements so that the casting therapist had more force to stretch the ankle musculature, especially in older, stronger patients. Clinical images of the foot dorsiflexed with the knee both flexed and extended were taken to verify ankle position. It was important to maintain neutral ankle and foot alignment when measuring ADF PROM to ensure that the movement was coming from the ankle and not the midfoot.
Scottish Rite for Children’s toe walking protocols also included documenting the FPI-6 to screen for mid-foot break prior to and after serial casting. If the PT had concerns about pes planus or pronation developing during serial casting, the FPI-6 was documented again, and the referring provider was contacted to determine whether casting should continue. The FPI-6 consists of 6 criteria, each criterion scored on a scale of –2 to +2. A “normal” foot posture total score is +4 or slightly pronated once a child turns 6 years old [13, 14]. Research on the FPI-6 is typically conducted in children 6 years and older [15–17] since the plantar arch does not typically develop until age 6 [18]. The FPI-6 is reliable in children as young as 3 years old [19] and is valid [15–17].
Timed SLS was used pre- and post-casting as a functional balance measure. Patients were asked to stand with their hands on their hips and with their opposite leg flexed to 90°. The test was stopped when the flexed leg bent to less than 45°, patients took their hands off their hips, or patients took a step.
The following data was entered into a spreadsheet by a staff member after reviewing patients’ electronic medical records: date of birth, date of visit, gender, date of first and final cast, initial and final ADF PROM with knees flexed (KF) and KE, FPI-6 scores, and timed SLS scores. After data was entered, the project lead reviewed the data of each patient to ensure accuracy.
Statistical analysis
Means and standard deviations were used to describe continuous variables. Paired t-tests were used to compare ADF PROM, FPI-6, and SLS scores pre- and post-cast and pre- and post-education. The right and left sides were averaged to determine ADF PROM, FPI-6, and SLS scores. Logistic regression analysis with backward elimination method was performed to assess for gender and age associated with adherence to protocols both pre- and post-cast and odds ratios (OR) and 95% confidence intervals were reported. A receiver operating characteristic (ROC) curve analysis was run to identify an age threshold value for adherence to protocols. Significant differences were based on a p-value of 0.05. Statistical analyses were performed using SAS/STAT (version 9.4). The intraclass correlation coefficient (ICC) was used to assess the test-retest reliability for the FPI-6 total score.
Results
Baseline phase (n = 30)
The total number of weeks of serial casting averaged 4.5±1.1 weeks, which adhered to the institutional protocol of 4–6 weeks of serial casting. Nine patients had difficulty tolerating the casts due to skin injury (n = 5), calf or heel pain (n = 2), or concerns of cast integrity (n = 2). Skin injury included scratch abrasions at the anterior ankle or distal tibia or heel, bruise at anterior ankle, and skin peeling at the great toe. Concerns of cast integrity were a cracked cast from ambulating without a cast shoe and an older patient who broke through the casts. Casting was discontinued early for the latter despite attempts at multiple layering. The team educated the therapist afterward that a strut of fiberglass could have been placed along the posterior aspect of the cast to add sturdiness.
ADF PROM was measured in all 30 patients pre- and post-cast, reflecting 100% adherence to the protocol of measuring PROM KF and KE (Table 1; Fig. 1). Pre-cast, ADF PROM averaged –5.8° KF and –10.6° KE overall. The lowest pre-cast ADF PROM KE was –45°. Post-cast, ADF PROM significantly improved to an average of +10.2° KF and +5.5° KE overall (p < 0.001), which did not adhere to the protocol of 10° ADF PROM KE.
Ankle dorsiflexion, Foot Posture Index, and Single Leg Stance scores pre- and post-serial casting at Baseline Phase and Post-Education Phase
Ankle dorsiflexion, Foot Posture Index, and Single Leg Stance scores pre- and post-serial casting at Baseline Phase and Post-Education Phase
*: p < 0.05.
a. Pre-cast ankle dorsiflexion passive range of motion with knee flexed and extended. b. Post-cast ankle dorsiflexion passive range of motion with knee flexed and extended.
