
Abstract
This systematic review assessed four measurement properties of measures (instruments) used by researchers to assess adherence to caregiver facilitated therapeutic activities (CFTA) for children in published research. The measurement properties considered in this systematic review were dyadic considerations, interpretability, reliability, and validity of the instruments used to assess adherence or compliance. Two databases (http://www.pubmed.gov and EMBASE) were searched for studies that reported adherence or compliance to CFTA prescribed by physiotherapists or occupational therapists or speech and language therapists. Papers included in this review were those that studied children less than 18 years old and or their primary caregivers. Data were extracted by the authors using a data extraction table adapted from the work of Bollen and colleagues (2014) and by rating the measurement properties of the adherence measures identified based on predefined rating criteria (see supplementary file and Table 1 respectively). The authors relied only on the published research articles and any associated published supplementary files/data. None of the 40 adherence instruments identified wholly fulfilled all the criteria of the four measurement properties assessed. The results of this systematic review show that the measures used by researchers for assessing adherence to CFTA generally lack validity, reliability, and dyadic considerations.
Introduction
In this paper, compliance and adherence are used interchangeably.
Adherence or compliance to prescribed therapeutic activity is the accurate performance of the activity in line with the prescribed frequency, duration, and quality of performance [1, 2]. In a systematic review by Bollen and colleagues [3], 61 measures for assessing self-reported adherence to unsupervised home-based exercise were examined for their psychometric properties. The authors found that only eight of the measures examined had positive to intermediate content validity, three had intermediate reliability, while none had positive interpretability. The work of Bollen and colleagues exposed the inadequacy of measures of assessing adherence that are commonly used in clinical research [3]. Research in adherence to caregiver facilitated therapeutic activity (CFTA) in the paediatric population has received significant attention recently but the measurement properties of the measures of adherence (methods/instrument for assessing adherence) to CFTA have received less attention.
Adherence requires behaviour or lifestyle changes corresponding with recommendations agreed upon with a healthcare provider [4]. The paediatric population receiving rehabilitation services are generally involuntary patients brought to therapy by parents or caregivers. Oftentimes, the rehab process extends beyond the clinic where the caregiver is required to facilitate the performance of therapeutic activities for the child or with them in the absence of the therapist. Such CFTA require behavioural or lifestyle changes by both the caregiver and the child. Therefore, measures of adherence to CFTA should consider the dyad (caregiver and child) and not just the facilitator or caregiver. Studies that investigated adherence to CFTA for children tend to focus on the caregiver and less on the child [5, 6]. An important phenomenon that should prompt the inclusion of the child in the assessment of adherence to CFTA is the psychological concept of health locus of control, which is the belief regarding the type or amount of control that an individual has on their personal health based on personal experience(s) [7]. The health locus of control in an individual with a health condition could be internal, meaning that they believe that they have control over their own health and are personally responsible for it. Conversely, a person with an external health locus of control believes that other people or factors around them are responsible for their health. This person believes that they have no control over their own health and are therefore not responsible for it. It is also possible that the health locus of control in one individual may be internal for some health issues and external for others. Health locus of control may affect the health behaviours of children, including compliance to prescribed therapeutic activity [8–10]. Therefore, it is imperative that methods of assessing adherence to CFTA should assess dyadic adherence instead of focusing solely on the adherence of the caregiver.
A caregiver is anyone who provides care for another person with a health condition. Caregivers may be family members, friends, or anyone within the social support network of persons with health conditions [11]. Their caregiving duties are voluntary and uncompensated. Thus, they are often referred to as informal caregivers as opposed to paid caregivers who are employed to lessen the caregiving burden of the family members. Given that the caregiving tasks of paid caregivers are considered routine activities within their job description, they were excluded from this review in order to focus on informal caregivers.
Study aims
This study aimed to identify measures of adherence to CFTA for children that have been used in published research and to assess the way published research papers report the measurement properties of the instruments they used to assess adherence. The CFTA considered in this study are those prescribed by physiotherapists, occupational therapists, and speech and language therapists. Also, the study aimed to document the existence or lack of four measurement properties in the identified measures of adherence. The first measurement property considered was content or construct validity expressed statistically by Pearson’s r value and its equivalents. This is the strength of the correlation between measurements obtained from an instrument compared to measurements obtained from a referent standard instrument that measures the same construct [12–14]. The second measurement property was reliability (inter-rater, or test-retest reliability, or internal consistency reliability) [13, 14]. This is the level of agreement between the measurement values obtained from repeated use of a measuring instrument either by one assessor or multiple assessors. It is also determinable by Pearson’s r value and its equivalents. The third property considered was interpretability which may be defined as either a clear rationale for determining meaningful changes in adherence, or a clear rationale for making differences in adherence between participants or changes in the level of adherence for individual participants over time meaningful [12]. Lastly, dyadic consideration has been considered as a dichotomous characteristic of adherence measures in this systematic review. This classified the measures of adherence as either with dyadic consideration (adherence of both the caregiver and the child), or without dyadic consideration (adherence of either the caregiver alone or the child alone) [15].
