
Abstract
PURPOSE:
Cerebral palsy is a common pediatric neurological problem that has multiple comorbidities, including nutritional issues. Hematological and biochemical parameters significantly affect the health status of patients with cerebral palsy, and till now very few studies have analyzed these parameters. This study aimed to describe the hematological and biochemical parameters of children diagnosed with cerebral palsy.
METHODS:
This four-year observational study included children with cerebral palsy who were admitted to the Department of Pediatrics of a medical college teaching hospital.
Hemoglobin, platelet count, white blood count (WBC), red blood cells (RBCs), packed cell volume, RBC indices, and biochemical parameters (urea, creatinine, total bilirubin, total protein, albumin, globulin, aspartate transaminase, alanine transaminase, electrolytes, calcium and alkaline phosphatase) were noted and values (mean, standard deviation, and interquartile range) presented. Age and gender-based analyses were performed.
RESULTS:
The average hemoglobin level was 11.48 mg/dl, platelet count was 301.24×109/L, and WBC count was 11.13 109/L. Anemia was observed more commonly in males younger than nine years of age. Of 282 patients, 14 (4.96%) had a platelet count of less than 150×109/L. Abnormal alkaline phosphatase levels were observed more commonly in patients who were younger than nine years of age and in females more than males, and the difference was statistically significant. Protein levels and calcium levels were similar between both age groups.
CONCLUSION:
Anemia was more common in younger patients and males with cerebral palsy. Abnormal bone turnover markers (alkaline phosphatase) were more common in young patients and females with cerebral palsy. Understanding the differential effect of age and gender on various investigational parameters will help improve care of children with cerebral palsy by initiating appropriate and timely clinical interventions, thereby providing a better quality of life.
Introduction
Cerebral palsy (CP) has been defined as “a group of permanent disorders of the development of movement and posture, causing limitation of activity, that are attributed to non-progressive disturbances that occurred in the developing fetal or infant brain” [1]. The prevalence of CP in the USA has remained approximately the same at around 3.5 per 1,000 births [2]. Though there was a brief reduction in the prevalence of CP in Western countries, it has begun to rise again [3]. In India, the prevalence of CP is approximately 2.8 per 1,000 births and has not changed much over the last two decades [4]. Considering the large population of India, the burden of CP is huge as it is one of the major neurodevelopmental disorders among Indian children [5]. One study in India estimated that almost two-thirds of the patients with CP had a moderate or severely affected healthcare-related quality of life [6].
Children with CP have various needs, and many articles in recent Indian medical literature have focused on the neurological problems and neurorehabilitation of these patients. They also have poor nutrition, leading to poor overall health status. Favero et al. [7] have focused on the nutritional and food intake profile of CP and found that reduced intake, gastrointestinal motility issues, and poor absorption are all contributors to the abnormal nutritional status of children with CP. Al-Muneef et al. [8] and Omeroglu et al. [9] have noted similar findings of malnutrition in children with CP.
In the Indian context, Hariprasad et al. [10] have estimated hemoglobin and vitamin D levels as part of a comprehensive evaluation of children with CP and have highlighted the contribution of nutritional deficiencies to the overall burden of morbidity in children with CP. While anthropometric measurements are the mainstay for identification of nutritional disorders, hematological and biochemical investigations are also important indicators of nutritional status. There is a paucity of literature available on the basic hematological and biochemical parameters of children with CP, and this therefore formed the basis of the current study. The study was performed with the limited data (investigational parameters) that were already available, with the following objectives: 1) to describe the hematological and biochemical parameters of children with CP and 2) to assess the influence of age and gender on these parameters.
Materials and methods
This was a retrospective observational study conducted in the Department of Pediatrics of a medical college teaching hospital in urban south India.
Institutional Ethics Committee clearance was obtained. Medical records from 2015–2019 of children with CP, diagnosed using conventional clinical examination methods, were studied.
Children admitted to the pediatric ward for evaluation and/or for diagnosis of CP or for rehabilitative measures referred from other centers were included. Hematological and biochemical characteristics were noted.
The hematological parameters included hemoglobin (Hb), platelet count, white blood count (WBC), red blood cells (RBCs), packed cell volume, mean corpuscular Hb (MCH), mean corpuscular volume (MCV), mean corpuscular Hb concentration, red cell distribution width (RDW) and mean platelet volume.
The biochemical parameters included urea, creatinine, total bilirubin, direct bilirubin, total protein, albumin, globulin, aspartate transaminase, alanine transaminase, and electrolytes (sodium, potassium, and chloride). Investigations indicating the bone status (calcium and alkaline phosphatase [ALP]) were also included. The hormonal assay test for thyroid stimulating hormone (TSH) was also noted.
