
Abstract
PURPOSE:
The purpose of this study was to measure the growth of the Cerebral Palsy (CP) Research Network towards becoming a Learning Health Network in order to guide future development.
METHODS:
Thirteen CP Research Network leaders completed the Network Maturity Grid (NMG) which consists of six domains with eight to 10 components each. The six domains are Systems of Leadership, Governance and Management, Quality Improvement, Engagement and Community, Data and Analytics, and Research. Radar mapping was utilized to display mean scores on a 5-point ordinal scale (1
RESULTS:
Domain scores ranged from 2.4 in Quality Improvement to 3.2 in System of Leadership. The lowest scoring component was clinician clinical decision support and the highest was common purpose. The following priority areas of focus were agreed upon moving forward: development of leaders, financial sustainability, quality improvement education and training, patient reported data, data quality and validation, and primary data collection.
CONCLUSION:
Results from this project will be utilized for strategic planning to improve the network. Conducting regular self-assessments of the network with the NMG will be useful in achieving the network’s ultimate goal to improve care and outcomes for individuals with CP.
Abbreviations
Introduction
Cerebral palsy (CP) is the most common cause of physical disability in children, with a recent estimated prevalence of 3.5 per 1000 births in the US [1]. CP is associated with a high lifetime cost of care of approximately 11.5 billion dollars for all individuals born with CP in 2000 [2]. Members at a 2014 workshop sponsored by the National Institutes of Health identified a need for a clinical registry for CP in the United States (US) [3]. Different than population-based registries for CP [4, 5, 6, 7], clinical registries are not designed to surveil or estimate the prevalence or incidence of CP but to utilize data from ongoing care to improve healthcare processes and outcomes, describe patterns of care, reduce practice variation, and conduct research. While there have been clinical registries reported at single medical centers in the US [8, 9, 10], the Cerebral Palsy Research Network (CP Research Network) was established in 2015 across multiple institutions as a means to identify problems, generate solutions and answer questions that cannot be solved at a single institution due to the clinical variability in the population and the longitudinal course of CP. The mission of the CP Research Network is to improve outcomes that people with CP value most through high quality clinical research and quality initiatives. A core goal of the CP Research Network is to establish a large clinical registry by aggregating the individuals seen at these institutions.
Clinical registries utilize electronic health record (EHR) data that is collected as part of usual care. EHR data is a driving force behind the emergence of learning health systems [11]. The learning health system, proposed in 2007 by the National Academy of Medicine [12], is defined as any type of healthcare delivery system designed to promote improvement in health and healthcare delivery by integrating care activities of patients, families, clinician researchers, and healthcare system leaders. Learning health systems that include multiple institutions engaging all stakeholders to improve the health of individuals with a specific condition are called Learning Health Networks (LHNs) [13]. There are several pediatric LHNs reported in the literature for diseases such as Inflammatory Bowel Disease [14], pediatric cardiac conditions [15], and pediatric rheumatology care [16] that have demonstrated improved care and outcomes for these conditions [17]. Features of an LHN include multidisciplinary teams and patient/family partnerships that focus on a high impact condition, use data from ongoing care to provide feedback for learning and improvement, test changes iteratively, support an infrastructure for data collection analysis and reporting, and participate in quality improvement (QI). Clinical registries are a key part of LHNs [12] and are utilized to facilitate clinical care, improvement, and research activities [13].
Creating an LHN is a process that can take several years. Construction of a maturity grid is recommended to assess growth and development towards becoming an LHN. The purpose of this paper is to report on CP Research Network’s progress toward developing as an LHN and prioritize areas for growth. The findings will provide detailed information about the strengths, weaknesses, and overall infrastructure of the CP Research Network, as well as opportunities for improvement.
Methods
This descriptive study uses cross-sectional information. In September 2020, CP Research Network leaders (
Network maturity grid domains and their components
Network maturity grid domains and their components
Individual domain scores are computed as the mean of corresponding component scores.