Methods
Two databases (http://www.pubmed.gov and EMBASE) were searched on the 11th of December 2020 for the following combination of keywords/key phrases: ((caregiver or family) AND (compliance or adherence)) AND (physiotherapy or occupational therapy or speech and language therapy). Broad search terms were used in order to retrieve the maximum number of relevant publications. The search results were then filtered to include human species and articles that have been written in the English language. The study selection process is shown in Fig. 1.
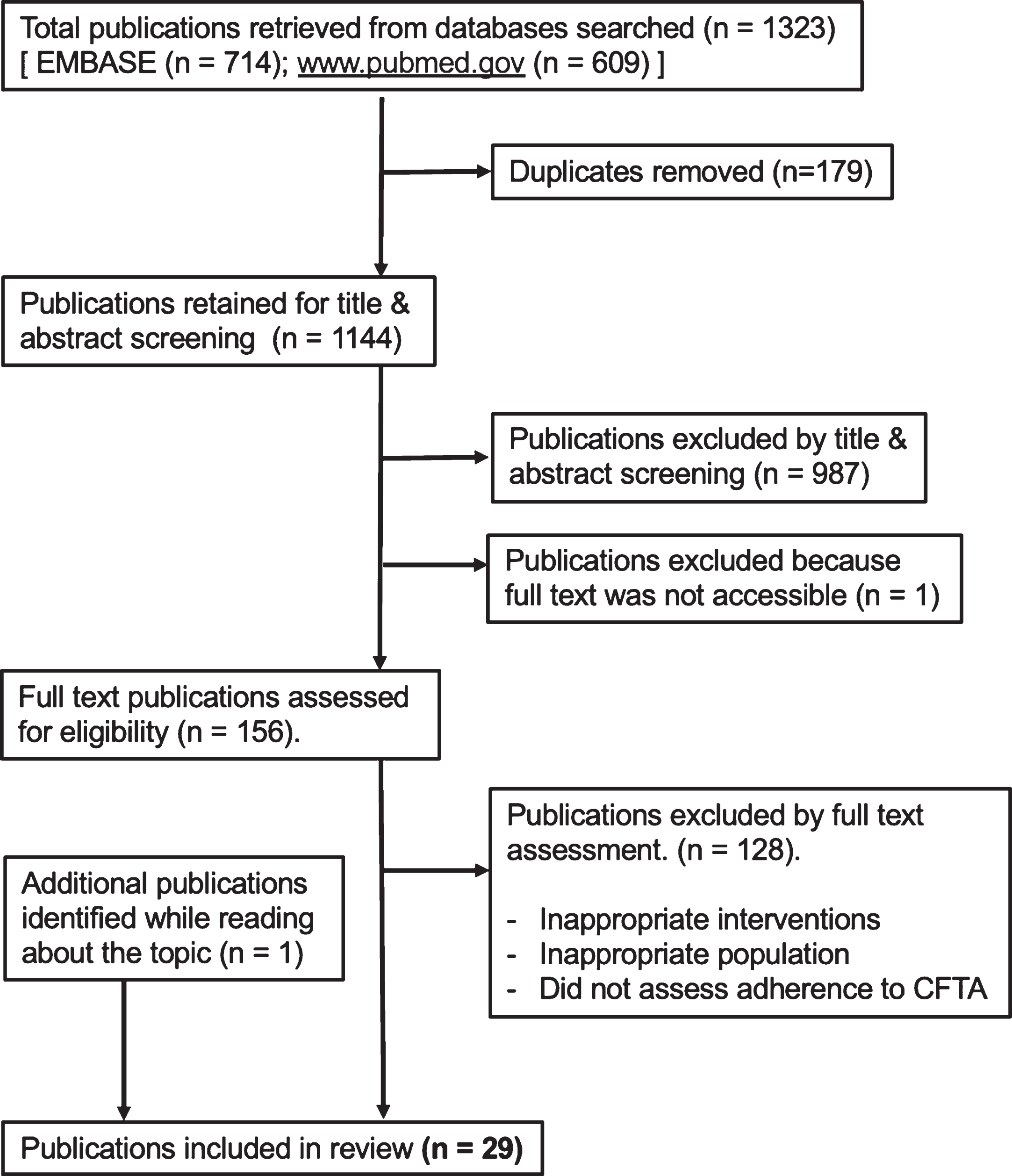
PRISMA Flow chart of the search strategy and study selection.