The values of all the patients were collected, and statistical analysis was performed.
Statistical analysis
The values were analyzed and tabulated using Microsoft Excel. Mean and standard deviation were calculated for the parameters. The frequency distribution of the values was presented in the form of tables or appropriate representational tools. Intra-group analyses of a few of the significant investigations (Hb, protein, calcium, and ALP) were performed to assess the influence of age (younger than nine years/older than nine years) and gender (male/female) on these parameters using chi-squared tests. Analysis was performed using Microsoft 365 Excel withStatPac.
Results
Two hundred and eighty-two children with CP were included over the four-year period. There were 184 males and 98 females in the study. The average age of the study population was 7.18±3.83 years. The average age of the males was slightly higher (7.52 years), and that of the females was 6.55 years. The age distribution of the study subjects is shown in Fig. 1. Age (by sex) distribution.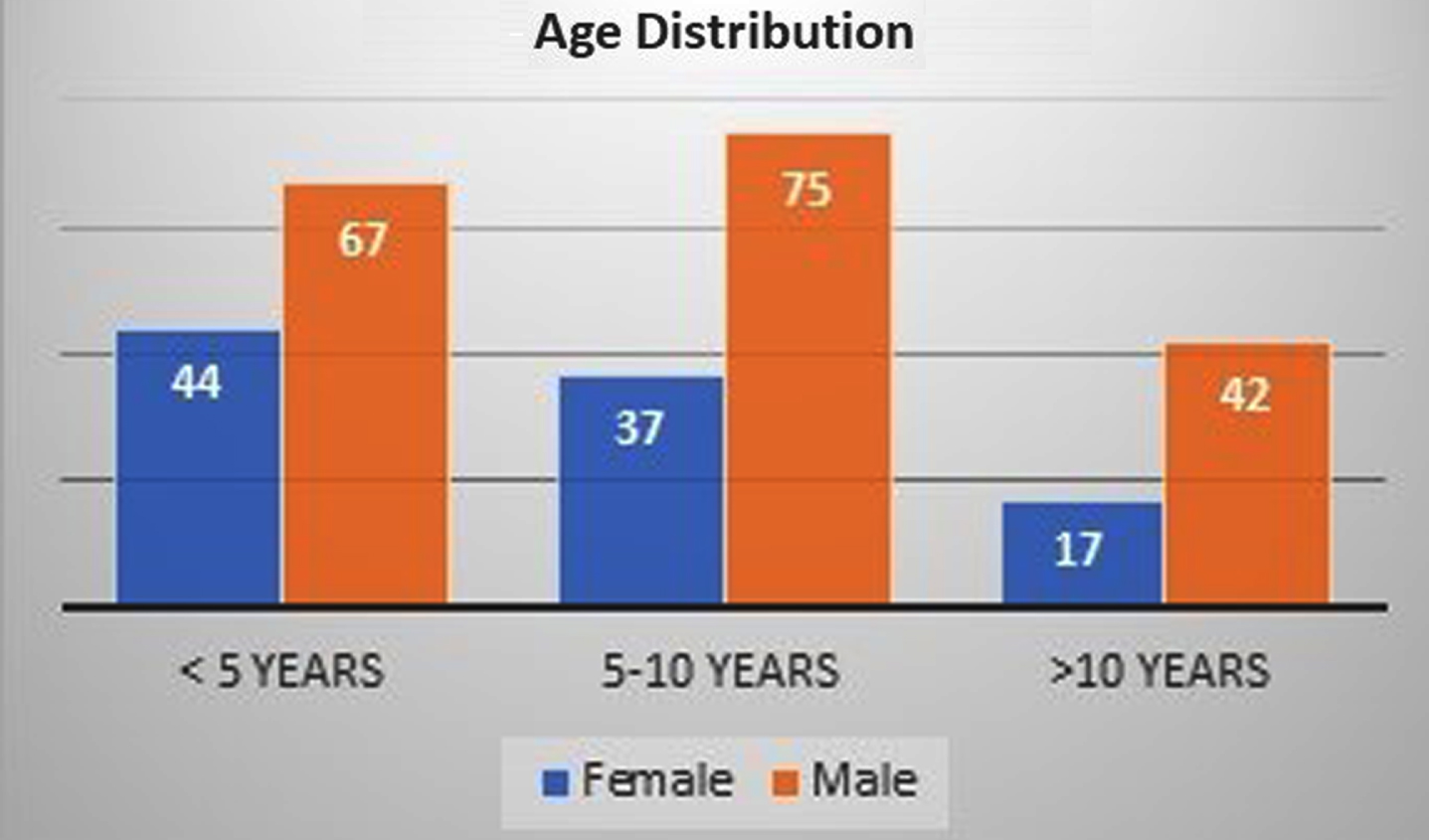
While hematological results were available for all the patients, the biochemistry values were available for only 244 patients. The average Hb value was 11.48 g/dl, platelet count was 301.24 109/L, and WBC count was 11.13 109/L. Further details are presented in Table 1. The biochemical results (renal function and liver function) are listed in Table 2.