The NMG was developed in 2014 and builds upon literature as well as expert opinion and user experience to provide a structured method to assess network progress and support detailed and strategic discussion [18]. The NMG has a detailed rubric and broad consideration of elements in an LHS. The rubric consists of six domains with eight to 10 components each. The six domains are Systems of Leadership, Governance and Management, Quality Improvement, Engagement and Community Building, Data and Analytics, and Research. See Table 1 for a list of components for each domain. Participants were instructed to rate the maturity for each component within each domain on a 5-point ordinal scale: 1
Average rating for each domain. This figure displays the average rating from 1 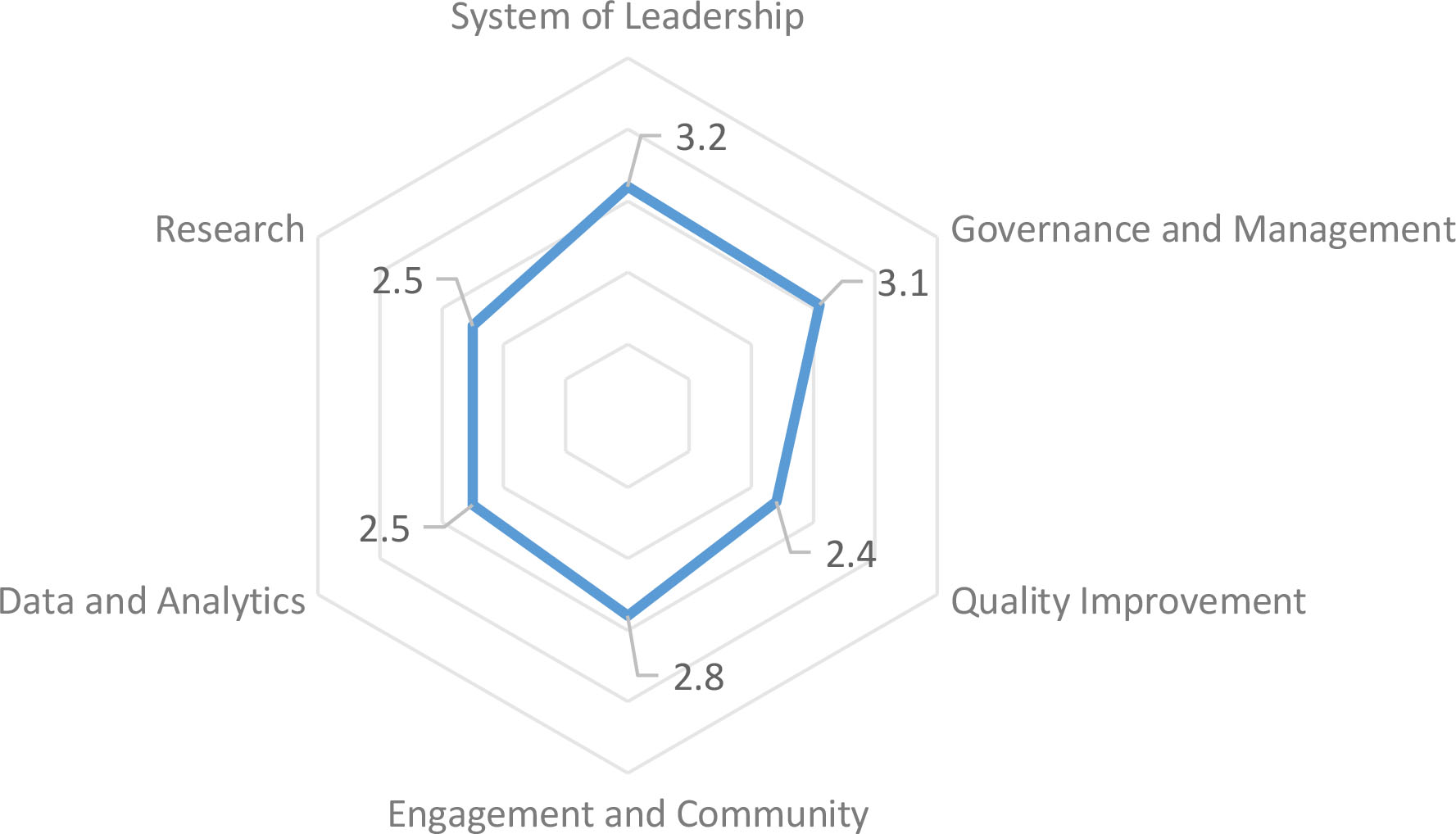
Domain scores were computed as the mean of corresponding component scores. Data visualization included the use of radar mapping [19, 20]. A radar map is a visual display of multivariate data in the form of a two-dimensional chart. Three or more quantitative variables are represented on axes starting from the same point. Radar maps allow for a quick way to visualize data points in relationship to each other. The distance of the variable score from the axis represents performance (scores range from a 1
Component and domain scores were summarized by the PI and shared with network executive committee members. To prioritize areas for growth, each member of the executive committee was asked to identify the top priority component for each of the six domains. Consensus was defined as 70% agreement; components that were ranked a top priority by more than 70% of participating executive committee members were selected. When consensus was not reached by the ranking, the group reached agreement by discussion at a virtual meeting that took place on November 30, 2020.
