
Abstract
PURPOSE:
The purpose of this study was to assess if the incidence of lower extremity (LE) pressure injuries resulting in amputations was more frequent in ambulatory versus non-ambulatory patients with spina bifida.
METHODS:
The medical records of all patients at a large pediatric rehabilitation hospital who had spina bifida and a history of a pressure injury between 1997–2018 were retrospectively reviewed.
RESULTS:
In this study, 112 patients with spina bifida developed LE pressure injuries, 53 patients walked with braces and/or an assistive device, and 59 patients used a wheelchair for mobility. Of the 11 patients who had amputations, 10 walked and 1 did not walk prior to their amputation. Ambulatory patients with LE pressure injuries had a 19% chance (10 out of 53 patients) of requiring an amputation. Non-ambulatory patients with a LE pressure injury had only a 2% chance (1 out of 59 patients) of requiring an amputation. Ambulatory patients with LE pressure injuries were at a much higher risk of requiring an amputation than patients who did not walk (p-value of < 0.005).
CONCLUSION:
Patients with spina bifida who are ambulatory and develop a pressure injury have a high risk of ultimately needing an amputation and should be monitored and treated aggressively.
Introduction
Spina bifida is the second most common childhood disability, although the overall incidence has decreased following mandatory folic acid dietary fortification instituted in 1998 [1]. Spina bifida is a congenital defect in which an incomplete closure of the embryonic neural tube can lead to unfused or underdeveloped vertebrae, paraplegia, sensory deficits, hydrocephalus, cognitive developmental problems, and neurogenic bowel and bladder. Sensory and motor impairments vary greatly and depend on the level of dysraphic malformation [4, 5] Higher level spinal cord involvement can cause more profound brain anomalies with associated neurocognitive impairment [2]. Sensory impairments in the lower extremities (LEs) can lead to pressure injuries, infections, osteomyelitis, and ultimately amputations [2]. Most patients with spina bifida have hypotonic motor deficits due to lower motor neuronal abnormalities. However, 10 to 40 percent of spina bifida patients have a combination of flaccid and spastic paraparesis [3].
The impaired sense of pain and touch in patients with spina bifida puts them at a high risk of acquiring pressure injuries from pressure, trauma, and heat [3]. Pressure injuries often become infected, heal slowly, and can result in acute or chronic osteomyelitis [3]. These bone and deep tissue infections can be very difficult to manage and may ultimately require an amputation. Graham et al. reported that the most common cause of amputations in patients with spina bifida is chronic skin injury [6]. Bowel or bladder incontinence can exacerbate infections [7]. Higher level of spina bifida and brace usage can also impact risk of pressure injuries [8, 9]. Additionally, cognitive impairments can adversely impact a patient’s ability to take care of their injuries appropriately, thus increasing the risk of infection and chronicity [10].
Previous studies have discussed risk factors for amputations, yet none so far have discussed ambulation of patients with spina bifida as a risk factor for amputation. One previous study concluded that a deterioration in ambulation was related to motivation, obesity, and musculoskeletal deformity [11]. Other studies emphasize that mobility impacts a person’s quality of life and highlight that LE amputations are preventable with pressure injury precaution and awareness programs [12, 13]. In the case of people with spina bifida, amputations are often preventable with proper skin monitoring and care.
To the authors’ knowledge, there have been no studies specifically looking at the association of the ambulatory status of patients with spina bifida and their incidence of amputations. Conklin et al. demonstrated that there is no difference between pressure injury risk among ambulatory and non-ambulatory patients with spina bifida but did not look at the risk of developing chronic osteomyelitis and the incidence of amputation [14]. Additionally, Roach et al. suggested that cognitive impairment of patients with spina bifida increases the risk of amputations but did not analyze any associations with ambulatory status [15]. The aim of this study was to assess the risk of amputations in patients with spina bifida who have a LE pressure injury and whether there is an association with ambulatory status.
Methods
This is a retrospective study at a large pediatric rehabilitation hospital. After Institutional Review Board approval, medical records of all patients from 1997–2018 with spina bifida and a history of a LE pressure injury were reviewed. Each patient’s age, level of spina bifida, type of amputation, history of pressure injuries, ventriculoperitoneal shunts status, and ambulatory status were collected. Due to the limitations of a retrospective study, clear, comprehensive evidence of patient cognitive status, socioeconomic status, educational status, vocational status, cultural impact on outcomes, brace usage time, timing/compliance of pressure injury treatments, nor home support could be established. It would be beneficial to explore these topics in future studies.
