
Abstract
PURPOSE:
To determine whether adolescents with cerebral palsy (CP) initiate and are up-to-date with the human papillomavirus (HPV) immunization series compared to adolescents in the general population.
METHODS:
Data on initiation and up-to-date status of the HPV series were collected on adolescents with CP aged 13–17 years old (n = 74) via retrospective medical record review and compared to 616 age-matched peers from the National Immunization Survey, Teen 2019. Analysis by gender, Gross Motor Functional Classification System (GMFCS) level, and ambulatory status was performed in the CP group.
RESULTS:
Adolescents with CP were three times less likely to start (p < 0.001) and two times less likely to be up-to-date (p = 0.004) with the HPV immunization series compared to age-matched peers. When the HPV immunization series was initiated in adolescents with CP, these adolescents were as likely to complete the series (p = 0.400), with 83.3% being up-to-date. In those with CP, there was no statistical difference in status of the HPV immunization series when comparing gender, GMFCS level, or ambulatory status.
CONCLUSION:
Adolescents with CP were less likely to start the HPV immunization series; however, they were as likely to be up-to-date with the series if it was initiated. This presents an opportunity for pediatric physiatrists to help reduce the disparity.
Introduction
Human papillomavirus (HPV) is typically a sexually transmitted virus that causes anogenital and oropharyngeal diseases, including cancers of the cervix, vulva, vagina, oropharynx, penis, and anus along with non-genital and genital warts [1]. Transmission occurs mainly via sexual contact, including oral sex, but can also occur via more innocuous routes such as saliva or hand contact [2, 3]. Approximately 63–91% of the aforementioned cancers are associated with HPV, with the most common locations being oropharyngeal and cervical [4]. The HPV vaccine was developed to protect against infection and development of HPV-associated diseases [5]. Since introduction of the vaccine, there has been a 71–86% decrease in prevalence of high-risk HPV types in females, highlighting the importance of vaccination in disease and cancer prevention [4].
In the United States, HPV vaccination in females was recommended starting in 2006 and subsequently for males in 2009. At the time of publication, the Advisory Committee on Immunization Practices (ACIP) recommends routine HPV vaccination for males and females starting at 11 or 12 years of age, younger if sexually abused [6, 7]. If vaccination is initiated prior to 15 years of age, a two-dose series is recommended; if 15 years or older, three doses are required to be effective [5]. In 2019, data from the Centers for Disease Control and Prevention (CDC) show that 71.5% of adolescents aged 13–17 years had started the HPV vaccine series, and 54.2% were considered up-to-date (defined as receiving the appropriate number of doses based on age and immunocompromised status and dosing at valid time intervals) [4, 8].
Individuals with disabilities are often considered an unrecognized health disparity population, particularly when considering preventative healthcare [9]. Cerebral palsy (CP) is a group of disorders that results from abnormalities of the developing brain and causes motor disability. Children with CP have been found to have lower rates of vaccination coverage compared to the general population, with higher risk of incomplete or delayed immunization [10]. While several small studies have demonstrated lower immunization rates for HPV in children with chronic medical conditions, data on HPV vaccination rates among adolescents with CP are limited [11, 12].
Several factors may place individuals with CP at higher risk for sexually transmitted infections, such as HPV. There is a misconception that adolescents with chronic illnesses and physical disability are less sexually active and therefore at lower risk for HPV infection. However, adolescents with CP become sexually active at about the same age as those without a physical or cognitive disability [13]. They also report a similar frequency of sexual activity and contraceptive use as individuals without a disability [13, 14]. Sexually active adolescents with chronic conditions, including CP, report a higher rate of sexually transmitted infections than peers without a chronic condition [13, 14]. These children are also more likely to become victims of sexual abuse and may not know when or how to disclose mistreatment with their providers [15].
Additional factors may place adolescents with CP at higher risk for HPV infection. In young adults with CP, 90% report that sexuality had not been addressed during their rehabilitation treatment, decreasing their awareness of prevention strategies [16]. Parental influence and overprotection may also hinder proper discussion about sexual health for children and adolescents with CP [17]. Finally, individuals with disabilities may receive routine preventive services, such as cervical cancer screening (i.e., pelvic examinations or Pap smears), less often than peers, and those with more severe disability may receive these services even less frequently [9, 18]. These factors combine to put individuals with CP at higher risk for sexually transmitted infections, highlighting the importance of vaccination for disease prevention.