Results
Thirteen CP Research Network pediatric leaders (68%) responded, which included two advocates, three physical therapists, one health services researcher, two neurologists, two neurosurgeons, one physiatrist, one orthopedist, and one developmental pediatrician. Overall mean scores across domains are displayed as a radar chart in Fig. 1 and ranged from the lowest score of 2.4 in the Quality Improvement domain to a highest score of 3.2 in the System of Leadership domain.
Individual component scores within each domain are displayed as radar charts in Fig. 2 and from highest score to lowest in Table 2. Nineteen components scored 3 or above, while 31 components scored below 3. No components scored the highest score of 5 or idealized state. The highest scoring component was common purpose of the network, with an average of 4.5/5 and the lowest scoring component was clinical decision support with an average score of 1/5.
Average scores for each component of the 6 separate domains of the maturity assessment tool.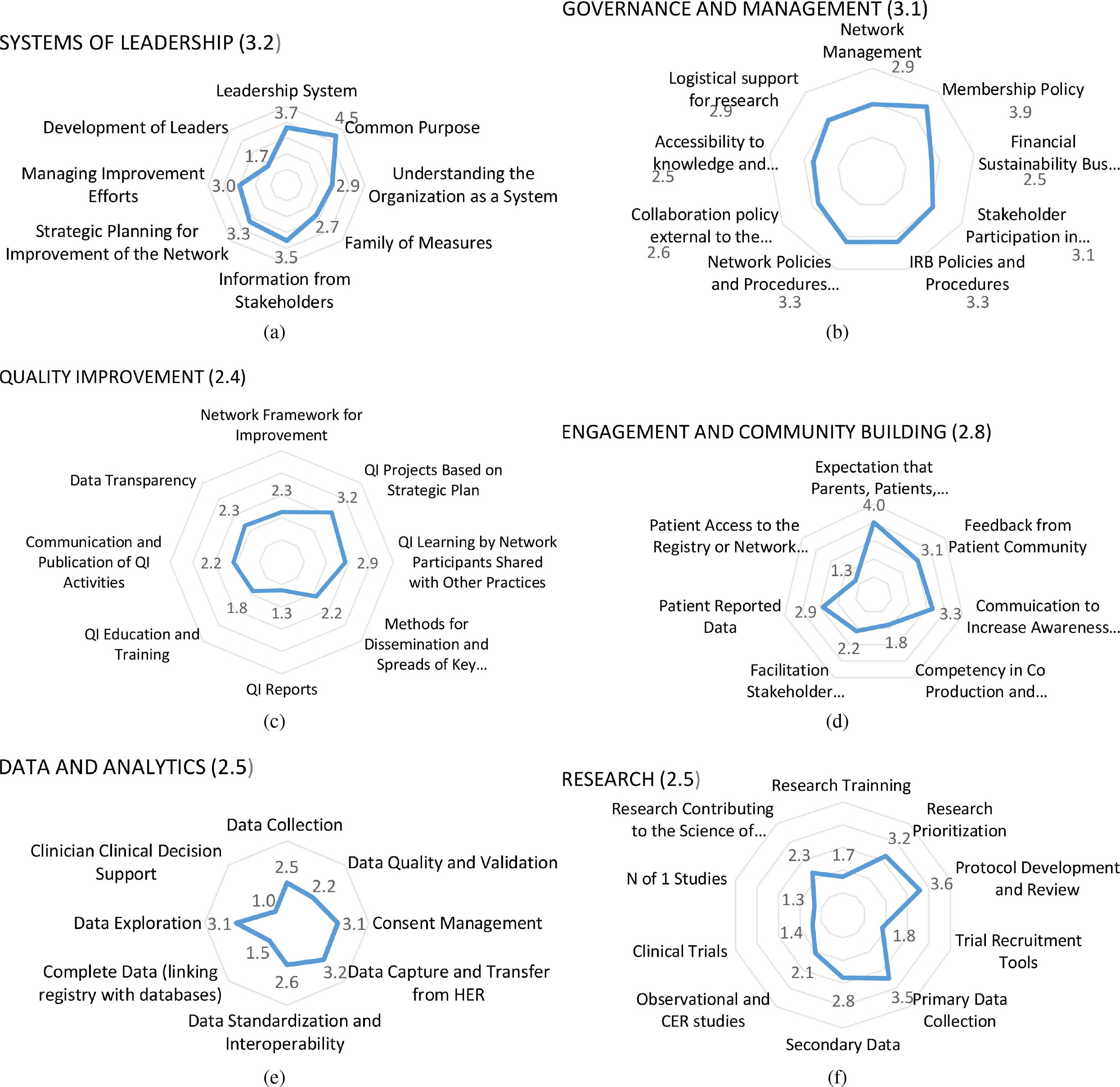
Highest to lowest individual component scores
The CP Research Network Systems of Leadership reflects the network’s commitment to stakeholder involvement and multidisciplinary care and includes an executive committee consisting of two caregivers of children with CP, four physicians, two therapists, and two health services researchers. Several additional committees drive the activities of the network, including the community advisory, investigator, manuscript review, QI and scientific review committees.