The patients were categorized into four groups: ambulatory with amputations, non-ambulatory with amputations, ambulatory without amputations, and non-ambulatory without amputations. Ambulatory was defined as a person that ambulated routinely during the day with braces and/or assistive devices. All patients who were ambulatory, by definition, walked short community distances as their main mode of mobility. Many patients were able to walk short household distances but rarely did so and primarily used wheelchairs for their mobility. These patients were classified as non-ambulatory. The Pearson’s chi-squared test was used to determine the correlation between the ambulatory status of a patient with spina bifida and their probability of acquiring an amputation. A systematic review of all materials related to this study topic was performed.
Results
One hundred twelve patients with spina bifida (57 female, 55 male) had a history of LE pressure injuries and, of these patients, 11 ultimately had a LE amputation. All 11 amputations were secondary to chronic pressure injuries of insensate skin below the knees and associated osteomyelitis. No patients with spina bifida and an amputation who did not have a history of pressure injuries were found. The amputation levels varied from transtibial to toe amputations. Three patients had bilateral amputations. The patients had their first amputations between the ages of 4 and 36 years. Eighty-one percent of the patients requiring amputations received their amputation prior to 2000 (9 out of 11). The amputations occurred between 1963 and 2009 (Fig 1). In this study, 53 patients walked with braces and/or an assistive device as their principal mode of mobility, and 59 patients primarily used a wheelchair for mobility. All patients that had ankle-foot orthoses (AFOs), including those classified as ambulatory patients, had custom-molded solid-ankle plastic AFOs. Of the 11 patients who had amputations, 10 were ambulatory and 1 was non-ambulatory prior to their amputation. The patient who did not walk prior to their amputation had a 5th toe amputation (Table 1). One patient who originally had a Syme amputation later developed another pressure injury and subsequently required a transtibial amputation. Of the 10 ambulatory patients, 1 required a toe amputation, 3 required foot amputations, 5 required unilateral below-the-knee amputations, and 1 required bilateral below-the-knee amputations (Table 2).
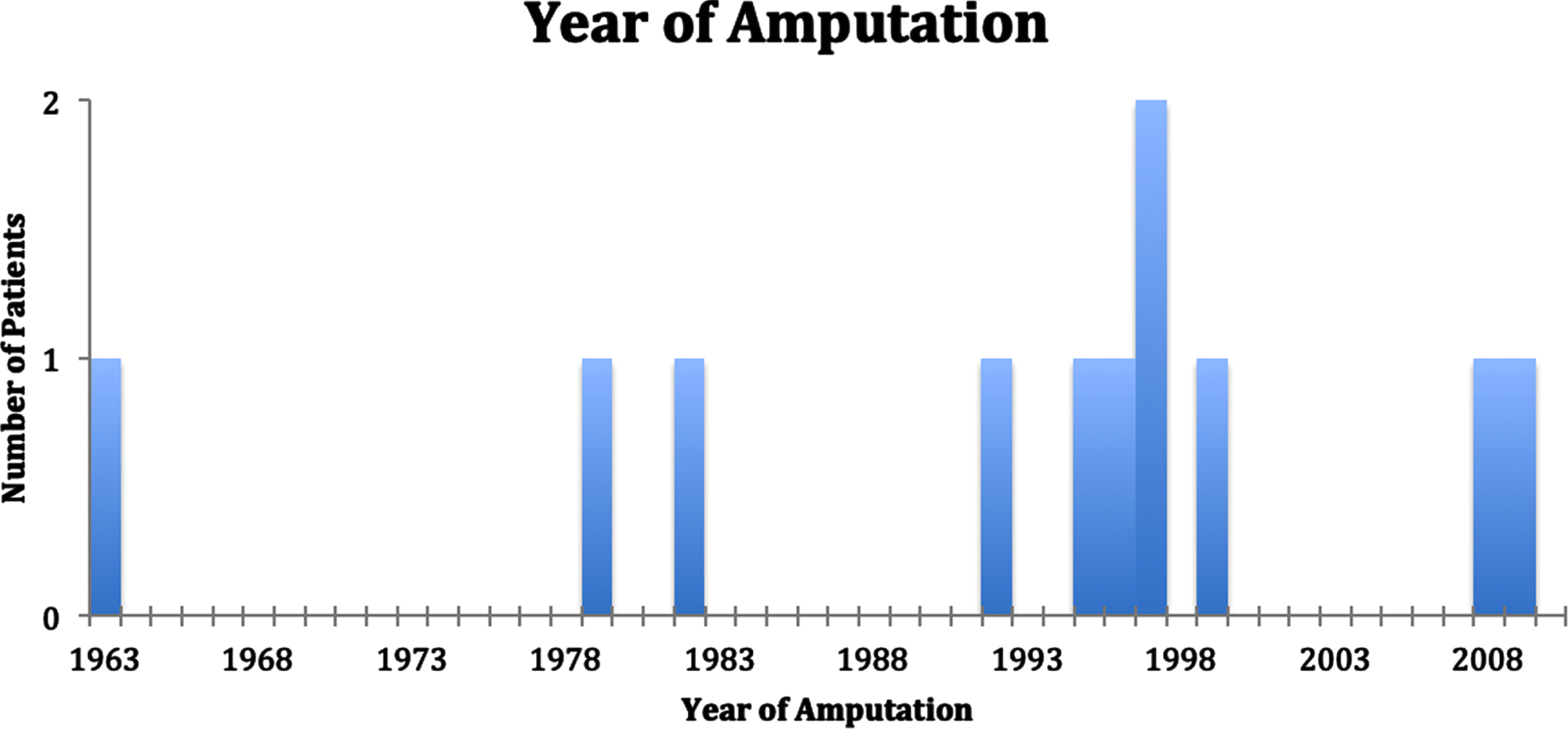
Year amputation was required for each patient.