Papers included in this review fulfilled the following criteria: the study participants (population) must have been unpaid or informal caregivers (parents, family members, friends, guardians, etc) providing care for children (aged from birth to 18 years old) and/or the children receiving care from them. The CFTA (intervention) were prescribed by any of the three professionals stated in the study aim. An exception to this inclusion criterion was the inclusion of studies that investigated adherence to foot abduction braces as part of the treatment for congenital talipes equinovarus. This exception was necessary because the prescription and monitoring of foot abduction braces is done by either orthopaedic surgeons [16] or physiotherapists [17] depending on the region. Furthermore, the interventions considered in this review included passive therapeutic activities performed by the caregiver. There were no exclusions based on disease conditions or the types of medical interventions or surgical interventions associated with the health conditions of the children that participated in the studies selected. The outcomes of interest in this review are the measurement properties of the instruments/methods used to assess adherence to CFTA. Therefore, to be included in this review a study must have clearly described the method (or instrument) used to assess adherence. Studies that did not assess adherence to CFTA were excluded. Regarding the study type, the authors included any type of completed study in which adherence to CFTA for children was assessed. Protocols of studies not yet completed were excluded.
The two authors independently applied the study selection criteria to the studies retrieved from both databases searched and, by consensus, decided on the inclusion or exclusion of the ones on which they did not initially agree. Data was extracted from the full text of each paper selected for inclusion by using a data extraction table adapted from the work of Bollen and colleagues on the psychometric properties of self-reported adherence to unsupervised home-based exercise [3]. See supplementary file for the data extraction table.
The full text of one paper published in 1993 was only accessible via a paywall. It was excluded from this review because it was not available through the authors’ institutional access for published research.
The measurement properties of the identified adherence measures were rated according to the criteria described in Table 1. For studies that did not report validity statistics, it was possible to assess the validity of the adherence instrument based on the criteria and rating system for evaluating the content validity of patient reported outcome measure developed by Consensus Based Standards for the Selection of Health Measurement Instruments (COSMIN) [18]. However, in order to do this the adherence measure must have been either adequately described in the reviewed paper or the details of the adherence measure must have been available in associated supplementary data or the paper made reference to another publication where the adherence measure was adequately described. The criteria for rating the measurement properties described in Table 1 are for descriptive purposes only. Based on these criteria, the maximum rating score for validity was 2. Similarly, the maximum score for reliability was 2. Dyad and interpretability each had a maximum rating score of 1. Therefore, for each adherence measure, the maximum overall score for all four measurement properties combined was 6.
Criteria for rating the measurement properties of methods of assessing adherence to caregiver facilitated therapeutic activity
Criteria for rating the measurement properties of methods of assessing adherence to caregiver facilitated therapeutic activity
r value = Intraclass Correlation Coefficient [34]; Equivalents of r = Cohen’s Kappa, % agreement; *Frost et al (2007) [34]; $COSMIN criteria and rating system for evaluating the content validity of Patient Reported Outcome Measure [18]. Equivalent of r value for reliability = Cronbach’s Alpha.
Considering that adherence to CFTA is not a clinical outcome but an intermediate factor required for a desired clinical outcome [4, 19], the measurement property of interpretability in Table 1 is not based on the responsiveness of adherence measures to detect clinically important change. Furthermore, the concept of “minimum important change” or its equivalents are not considered in the context of this systematic review. Rather, the rating of interpretability of adherence measures in this study relates to the capacity of each adherence measure to detect any change (not necessarily clinically relevant change) in adherence levels within one participant or the differences between participants. This is assessed based on the clarity and relevance of the definition and or the description of interpretability by the creators of the measures of adherence [20]. The rating of interpretability is also based on the relevance of each adherence measure to the population for which it was used. Some adherence measures are inherently interpretable because they have numerical scales, Likert scales or similar reporting tools. Such adherent measures were automatically given a score of 1 for interpretability in this review (see Table 1). Although it is important for researchers of adherence to state the threshold or minimum score that they categorised as adherent in their instrument, this was not considered in the rating of interpretability in this review.