The mean Systems of Leadership domain score was 3.2 (SD 0.5). Component scores ranged from a “not started” score of 1.7 (SD 0.6) for development of leaders to a “mature” score of 4.5 (SD 0.5) for common purpose. The components of understanding the organization as a system, family of measures, and development of leaders were rated below a score of 3 as areas for improvement. Intermediate status (score of 3 or above) was achieved for the components of leadership system, information from stakeholders, strategic planning for improvement of the network, and managing improvement efforts. Mature status was achieved only for the component of common purpose.
Governance and management
The CP Research Network activities around Governance and Management include establishing standard operating procedures (SOPs) to govern the network’s development, organizational structure and membership, research, authorship processes, and data sharing. Additional SOPs have been approved for formalizing mentorship, modifying the clinical registry, and developing a community registry. The clinical registry protocol has been developed, shared with network participants, and approved at 28 sites. A master reliance agreement with Nationwide Children’s Hospital’s Institutional Review Board governs six of these sites and the remainder have individual institutional approval for research. Data sharing agreements have been signed with each institution and the Data Coordinating Center is at the University of Utah.
The mean Government and Management domain score was 3.1 (SD 0.8). Component scores ranged from 2.5 for both accessibility to knowledge and tools and financial sustainability to 3.9 for membership policy. The components of network management, logistical support for research, collaboration policy external to the network, financial sustainability, and accessibility to knowledge and tools scored below 3 and were areas for improvement while membership policy, IRB policies and procedures, network policies and procedures, and stakeholder participation in governance scored 3 (“intermediate”) or above.