Hematological results
Biochemistry results: Renal function and liver function
Influence of age on investigation parameters
As shown in Fig. 2, four patients had a Hb value of less than 8 gm/dl. Thirty-one patients (10.99%) had a Hb value between 8 and 10 gm/dl. The majority of the patients had a normal Hb value. Fourteen patients (4.96%) had a platelet count of less than 150×109/L. Fourteen patients (5.77%) had hypocalcemia (<8.8 mg/dl), and 21 patients (8.6%) had a protein value of less than 6.4 mg/dl.
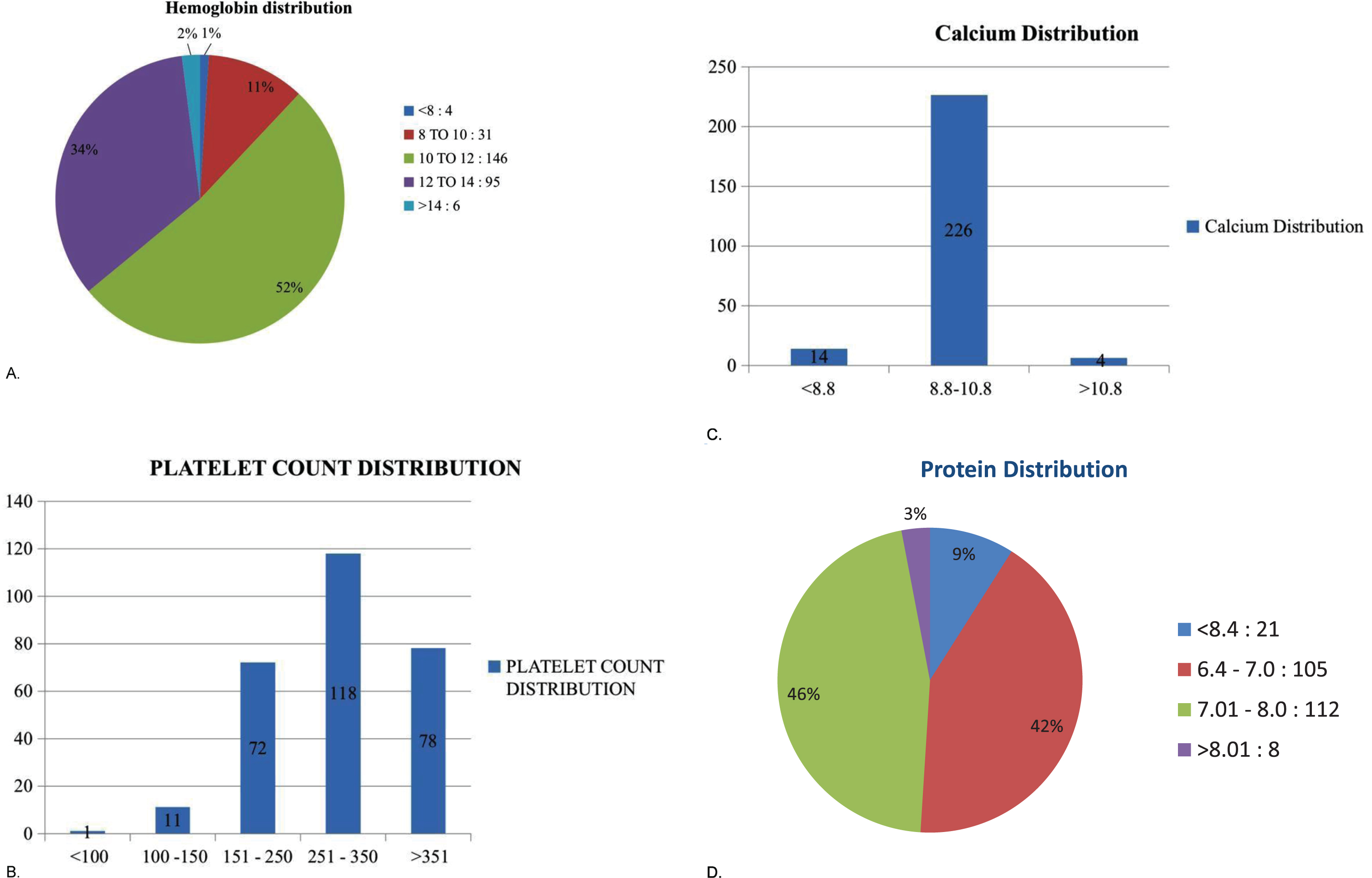
Distribution of investigation parameters by age.