The FPI-6 was assessed in 11 patients both pre- and post-cast, reflecting 37% adherence (Table 1). Pre-cast, the FPI-6 total score averaged +5.3 overall, indicating a “normal” foot posture. Post-cast, the FPI-6 did not significantly change, averaging +5.0 overall. Due to the low adherence and to help determine whether the FPI-6 should remain part of the protocol, the reliability of the FPI-6 at Scottish Rite for Children was evaluated. A cohort of 3 of the 9 serial casting PTs assessed the posture of 20 feet/ankles in 10 children using the FPI-6. Interrater reliability of the FPI-6 score of the 3 PTs was excellent (ICC = 0.94 [95% CI 0.84–0.98]). Timed SLS was measured in 10 patients both at baseline and post-serial casting, reflecting 33% adherence (Table 1).
The QI team met with the casting therapists as a group, followed by meetings with individual casting therapists to assess factors of non-adherence and the benefits of adherence to the clinical protocols. A possible reason for not achieving 10° ADF PROM KE was not casting for the full 6 weeks when ADF PROM KE plateaued after 2 successive casts (n = 10), when families did not return to their follow-up serial casting visit (n = 3), when a patient broke through the casts (n = 1), or due to concerns of midfoot deformity (n = 1). The team educated serial casting PTs on ensuring that ADF PROM did not change for 2 weeks before discontinuing casting. The team reviewed the benefit of patients achieving an optimal gait with 10° ADF PROM KE.
Possible factors of non-adherence to protocols for assessing the ankle/foot posture with the FPI-6 include patients having difficulty balancing, standing stationary or who were flat footed secondary to limited ankle motion and associated impairments. PTs may have forgotten to perform the FPI-6, since it was not built into their post-cast documentation notes. Or PTs may not have had buy-in regarding the clinical importance of assessing the ankle/foot posture with the FPI-6. Finally, the FPI-6 assessment itself can be time consuming.
Adhering to this part of the protocol can have benefits such as informing casting management for both the casting therapist and referring provider by ensuring that casting does not cause unfavorable foot posture changes, including minimizing the risk of mid-foot breakdown. FPI-6 scores can also provide a baseline for patients and families regarding foot and ankle posture. When casting, the FPI-6 results inform the position of the ankle and foot in the cast. For example, a foot that is more pronated should be placed in more varus in the cast to maintain neutral alignment. FPI-6 results might also inform orthotic fabrication with regard to supporting or posting the forefoot and hindfoot.
A possible factor of non-adherence to protocols for measuring SLS is that younger children may have difficulty tolerating the test due to their developmental milestone status. Also, performing a SLS immediately post-cast removal may not be ideal due to altered weightbearing during casting and a likely change in standing position after casting to which the patient is not accustomed. SLS scores may also decline due to ankle and foot weakness from prolonged immobilization during casting and lengthened heel cord tendons.
The benefits of performing the SLS include that it is a functional outcome that is meaningful to patients. The SLS is quick and easy for a PT to administer. This functional test may indicate whether a course of outpatient physical therapy is warranted to improve balance by use of an ankle strategy. Although SLS outcomes did not deteriorate overall despite the bout of serial casting, some patients demonstrated a less efficient hip strategy to balance if their ankle strategy failed to keep their center of gravity over the base of support.
In February 2020, after assessing adherence to protocols, the QI team focused on improving adherence by educating serial casting PTs on the findings from this project. The team mitigated barriers to adherence by discussing the benefits of adherence to the protocols of achieving 10° ADF PROM KE and performing the FPI-6 and SLS. The team reviewed existing documentation templates which already included the FPI-6 and SLS for easy reference, and PTs were reminded to remeasure outcomes post-casting. The team also advocated taking clinical images of the components of the FPI-6 for easy comparisons to pre- and post-cast and to assist the casting therapist in scoring the FPI-6. The team also recommended improving education for families about what to expect during a course of serial casting to proactively address concerns from parents about pain and skin integrity, including advising patients to avoid scratching their skin immediately post-cast removal. The QI team checked in with the casting PTs and referring providers through recurring quarterly virtual meetings to discuss updates to protocols and any questions regarding serial casting practices.