Founded with a 10-year philanthropic gift in 2015, the network has not finalized its long-term financial sustainability. The initial financial support has been used to establish the data coordinating center (DCC) that consists of one full-time equivalent and several part-time employees and contractors to support the development and maintenance of its registry and its initial forays into research and QI. The individual hospitals provide EHR support as part of clinical operations of the CP programs. The CP Research Network does not directly support the salary of any of the network investigators, though three investigators thus far have received outside funding to support research activities using the CP Research Network.
Quality improvement
QI is an essential part of the CP Research Network. The mean Quality Improvement domain score was 2.4 (SD 0.6). Component scores ranged from 1.3 (SD 0.5) for QI reports to 3.2 (SD 1.0) for QI projects based on strategic plan. Only one component, QI project based on strategic plan, scored a 3 or above. The remaining components of the Quality Improvement domain scored below 3 and were areas for improvement; they include QI learning by network participants shared with other practices, network framework for improvement, data transparency, communication and publication of QI activities, methods for dissemination and spreads of key learnings across care centers, QI education and training, and QI reports.
In 2017, the CP Research Network initiated its first improvement project involving four centers that have reduced the intrathecal baclofen pump infection rate from 4.3 to 2.6 percent per all intrathecal baclofen pump procedures [21]. Strategies learned from this project are currently spreading to other network centers. Four CP Research Network leaders have formal training in QI methodology with another leader scheduled to begin formal training winter 2021. Also a part time QI coach was engaged in 2020, enabling the network to begin work in three additional areas: 1) screening for dystonia, 2) hip surveillance, and 3) adult outcomes across the network. These topics were chosen based on the strategic plan and feedback from the community.
Engagement and community building
At the core of the CP Research Network’s mission, vision, and infrastructure is community engagement and community building. The mean Engagement and Community Building domain score was 2.8 (SD 0.9). Component scores ranged from a “not started” score of 1.3 (SD 0.9) for patient access to the registry or network database to a “mature” score of 4 (SD 0.8) for expectation that parents, patients, clinicians and researchers are co-creators. The components of patient reported data, facilitation stakeholder collaboration, competency in co-production, leadership and patient access to the registry scored below 3 and were areas for improvement. In addition to expectation that parents, patients, clinicians and researchers are co-creators, two other components of this domain scored a 3 or above: communication to increase awareness and feedback from patient community.
The CP Research Network has initiated three large efforts to increase the awareness of the network and obtain feedback from the community. First, in 2017, Research CP was funded in part through an engagement award from the Patient-Centered Outcomes Research Institute (PCORI) to set a patient-centered research agenda for the network. Conducted in partnership with a leading patient advocacy organization (CP NOW), Research CP engaged a broad swath of the extended community – people with CP, parents and caregivers, advocates, clinicians and researchers – in a three-month long process to establish community driven priorities for research. These priorities are being used to drive the development of research and quality initiatives for the network [22]. Also in 2017, a Community Advisory Committee (CAC) was established. A subcommittee including MS, MG and PG advertised in CP related forums and invited known advocates from across the nation to apply if interested in serving. Participants representing diverse geographic regions of the US, ethnic backgrounds and functional levels were selected based on a submitted biography and interview. The CAC includes 10 adults with CP, three adults that care for adults with CP, and 11 parents that care for children with CP. The CAC reviews network strategy and co-produces research and quality efforts on a volunteer basis. Third, more recently in 2019, the MyCP Community Forum and Registry (
Data and analytics
A large effort of the CP Research Network to date has been to define common data elements (CDEs) for each discipline interacting with the person with CP, building these elements into EHRs, deploying forms into clinical care, and transferring data to the DCC. Reflecting these activities, the mean Data and Analytics domain score was 2.5 (SD 0.7). Component scores ranged from 1 (SD 0) for clinician clinical decision support tools to 3.2 (SD 0.6) for data capture and transfer from EHR. The components of data collection, data quality and validation, data standardization, complete data linking registry with databases, and clinician clinical decision support scored below 3 (intermediate) and are areas for improvement. Intermediate status was achieved for components data capture and transfer from electronic record and data exploration and consent management.