Twenty-nine papers published between 1981 and 2020 were selected for inclusion in this systematic review. They featured diverse methods for assessing CFTA adherence which were grouped into 7 categories shown in Table 2. Some of the papers featured more than one method of assessing adherence to CFTA. A total of 40 adherence measures were identified from the 29 papers reviewed. Details of the data extraction are in the supplementary file.
Measures (instruments) of adherence to caregiver facilitated therapeutic activity
Measures (instruments) of adherence to caregiver facilitated therapeutic activity
Table 3 shows that none of the 40 measures of adherence identified achieved the maximum rating of 6/6 for the four measurement properties considered.
Ratings of the measurement properties of adherence measures based on the criteria in Table 1
PARQ (Parent Adherence Report Questionnaire). GAS (General Adherence Scale).
Only one adherence measure achieved a total rating of 5/6. This was the compliance questionnaire used by Law and King [21]. It fell short of the maximum rating because it lacked dyadic considerations. The next highest rating was the Parent Adherence Report Questionnaire used by De Civita and colleagues [5]. It scored 4/6 and is the only adherence measure that wholly or partially fulfilled all the 4 measurement properties considered (i.e. validity, dyadic consideration, interpretability and reliability). It was rated 1/2 for construct validity because the reported r value was 0.62 when the General Adherence Scale is used as the referent standard scale that measured the same construct. This means that there was a 62% agreement between the two. De Civita and colleagues also reported a Kappa coefficient of 0.36 which they computed by comparing the Parent Adherence Report Questionnaire to adherence rates reported in the daily logs of caregivers in their study. This means that there was 36% agreement between values obtained from the Parent Adherence Report Questionnaire and the caregivers’ reported adherence in their daily logs of CFTA performed. Similarly, the reliability (reproducibility) of the exercise items on the Parent Adherence Report Questionnaire was rated 1/2 in this review because the intraclass correlation coefficient for reproducibility was reported to range from 0.53 to 0.88. This indicates that there was between 53% to 88% agreement between values obtained from repeated assessments for some of the items on the questionnaire. Furthermore, the Kappa coefficient for the reproducibility of items on the Parent Adherence Report Questionnaire assessing the locus of responsibility was 0.42. Therefore, the authors of this review downgraded the rating for reliability to 1/2 because the reliability coefficients of several items were less than 0.7.
Interpretability was the most commonly fulfilled measurement property. A total of 27 of the 40 adherence measures identified received a rating of 1/1 for interpretability. This was attributed to the way interpretability was defined in the rating criteria for the measurement properties (Table 1).
Only two of the 40 adherence measures reviewed reported validity data, six reported reliability and six had dyadic considerations. Twenty of the adherence measures reviewed had total scores of 1/6 while 11 of them had total ratings of 0/6. This indicated either a lack of consideration for any of the four measurement properties reviewed or inadequate reporting of the measurement properties by the authors of those research articles.
The findings of this review are in line with those of Bollen and colleagues [3]. Researchers frequently use measures for assessing adherence with inadequate consideration for the measurement properties of the instruments used. This is perhaps attributable to the aforementioned fact that adherence is not regarded as a clinical outcome but rather an intermediate requirement for the achievement of a desired clinical outcome. Hence, the measurement properties of the instruments used to assess adherence tend to receive less scrutiny from research publication reviewers. However, this review also demonstrates the trend for inaccurate assessment of adherence by researchers and clinicians alike. The literature is replete with myriad and disparate methods of assessing adherence to CFTA which makes the consideration and accurate reporting of their measurement properties crucial to evidence-based practice. For example, Frost and colleagues in 2016 [22] reported that the use of diaries to assess adherence is valid at the group level but not at the individual level. Conversely, Frost and colleagues in 2017 [23] reported that diaries and logs have excellent criterion validity for the specific populations in which they have been validated for but lack reliability. Furthermore, observational scales for assessing adherence can be valid and reliable [24] but the researchers using them should demonstrate the validity and reliability of the specific scales used. The use of some wearable sensors for assessing adherence may be reliable but has inadequate validity [23]. The incoherence and divergence in the outcomes of these studies demonstrate that the validation of one adherence measure does not confer validity or reliability onto another adherence measure in the same category. It is vitally important that researchers should report the measurement properties of the specific instrument used in their work.