Post-education phase
In December 2021, the team reviewed the next 30 charts of patients with ITW who received serial casting to review the impact of the education. The total number of weeks of serial casting averaged 5.1±1.7 weeks. Five patients had difficulty tolerating the casts due to pain at dorsum of foot, heel, or calf (n = 3) or skin injury (n = 2). Skin injury included scratch abrasions at the calf and skin flaking at the heel. Casting was not discontinued early in these patients.
ADF PROM was measured in all patients, reflecting continued 100% adherence to the protocol. Pre-cast, ADF PROM averaged –4.5° KF and –10.9° KE overall. The lowest pre-cast ADF PROM KE was –35°. Post-cast, ADF PROM significantly improved to an average of +12.9° KF and +7.6° KE overall (p < 0.001), which is a few degrees short of the protocol of 10° ADF PROM KE. ADF PROM was significantly higher post-cast post-education compared to baseline for both KF (p = 0.02) and KE (p = 0.04). A post-hoc power analysis with 80% power and 5% significance level with a 2-sample t-test with unequal variance revealed that 53 patients per group were needed to detect a difference of 2.7° (2.1°) between groups. Patients did not achieve 10° ADF PROM KE when ADF PROM KE plateaued (did not change after 2 successive casts [n = 12]) and when one patient was reported to ambulate without an observed gait deviation at ADF PROM KE 5° for the post-education phase. Since 22 of the 60 patients’ ADF PROM plateaued (10 from the education phase and 12 from the post-education phase), age, pre-cast ADF PROM, and change in PROM was compared between patients whose ADF PROM plateaued between two successive casts and those whose PROM did not plateau. Patients who plateaued demonstrated significantly decreased pre-cast ADF PROM KF and KE than patients who did not plateau (–9.0° vs. –2.7°, p < 0.01; –14.5° vs. –8.3°, p < 0.01).
The FPI-6 was assessed in 24 patients, reflecting 80% adherence to the protocol (Table 1). Pre-cast, the FPI-6 total score averaged +5.2 overall, indicating a “normal” foot posture. Post-cast, the FPI-6 significantly increased to +6.2 overall (p = 0.03), which indicates a “pronated” foot. The casting therapists frequently noted that it was difficult to tell whether patients’ FPI-6 scores truly increased, since patients’ amount of pronation pre-cast may have been disguised by their inability to stand in a plantigrade position. Timed SLS was measured in 24 patients, reflecting 80% adherence (Table 1). The FPI-6 and SLS were not measured in children under 2 years of age who were too young to cooperate (n = 2) and by two newer therapists who were not trained by a PT of this QI core team (n = 3). After running logistic regression analysis for age or gender, increased age was positively associated with adherence to performing the SLS measurement (OR 1.32, p = 0.02;) but not the FPI-6 (OR 1.14, p = 0.21). Gender was not associated with adherence. A ROC analysis was run next and found that age 6.1 years (Area Under the ROC Curve [AUC] = 0.70) was the age threshold value for a higher chance of performing the SLS measurement.
Discussion
Improving the uniformity of serial casting practices to standardize care is a high priority at Scottish Rite for Children to increase patient safety, improve quality of care, and improve outcomes. Non-adherence to protocols was due to PT-related factors, patient-related factors, and the procedure itself. Through the evaluation of current clinical practices, post-cast ADF PROM KE of 10° was not achieved despite prolonged serial casting. Serial casting was discontinued before 6 weeks when ankle PROM plateaued (22/60), which may have been due to the child’s muscle length tension relationship, the soft casting material, or the procedure itself. Adding padding or hard casting especially in older children may improve stretch on the gastrocnemius, in addition to improving skin integrity and cast tolerance.