Patients with spina bifida and pressure injuries. The distribution of patients with or without amputations and ambulatory or non-ambulatory. (Chi-square: 9.5201, p-value: < 0.005)
Type of amputation required for ambulatory and non-ambulatory patients
Out of the 11 patients with amputations included in this study, none had thoracic level of malformation, 63% (7/11 patients) had lumbar level of malformation, and 36% (4/11 patients) had sacral level of malformation (Table 3). Although data was missing from the patients without amputations, of the data available, 23% (16/70 patients) had thoracic level of malformation, 73% (51/70) had lumbar level of malformation, and 4% (3/70) had sacral level of malformation (Table 4). This association was statistically significant and is one of the confounding variables correlated to amputation risk.
Level of spina bifida in patients with amputations
Level of spina bifida, shunt status, and ambulation status compared for those with amputations and those without. P-values show significant confounding factors in all 3 categories. (Of note, missing definitive shunt data from 30 people without amputation history and missing shunt data from 2 people with amputation history. Missing level of spina bifida information from 31 people without amputations.)
Data regarding patient shunt status was also very limited. Of the data available, 22% (2/9) of those requiring amputations had a shunt. Of those not requiring amputations, 90% (64/71) required a shunt (Table 4). Fifty-seven percent (4/7) of patients without shunts and without amputations were ambulators, whereas 86% (6/7) of patients who had no shunt and an amputation were ambulators (Table 5). All patients with a shunt who had amputations were ambulators (2/2) (Table 5). The correlation between not having a shunt and requiring an amputation was significantly correlated with the limited data available (Table 4).
Shunt status in patients that were ambulatory vs. non-ambulatory and in patients that had amputations vs. did not require amputations. Shunt data lacking for 2 patients with amputations
Ambulatory patients with LE pressure injuries had a 19% chance (10/53 patients) of requiring an amputation. Non-ambulatory patients with a pressure injury had a 2% chance (1/59 patients) of requiring an amputation. Ambulatory patients with pressure injuries were at a significantly higher risk of having an amputation than patients who did not walk (p-value of < 0.005).
Patients with spina bifida rarely have amputations. However, they do have an increased risk for pressure injuries due to sensory deficits. These pressure injuries can become infected and progress to chronic osteomyelitis eventually requiring an amputation [12]. Also, cognitive impairment is a risk factor for pressure injury development [13].
In this study, it was found that patients with spina bifida who are ambulatory had a greater chance of requiring an amputation. This increased risk may be due to the inability of these ambulatory patients to feel their limbs, which puts them at risk to develop chronic pressure injuries. When patients can move, there is an increased risk of skin friction, which can cause a pressure injury to develop. Continuing to walk can worsen these pressure injuries rapidly and aggressively. When patients do not adequately care for their pressure injuries or do not allow them to heal properly, the pressure injuries may become chronically infected leading to osteomyelitis and leaving amputation as the only viable treatment option. When walking is their primary mode of mobility, these patients continually traumatize the affected area and tolerate this trauma due to lack of sensation, thus worsening the pressure injury. Even if an ambulatory person with spina bifida is able to heal their pressure injury effectively, there is a high risk that a pressure injury will develop again [14]. With this increased risk of chronic pressure injuries comes the risk of osteomyelitis and ultimately amputation. Of note, radiographs and bony exposure were utilized for evaluating osteomyelitis. The results are consistent with these factors and show that there is a correlation between the ambulatory status of persons with spina bifida and amputation risk.
Ten patients in this study were ambulatory before requiring their amputation, and 9 of them continued to ambulate after their amputations. All these patients had been ambulatory for many years prior to their pressure sore or amputation, and all were good ambulators with their prostheses after their amputation. This may be because they were previously adept at walking on insensate limbs. The one patient that was non-ambulatory after their amputation had bilateral transtibial amputations.