To date, CDEs have been defined and are available at
Chart abstraction processes and training for REDCap have also been developed to facilitate consistent data collection practices. The data transfer process is documented on the CP Research Network website including supplementary resources, program scripts and database queries so that sites can be self-sufficient in installing and deploying the registry. A similar set of EHR forms is being developed for Cerner and is anticipated for deployment in 2021. In addition to these resources, a registry explorer function is in development so that investigators can determine the quantity and quality of data for any given field in the clinical registry database.
Research
The CP Research Network activities around the domain of research have included prioritization and creation of a research agenda [22], utilization of pilot data from the clinical registry to support funding applications, and execution of internally and externally funded studies. The mean Research domain score was 2.5 (SD 0.4). Component scores ranged from 1.3 (SD 0.5) for
Internally funded studies that have been completed include function and pain in adults [26, 27] and practice variation for spasticity [28]. Also underway and internally funded is the development of a research agenda specifically devoted to management of dystonia. Externally funded studies that are in progress include Genomic Insights into the Neurobiology of CP (PI Kruer, National Institute of Neurological Disorders and Stroke), Enhancing a Multidisciplinary Research Network for Research and Quality in Epilepsy and CP (PI Ostendorf, Pediatric Epilepsy Research Foundation), Speech and Language Predictors of Participation for Children with CP (PI Allison, CP NOW), and Feasibility of Adding Grip Strength Measures to Body Composition Assessments in Individuals with CP (PI Hurvitz, Foundation for Physical Medicine and Rehabilitation).
Determining top priorities
Eight of the 10 CP Research Network executive committee leaders ranked top priorities and were available virtually to review component scores for each domain and determine the top six component priorities moving forward. Consensus was reached by rankings for development of leaders within the Systems of Leadership domain (85%) and financial sustainability within Governance and Management domain (100%). Consensus for the domains of Quality Improvement, Engagement and Community Building, Data and Analytics, and Research was not reached by rankings and occurred with discussion. After discussion, 100% agreement was reached for QI education and training (QI domain), patient reported data (Engagement and Community domain), data quality and validation (Data and Analytics domain), and primary data collection (Research domain). These components were selected as the group agreed growth in these areas would likely result in significant impact on their respective domains as well as across several other domains.
Discussion
The purpose of this paper is to report on the CP Research Network’s progress toward developing as an LHN and provide detailed information about the strengths and opportunities for improvement.
The assessment indicates the CP Research Network LHN is strongest in the domains of Systems of Leadership and Governance and Management with relative weaknesses in Quality Improvement, Engagement and Community Building, Data and Analytics, and Research. It is not surprising that scores in Systems of Leadership and Governance and Management were highest as these areas are foundational to initial startup before growth can occur in other domains of the network.
Scores on the individual components within domains revealed the network has reached a score of at least intermediate (3 or higher) in 19 components and below intermediate (less than 3) in 31 components. Two components achieved a mature score of 4 or higher in common purpose and expectation that parent, patients, clinicians and researcher are co-creators. None of the components achieved a score of 5 or idealized state. These scores are similar to those of other young networks of approximately two years of age including All Children Thrive, the Autism Treatment Network, the Cystic Fibrosis Learning Network, and the Improving Renal Outcomes Collaborative, which assessed their maturity of most domains below 3 [18]. The CP Research Network maturity scores in this study seem appropriate for the length of time since its launch in 2015 and the beginning of data collection and assimilation. The CP Research Network maturity scores in this study were lower than more mature networks such as Improve Care Now at age 10 years, which reported most domain scores at or above maturity with scores near 4 [18].