It is desirable for adherence measures for paediatric CFTA to have dyadic considerations because they seek to measure changes in the behaviours of both the child and the caregiver, rather than the behaviour of either the caregiver alone or the child alone. Studies that used adherence measures with dyadic considerations have included research participants as young as 9 months old [25]. This is because adherence to CFTA is usually a patient reported outcome (excepting some wearable sensors) and the caregiver is the reporter of child adherence to CFTA [26–28]. Therefore, it follows that dyadic consideration is not limited by the age of the child, verbal ability, or cognitive ability. It is feasible to assess the adherence of the dyad in any CFTA. However, this review shows that adherence measures for paediatric CFTA generally lack dyadic considerations, which may necessitate the combination of two or more complementary adherence measures in the absence of a single measure that considers both the caregiver and the child. This is a viable solution for dyadic considerations in paediatric adherence assessment in clinical and research settings. Furthermore, future research should incorporate a dyadic framework into the development of new adherence measures for CFTA. This is important given an increasing global burden of diseases and the need to facilitate maximum adherence to non-pharmacological and non-surgical therapies. Accurate quantification of adherence to CFTA may add value for money to healthcare services per unit of population by enhancing the economic factors in rehabilitation. This includes recovery time, the number of consultations with rehabilitation specialists before full recovery, injury recurrence, and readmission rates.
Study limitations
This review relied solely on published research articles found on two databases and their published supplementary data, where available. The reviewers did not contact the authors of any of the articles reviewed for more data/information. This may affect the rating of the measurement properties of some of the adherence measures. For example, a cursory look at the one-week diary card used by Downs and associates [29] appeared to be inherently interpretable, but it was not available for the authors of this systematic reviewer to assess. In addition, Downs and associates did not adequately discuss the interpretability of their adherence measure, nor did they provide a reference to published supplementary data on the subject. Hence, the interpretability of the one-week diary card was rated as zero (i.e., not interpretable).
Another limitation of this study is that it did not distinguish the components of adherence assessed by each adherence measure identified. Considering that adherence is defined as behavioural changes in line with prescribed frequency, duration, and quality of performance of therapeutic activity [4, 29], an adherence measure should assess adherence to the three components (frequency, duration, and quality/accuracy of performance) of the prescribed therapeutic activity. It is rare to find adherence measures that assess all three components. A cursory look at the 40 adherence measures identified in the 29 papers reviewed showed that most of them did not. This could be due to the fact that most adherence measures are caregiver reported, and the frequency and duration of performance of CFTA are easily documentable in a diary or questionnaire. On the other hand, the accuracy of performance of CFTA requires observation by an expert performer (clinician) or a mechanism for detecting the accuracy of performance. This is perhaps the reason why most adherence measures are unable to assess all components of adherence. Future studies may explore the ability of measures to assess all components of adherence.
Finally, studies that reported the use of an adherence measure created by modifying an existing validated measure were rated for their measurement properties by the authors of this review based on the rating of the original adherence measure from which the modified measure was created. An example of such is the modified general adherence scale used by De Civita and associates [5] which was rated 2/2 for both validity and reliability because the original scale satisfied the criteria for those ratings. This rating process may not be accurate given that any modifications to a measurement scale requires revalidation of the scale [30–32].
Conclusions
Most adherence measures used for paediatric CFTA are interpretable, but they are generally not valid or reliable. They also do not consider the dyad and, instead, focus mostly on the caregiver. Given that adherence to therapy is a requirement for desired clinical outcomes, the practical implication of this study is that, in the absence of evidence-based adherence monitoring strategies by clinicians and researchers, clinical effectiveness studies would be suboptimal, clinical governance would be incomplete, cost-benefit analysis of preventive and curative strategies in rehabilitation would be inaccurate, and there would remain a missing link in strategies to reduce the global burden of diseases [33]. It is proposed that researchers and clinicians use valid and reliable measures of adherence and that they clearly report the measurement properties of their adherence measures. Furthermore, in the absence of adherence measures for paediatric CFTA that have dyadic considerations, clinicians and researchers may combine two or more complementary adherence measures to ensure that the adherence of both the child and caregiver are assessed.
Footnotes
Acknowledgments
The authors acknowledge Roberto Meroni (PhD) for facilitating access to one of the databases used in this study.
Conflict of interest
The authors have no conflict of interest to report.
Ethical considerations
This paper did not require ethical review board approval because it is a systematic review of the literature.