All the patients that were ambulatory had low lumbar or sacral level spinal dysplasia, and those that were not ambulatory either used a wheelchair or did not have adequate strength to ambulate. Seven of those with amputations included in this study had lumbar level malformations and 4 had sacral level malformations, whereas no patients with amputations in this study had thoracic level malformations. Sensory loss is correlated with level of spinal dysplasia, but these sensory deficiencies can often be asymmetric [16]. In this retrospective study, the specific levels of sensation and laterality of sensation were not well-documented in all patients with amputations. Of note, all pressure sores occurred within insensate areas.
One of the confounding factors that must be considered is that all the patients that had amputations had low lumbar or sacral level of myelodysplasia, whereas patients that were mid-lumbar or higher level of myelodysplasia had a lower risk of amputation. However, the pathophysiology of pressure injuries and the need for amputation should not differ significantly between a mid-lumbar and higher myelodysplasia versus a low lumbar and lower myelodysplasia. Chronically traumatizing a pressure sore is more likely to lead to osteomyelitis, a poorly-healing sore, and a need for amputation. Ottolini et al. further supported that foot and ankle injuries most commonly occurred in patients that were community ambulators with diminished sensation, primarily low-lumbar functional levels [17].
Many factors influence the development of pressure injuries. Impaired cognition increases the risk for pressure injuries and persons with spina bifida can have problems with executive functioning, increasing their risk of developing a pressure injury and not properly treating them when they do occur. This study did not explore the impact of cognition that may place a patient at risk for an amputation, mainly because details of that information were not available. Although there are often no obvious differences in cognition between those with hydrocephalus and those without, those with spina bifida without hydrocephalus often have neuropsychological function equal to the general population [15]. Shunt failure and frequency comprehensive data was not available.
With the limited data available, there were multiple factors in addition to ambulatory status that appeared to be significantly correlated with amputation risk, including not having a shunt and lower level of spina bifida (Table 4). Fifty-seven percent (4/7) of patients without shunts and without amputations were ambulators, whereas 86% (6/7) of patients who had no shunt and an amputation were ambulators (Table 5). All patients with a shunt who had amputations were ambulators (2/2). Of note, information regarding shunt status and level of spina bifida for each patient was lacking due to incomplete medical records on multiple patients, but it can be assumed that the remaining data would closely reflect the data available. As such, not having a shunt and having a lower level of spina bifida was correlated to the amputation risk in someone with spina bifida and a history of pressure sores. Hydrocephalus has been associated with lower cognitive status [15]. Those with lower cognitive status are likely less independent compared to those with higher cognitive status. It could be that those without shunts have more independence, are more likely to ambulate, and may be more likely to neglect their pressures sores resulting in need for amputation.
Additional confounding variables potentially impacting risk of amputation were also considered. For instance, the year in which the amputation occurred was analyzed. Only 2 amputations were found in the last 20 years, suggesting that monitoring and treatment of pressure injuries may have improved, decreasing the risk of amputations in ambulatory patients. The average age of those who underwent their first amputation and were ambulatory was 21 years old, and the patient who was non-ambulatory and underwent an amputation was 24 years old. The supportive care that each patient received varied. Generally, in the population with amputations, home support was less, but the data was not sufficient to comment on correlation. Additionally, there was not sufficient evidence in regard to impact of cultural status on amputation risk, and the vast majority of patients included in this study were white. There were no obvious cultural differences between each of the four categorized groups. Generally, treatment compliance and timing for pressure injuries of those that were ambulatory versus non-ambulatory did not differ. Treatment compliance generally did not differ for those that needed amputation versus those that did not need amputation. However, clear, comprehensive evidence was unavailable for this issue or for bracing. The vast majority of patients that had pressure sores, and all ambulatory patients, used custom-molded solid-ankle plastic AFOs. Overall, this study illustrated a stark difference in risk of amputation between ambulatory and non-ambulatory patients. Although other variables may impact amputation risk, this study demonstrated that ambulatory status is a variable that cannot be ignored. Further research in these areas could improve the understanding of the relationship between ambulatory status and the risk for amputations.
Conclusion
This study shows that ambulatory patients with spina bifida who develop LE pressure injuries have a significantly higher risk of amputations compared to those patients who are non-ambulatory. Other factors including not having a shunt and having lower level of spina bifida are correlated with higher risk of amputations in those with spina bifida and history of pressure injuries. Ambulatory patients with spina bifida and lower extremity pressure injuries should be monitored and treated aggressively.
Footnotes
Acknowledgments
Gillette Children’s Research Team
Conflict of interest
The authors have no conflict of interest to report.
Ethical considerations
IRB approval number: 0812M55802
Date of research: 1/24/2021
Funding
No additional funding obtained for this study.