In this study, HPV vaccination rates of adolescents with CP were compared with available data from adolescents in a similar geographical region. It was hypothesized that adolescents with CP would have lower vaccination rates compared to the general population. Similarly, adolescents with more severe gross motor involvement would have even lower rates of HPV vaccination. A tertiary hypothesis of this evaluation was that female adolescents with CP would have higher vaccination rates than males.
Methods
After Institutional Review Board approval, a retrospective chart review was performed. It included data from children and adolescents with a diagnosis of CP who were followed at a single, tertiary care pediatric hospital.
Participants were identified in the electronic medical record using ICD-9 or ICD-10 codes for CP and having a visit with a pediatric rehabilitation medicine (PRM) provider between January 2015 and January 2020. Participants were included if their age ranged between 11 and 22 years and they were a resident of Missouri or Kansas to allow comparison to statewide immunization data. Individuals were excluded if they fell outside of this age range, were not seen in the PRM clinic during the timeframe, had incomplete immunization records, or did not reside in the bistate region. In total, 129 participants with a diagnosis of CP who were between ages 11 and 22 years were identified. A total of six participants were excluded for the following reasons: immunization data incomplete [2], residing outside of bistate area [2], no clinical evaluation in timeframe [1], and incorrect diagnosis [1]. Thus, 123 participants were included in the total sample (Fig. 1).
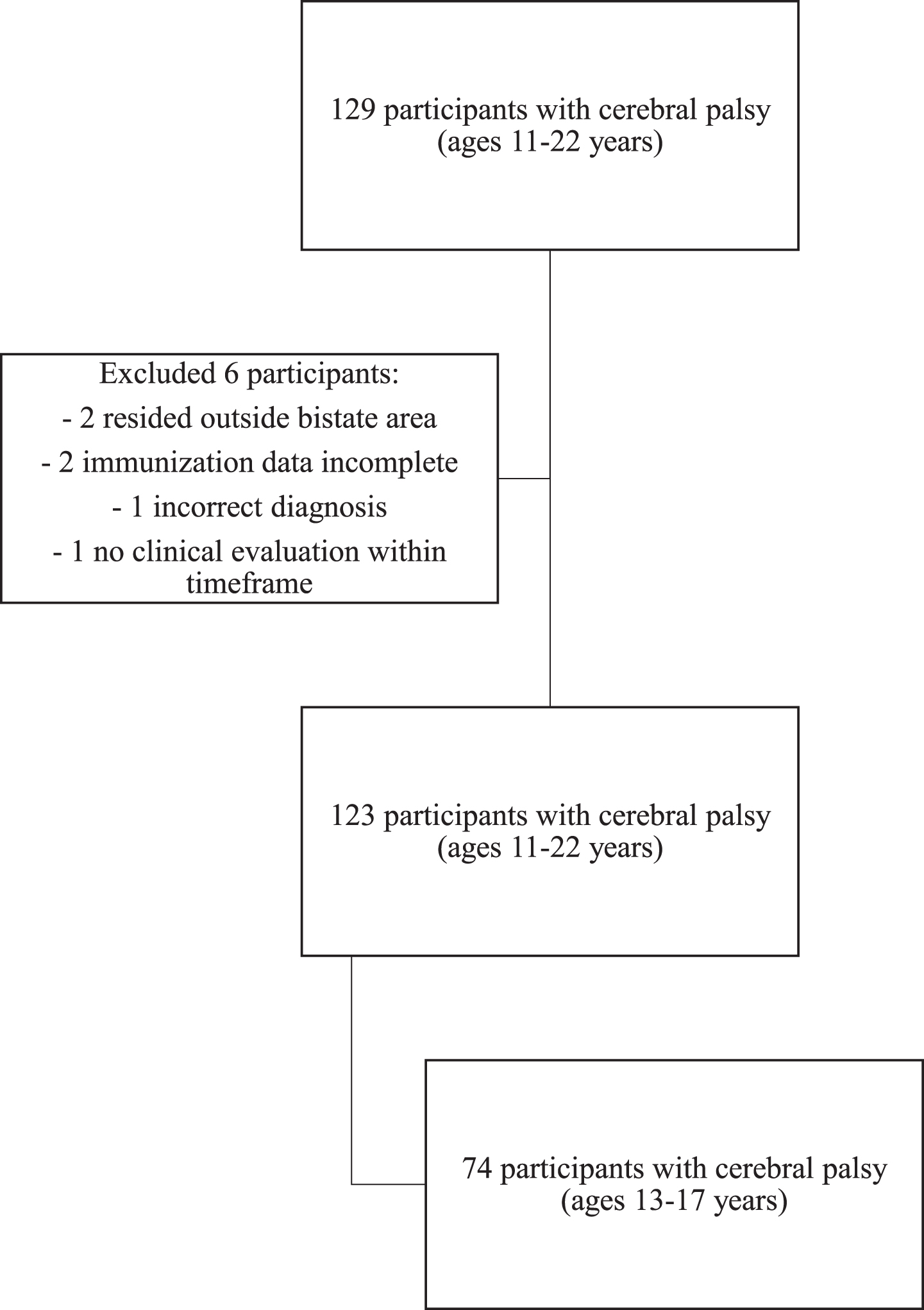
Flow-chart illustrating inclusion and exclusion of study participants.