Few studies that include small sample sizes report ADF PROM immediately post-cast; a systematic review reported 3.1° improvement after 3 years [20]. Fox et al. also did not achieve 10° ADF KE immediately after casting, averaging +5.8° ADF PROM KE and a 4.7° improvement [5]. This project’s results contrast that of Engström et al. and Brouwer et al., who reported achieving 10° after serial casting and did not initiate brace wear after serial casting [4, 7]. However, ADF PROM KE of this patient population pre-cast was also significantly lower at –10.3° (n = 60) compared to Engström et al. and Brouwer et al.’s pre-cast ADF PROM KE at +4.3° (n = 26) and –3.5° (n = 8) [4, 7]. This project’s post-cast improvement in ADF PROM KE was slightly higher (17°, n = 60) compared to Engström et al. and Brouwer et al.’s 6.6° and 13° improvements [4, 7]. Another probable reason for lower ADF PROM is the presence of midfoot deformity which may not have been sufficiently assessed due to the patient’s inability to stand in a plantigrade position pre-cast. Casting PTs should be cautioned of the difficulty of accurately assessing the foot/ankle posture of children using the FPI-6 in patients with ITW who are unable to stand plantigrade before casting.
While 10° ADF PROM KE is a justified PROM goal for functional activities beyond plantigrade gait such as jumping or walking on an incline, serial casting is a precursor to brace wear for ITW treatment at Scottish Rite for Children. Therefore, referring medical providers were not concerned about PTs not achieving 10°. The larger goal was that children achieve neutral ADF PROM KE to tolerate ankle foot orthosis (AFO) wear post-serial casting, preferably initiating an intensive brace wear schedule if families were willing. Orthotists at Scottish Rite for Children typically set AFOs at 0° ADF PROM KE, and patients typically wear articulating AFOs which also promote continued ankle stretching. Furthermore, the clinical practice guideline on the PT management of children with ITW from Cincinnati Children’s Hospital recommends using articulated AFOs and PT intervention in children whose ADF PROM KE is between 5° to 10° [21].
ADF PROM of patients at Scottish Rite for Children pre-cast (–10.7° KE) was not only lower compared to previous studies but was similar to a previous study whose patients required surgery with ADF PROM averaging –10° KE [6]. The QI initiative highlights the performance of the conservative treatment approach of serial casting in patients with equinus contractures who may otherwise be considered for surgical intervention.
This QI team considered performing the Observational Gait Scale to capture changes at the initial contact and mid stance phase but found that children walk differently for healthcare professionals than they do at home when they are not being evaluated. Additional considerations included a stratified sampling approach to generate a more representative sample across all age groups and gender to make the results more generalizable. Furthermore, accepting less than 10° of ADF PROM KE for this population needs more research and information as to how these children tolerate AFOs and with toe walking outcomes. Results of this project cannot be generalized beyond the patient sample or this Scottish Rite for Children. Furthermore, a post-hoc power analysis revealed that more patients were needed to improve confidence in the results; statistical significance of improved ADF PROM KE post-cast post-education compared to pre-education (7.6° vs 5.5° KE) was demonstrated.
Educating casting PTs regarding serial casting outcomes was successful in increasing ADF PROM and adherence to clinical protocols including assessment of the foot/ankle posture with the FPI-6 and assessment of SLS. The data obtained through evaluation of Scottish Rite for Children’s current practices exposed areas for improvement in the comprehensive documentation by PTs for patients with ITW who receive serial casting. Increasing uniformity in serial casting procedures for children with ITW across Scottish Rite for Children will result in data that can be used to determine outcomes as a result of this intervention.
Conclusions
Although the goal of ADF PROM KE of 10° was typically not achieved after 4 to 6 weeks of serial casting, ADF PROM KE significantly improved in a patient sample after assessing factors related to non-adherence and educating casting therapists regarding the benefits of adherence to the protocols. Scottish Rite for Children’s patient population also demonstrated lower pre-cast ADF PROM compared to previous papers [4, 7], and patients were fitted with AFOs immediately after serial casting. The importance of assessing the ankle/foot posture with the FPI-6 and SLS was successfully reinforced as a quality and safety measure.
Footnotes
Acknowledgments
The authors wish to acknowledge Brenda House, Cameron Gray, Courtney Warren, Charter Rushing, Rosa Cooksey, Lindsay Chiu, and Steven Lacore for performing serial casting.
Conflict of interest
The authors have no conflicts of interest to report.