Review of the NMG scores with CP Research Network leaders identified six areas of focus moving forward. These are development of leaders, financial sustainability, QI education and training, patient reported data, data quality and validation, and primary data collection. With regard to a focus on developing leaders, a recent paper describing the development of LHS leadership provides excellent guidance. Forrest ([29] describes core competencies including systems science, standards of scientific evidence, research methods, informatics, ethics of research, implementation and improvement science, engagement, leadership, and research management.
Similar to other LHNs that describe stable financial support as a barrier [17, 30], the CP Research Network is exploring more stable funding sources. A five-year strategic planning process initiated in 2020 set the priority to build an entity structure that would support multiple revenue streams including grants, participation fees, philanthropy, and sponsorship. With the exception of DCC staff, network participation in operations is voluntary. While external collaborations were initially dismissed to avoid any potential for undue influence or appearance of conflict, the network is considering establishing procedures for collaborating with industry. Greater financial support would allow the network to increase the number of dedicated staff. The CP Research Network currently has less than four full-time staff whose time is committed to work of managing the network, while other more mature networks have up to 15 with a reported range of 2.6–15.5 depending on the age of the network [18]. Although there has been progress made, the network is not as advanced at the five-year mark as was hoped. Yet, the time invested to develop the necessary infrastructure and the number of volunteer hours many of the members dedicated to building the network is appreciated.
There were several areas in the QI domain scoring below a 3, and the study team felt it was important to improve in all these areas. However, improving QI education and training would lead to improvement in the other areas of the domain, and they agreed to start with a focus on this. Although the CP Research Network does include four leaders with QI education, the study team acknowledges there are opportunities to increase QI knowledge of working groups at each institution to strengthen and support the execution of improvement activities.
Within the Engagement and Community Building domain, the study team agreed that focusing on patient reported data should be a priority in the coming years. If collected routinely, patient reported data, that had an average component score of 2.9, could be used by the system for management, research, and improvement. The network has focused on collecting clinical data and anticipates improving the standardization of information collected during a clinic visit; simultaneously, it is currently working on integrating several validated, CP-specific patient reported outcome measures into the EHR.
Like other LHNs [31], the CP Research Network clinical registry also reports missing or incomplete data. For this reason, the study team agreed that focusing on data quality and validation in the next three to five years would be foundational to future growth not only in the Data and Analytics domain but would also increase the ability to conduct observational and comparative effectiveness studies (Research domain). Stakeholders have identified observational and comparative effectiveness studies as critical given the heterogeneity and lifespan course of CP [22, 32]. Closely related to data quality and validation is the component of primary data collection (Research domain). Improvements in primary data collection should be a focus in the coming years and would have ripple effects towards improvement in other components of the network. Efforts to increase the number of subspecialties submitting data on patients at each institution are needed.
The present study has limitations. The sample of respondents was limited to 13 of 19 leaders that were invited to participate, although these respondents represent a spectrum of disciplines and institutions. Similar to Lannon’s [18]. report of nine networks assessing growth with the NMG, respondents in this study felt many components were interdependent and growth in one area is likely to lead to growth in another. Likewise, low scores in one component are likely to relate to low scores in another component. However, the study team felt the NMG was thorough in its assessment of several domains and components of domains which elucidated areas in need of greater focus and growth. All respondents indicated this was helpful in providing an overview of the network’s current strengths and areas important to develop further. All agreed that utilizing the NMG tool to conduct regular self-assessments of the network would be beneficial moving forward. Results from this assessment will be utilized at strategic planning events to develop action plans and guide the network’s future growth in the identified areas.
Conclusion
The CP Research Network has made substantial progress towards becoming an LHN since its launch in 2015. Results from this project will provide the network with a baseline for systems changes to prioritize areas for growth and track improvement of the network over time. Implications of the network are far reaching for those within and outside of the network. The breadth of participating clinical disciplines and diversity in practice settings and geography will allow the CP Research Network to produce information that is generalizable to clinicians and families receiving care at centers not enrolled in the network. Though network activities are rapidly disseminated through a variety of channels and can be monitored to stay abreast (
Supplementary data
The supplementary files are available to download from
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors have no conflicts of interest to disclose.