Demographic information included age and documented gender. The Gross Motor Function Classification System (GMFCS) level was recorded by the provider at the time of clinic visit in the electronic medical record as part of a divisional Quality Improvement (QI) project. For individuals who did not have documentation of GMFCS level during this QI project, GMFCS level was obtained from review of the clinic note. The HPV immunization status of each participant was collected through the electronic medical record, state electronic databases (Missouri and Kansas), and communication with the primary care provider. This included whether the HPV vaccine series was started and dates of vaccine administration. The vaccine series was considered up-to-date for participants based on 2016 ACIP and CDC guidelines for a 2-dose series if under 15 years and 3-dose series if 15 years of age or older [7]. If administered prior to the updated 2016 guidelines, a 3-dose series was considered up-to-date for all ages. Additionally, the time interval between doses had to meet ACIP guidelines (6–12 months from prior dose) for a participant to be considered up-to-date [7]. For the purposes of this study, participants who had completed the series per these recommendations were labeled as “up-to-date” to allow comparison with regional data.
Frequency data were calculated for the entire sample stratified based on age, gender, GMFCS level, and immunization status. First, a Chi-square Test of Association was conducted between gender and immunization status as well as GMFCS level and immunization status. Given perceptions of disability, data were further stratified into ambulatory participants (GMFCS I-III) and non-ambulatory participants (GMFCS IV-V). A Chi-square Test of Association was also conducted between ambulatory status and immunization status. To quantify the relative relationship between vaccination status and each population, odds ratios (OR) were also calculated.
Second, a subgroup analysis was performed to compare the sample population with data from adolescents in the bistate region (Missouri and Kansas). State-level data are available for adolescents aged 13–17 years via the National Immunization Survey (NIS)-Teen [19]. NIS-Teen data are collected annually by phone survey of randomly selected parents and guardians of eligible adolescents. The most recent data available are from 2019. Sample participants within this age range (13–17 years old) were included for this portion of the analysis (n = 74; Fig. 1). A Chi-square Goodness of Fit test was conducted to compare the sample population with the NIS-Teen population data. A significance level of p < 0.05 was used for all analyses. Statistical analyses were carried out with SPSS 26 software (IBM, New York, NY, USA).
Sample characteristics
The sample population included 65 males (52.8%) and 58 females (Table 1). The mean age was 15.22 years (SD 2.80, range 11–22). Participants were classified as GMFCS level I (9.8%), II (24.4%), III (11.4%), IV (26.8%), and V (27.6%). Fifty-six participants were classified as ambulatory (45.5%) and 67 were non-ambulatory based on GMFCS levels I-III and IV-V, respectively. Information on the subgroup of 13–17-year-old participants is provided in Table 1. There was no statistically significant difference in gender of participants between the CP subgroup and the NIS-Teen group (p = 0.424).
Characteristics of study population and available data from NIS-Teen† 2019
for the bistate area of Missouri and Kansas
Characteristics of study population and available data from NIS-Teen† 2019 for the bistate area of Missouri and Kansas
†National Immunization Survey—Teen; ‡Cerebral Palsy.
In total, 53 participants (43.1%) started the HPV series and 37 participants (30.1%) were up-to-date with the HPV series (Table 2). In the subgroup analysis of 13–17-year-old participants, 40.5% (n = 30) started the HPV series and 33.8% (n = 25) were up-to-date. If the HPV series was initiated, 68.9% of the total sample and 83.3% of the 13–17-year-old subgroup were up-to-date. In the total sample, participants who were up-to-date with the HPV series received their first dose at a mean age of 11.9 years (range 9.1–15.7 years).
HPV† vaccination status, all participants
HPV† vaccination status, all participants
†Human Papillomavirus; ‡Cerebral palsy; §National Immunization Survey—Teen; *statistically significant.
Data extracted from the NIS-Teen survey 2019 for Missouri and Kansas revealed 67.2% of teens started the HPV series and 51.6% were up-to-date (Table 2). There was a statistically significant difference in starting the HPV series between the general population and teens with CP (p < 0.001; OR 3.014). There was also a statistically significant difference in being up-to-date with the HPV series when comparing the entire subgroup populations (p = 0.004; OR 2.087). However, if the HPV series was started, participants with CP were as likely to be up-to-date with the series as the general population (p = 0.400; OR 1.522)
In the total sample with CP, there was no statistically significant difference between genders in starting the HPV series (p = 0.464). There was no difference between genders in being up-to-date with the HPV series (p = 0.828; Table 3).
HPV† vaccination status by gender
HPV† vaccination status by gender
†Human Papillomavirus; ‡Cerebral palsy; §National Immunization Survey—Teen; *statistically significant.
Similarly, no gender differences were found in HPV series initiation and being up-to-date for the 13–17-year-old subgroup with CP (p = 0.642 and p = 0.687, respectively). When compared to females in the NIS-Teen group, females with CP were statistically less likely to start the HPV series (p = 0.001; OR 3.396). Females with CP were also statistically less likely to be up-to-date with the HPV series (p = 0.040; OR 2.228). Males with CP were statistically less likely to start the HPV series (p = 0.002; OR 2.761) and were less likely to be up-to-date with the HPV series (p = 0.037; OR 2.009) compared to males in the NIS-Teen group. There were no statistical differences between females and males with or without CP and being up-to-date with the HPV series if the series was started (p = 0.514 and p = 0.609, respectively).
When considering GMFCS level in the total sample, there was no statistically significant difference between levels for starting or being up-to-date with the HPV series (p = 0.377 and p = 0.923, respectively). Likewise, there was no significant difference in the 13–17-year-old subgroup for starting or being up-to-date with the series (p = 0.703 and p = 0.547, respectively; Table 4).
HPV† vaccination status by GMFCS‡ level and ambulatory
status
HPV† vaccination status by GMFCS‡ level and ambulatory status
†Human Papillomavirus; ‡Gross Motor Function Classification System; §Cerebral palsy.
Analysis by ambulatory status (GMFCS I-III compared to GMFCS IV-V) did not demonstrate statistical significance for starting the HPV series in the total sample or the 13–17-year-old subgroup (p = 0.962 and p = 0.918, respectively). Similarly, there were no statistically significant differences between ambulatory and non-ambulatory groups for being up-to-date with the HPV series in the total sample or the 13–17-year-old subgroup (p = 0.649 and p = 0.800, respectively).
This is the first study to specifically address HPV vaccination in children with CP. Compared to NIS-Teen data of randomly selected adolescents, adolescents with CP residing in the same region were significantly less likely to start the HPV vaccination series. Teens in the general population were approximately three times more likely to start the HPV series than teens in the CP sample. These results support prior findings that individuals with CP represent an under-immunized population, highlighting potential health disparities faced by individuals with disabilities [9, 10].
When considering adolescents who started the HPV vaccine series, those with CP were up-to-date 83.3% of the time, which is similar to the general population. This finding underscores the importance of initiating the HPV vaccination series. By initiating the series, providers may be able to make a significant difference in the rates of adolescents with CP who are fully vaccinated. Additionally, those with CP who were up-to-date with the vaccine series initiated the first dose at 11.9 years of age, consistent with ACIP recommendations. Studies have demonstrated that vaccination is less likely in those who delay vaccines, so providers should emphasize initiating the vaccine series per the recommended ACIP guidelines [20, 21]. Pediatric physiatrists have the potential to impact vaccinations rates by counseling individuals and families and recommending HPV vaccination at the appropriate age.
Prior studies have demonstrated that provider recommendation and trust are predictors of HPV vaccination in adolescents in general [20–22]. Many children with chronic medical conditions may visit specialists more than primary care providers and consider a specialist as their primary provider [23]. Specialists report less comfort discussing sexual health and recommending and prescribing HPV vaccinations [23]. Thus, increasing awareness of HPV-related diseases and low HPV vaccination rates and encouraging specialists to offer HPV vaccinations may increase vaccination and decrease disease burden in adolescents with CP.
Gender bias has played a role in HPV vaccination in general, with early focus on vaccination of females and more recently males [24]. In this study population, both males and females with CP appeared to be less likely to have started the HPV vaccination series and were less likely to be up-to-date compared to gender-matched peers. Although this was the case, there were no differences between genders in HPV vaccination initiation or being up-to-date in this population of adolescents with CP. This may indicate a reduced gender bias in this population or differences in local practice patterns.
There is also a prevailing bias that individuals with physical disabilities or chronic conditions are less sexually active, thus less at risk for HPV infection. Sexual activity rates in adolescents with physical disabilities may be similar to the general population and sexual education rates may be lower [13]. These individuals may be at higher risk for sexual abuse, increasing potential exposure to HPV [15]. While the risk of HPV infection may be similar if not greater in this population, physical disability is often seen as a barrier to common screening procedures, such as pelvic examinations and Pap smears [9]. Individuals with disabilities such as CP are less likely to receive these recommended screening procedures and thus may have unrecognized and untreated HPV-associated disease [18]. The results of this study show no differences in HPV vaccination rates between GMFCS levels or based on ambulatory status. This indicates that individuals with a higher degree of gross motor impairment were as likely to receive the HPV vaccination as those with less impairment, which has not been demonstrated consistently in other studies [18]. These findings may be due to reduced bias, local practice patterns, or smaller sample size. Additionally, other factors that were not included here, such as intellectual disability, may play a role in vaccination patterns.
Pediatric physiatrists have the ability to impact HPV vaccination rates and cancer prevention in adolescents with CP. Providers should educate this population on sexual health and the risks of sexually transmitted infections and recommend appropriate screening procedures to all adolescents with CP. If able, specialists should offer vaccinations directly to individuals with CP or provide specific information on where and when the HPV vaccination should be obtained [25]. Common barriers for both providers and caregivers include discomfort with the topic, misinformation and stigma about HPV vaccines, culture, language, and low health literacy. To address these barriers, the CDC and American Cancer Society provide updated information on HPV vaccination recommendations, vaccination program implementation strategies, and educational materials for caregivers and patients [6, 25]. Pediatric physiatrists may utilize these and local resources to promote HPV vaccination and HPV-associated cancer prevention in this population.
Limitations
This study has several limitations. Data are from one tertiary care pediatric hospital. Results may be skewed by geographical attitudes toward vaccination or community practice patterns. To mitigate these limitations, the population data were compared to the NIS-Teen data only from the same states where the included participants resided. It is unknown if any children with CP were included in the NIS-Teen data. The sample size is relatively small, making it difficult to extrapolate to the larger population of adolescents with CP. Similarly, larger numbers of participants of each gender and each GMFCS level may lead to more robust results.
Conclusions
Children and adolescents with CP represent an under-immunized population in the United States. Adolescents with CP are less likely to initiate and be up-to-date with the HPV vaccination series compared to peers. However, they are just as likely to be up-to-date with the series if it is initiated; thus, it is important for healthcare providers to advocate for HPV vaccination in adolescents with CP. In this population, there were no differences between gender or function in starting or being up-to-date with the HPV vaccination series. Further research is warranted to determine strategies to reduce vaccination disparities in the CP population.
Footnotes
Acknowledgments
We are indebted to the tireless advocacy of Cindy Olson Burgess. Her dedication to ensuring all children are immunized is remarkable, and her efforts to collect data to this end laid the foundation for this study.
Funding
Matthew McLaughlin received grant funding through an NICHD grant (1K12HD093427).
Conflict of interest
The authors have no conflicts of interest to report.