Anemia was noted in 36.17% of those younger than nine years and 15.95% of those older than nine years (nine being the median age value), but the difference was not statistically significant (p-value = 0.13). Among males, anemia was noted in 31.5% of those younger than nine years and 17.3% of those older than nine years with a statistically significant difference (p-value = 0.03).
High ALP values were noted in 23.04% of those younger than nine years and 3.54% of those older than nine years, and the difference was statistically significant (p-value = 0.004). Hypocalcemia (3.9% vs 1.06%) and hypoproteinemia (3.1% vs 1.06%) were similar in both age groups.
Elevated ALP was seen in 75 children (26.59%). As per details shown in Table 4, high ALP was more commonly observed in patients younger than nine years and in females, and both these differences were statistically significant. There was no difference noted in the calcium or protein levels between the different age groups and genders.
Influence of gender on ALP values
Specific interventions have been done to improve the disabilities and limitations faced by children with CP. While the role of the healthcare providers in providing this care is commendable, this study sought to explore a broader approach to the health status of children with CP by studying their basic biochemical parameters. Most of the studies described below attempted to provide a correlation between severity of CP and nutritional status or the effect of an intervention on nutritional status. However, this study focused only on describing the baseline biochemical parameters in a relatively large population.
Hb
The importance of this study lies in the fact that it reported the range of hematological parameters in a reasonably large number of children with CP (n = 282, age 7.18±3.83 years). The average Hb value in this study was 11.48±1.398 g/dl. This is similar to a study done by Favero et al. (n = 40, age 6.7±2.4 years), wherein the Hb value was 11.0±6.0 g/dl. However, Omeroglu et al. [9] showed a mean Hb value of 13.4±1.2 g/dl in a study that focused on hematological assessment of patients with CP (n = 62, mean age 8.8 years). In the current study, the proportion of children with CP with anemia was found to be 52.12%. It was assumed that most of these cases were due to nutritional deficiency/iron deficiency anemia. A closer look into the RBC indices suggested that MCV was lower than normal in only 32% of the population. This discrepancy in the hematological abnormalities suggested that it could also be due to thalassemia traits. However, Hb electrophoresis was not performed for any patient, which is a limitation of the current study. One reason for not performing the test was that the center is located in the southern part of India, where hemoglobinopathies are much less prevalent than the northern and eastern parts of India, where they are most common. Hb electrophoresis could be considered in future evaluation of children with CP.
Hariprasad et al. [10] have reported a slightly higher prevalence of anemia, with 63% moderate anemia and 12% severe anemia. Herein, the sample size was 41, while the current study included a much larger number of patients (282). Hariprasad et al. and Goyal et al. [11] have highlighted the importance of the contribution of poor hematological status in compounding physical and functional impairments in CP.
In a study by Almuneef et al. [8], the prevalence of anemia was 43%. In the current study, the prevalence of anemia was 10.9%. The importance of anemia in children with CP has also been highlighted by Elshemy et al. [12]. They used the Peabody Developmental Motor Scales-2 and showed that anemic children with CP have poor gross and fine motor activity. The current study has not analyzed the relationship between hematological parameters and CP severity, which is one limitation of the study. Serum ferritin was not part of the analysis in the current study. Mohan et al. [13] have highlighted the importance of iron deficiency using serum ferritin analysis in children with CP. However, their study was a retrospective analysis of only 35 patients.
In the current study, anemia was more common in males as compared to females. This gender disparity has not been reported by most of the previously mentioned articles. This result cannot be applied universally because of the unequal representation of male and female patients in this study, but it might lay the foundation for further investigations into acceptable baseline values that can be used as reference values in clinical application.
Papadapoulous et al. [14] have also reported a high incidence of anemia in children with CP in Greece. In their 108-patient study, 33% were found to have microcytic hypochromic anemia, which is comparable to this study (38%). However, they observed no statistical difference in the incidence of anemia at various age groups. In the current study, younger (<9 years) male children had a higher proportion of anemia than the other groups. Although the reason behind this needs further analysis, it could be that more males (184 in number) were in this study than females (98). The onset of puberty could also cause some biochemical changes in children with CP of this age group; puberty was not considered while evaluating the children, which is a limitation of this study.
This study had only one patient with megaloblastic anemia (1/282, 0.35%). As such, severe megaloblastic anemia with CP was a rare association. One case report by Ahmad et al. suggested that folate malabsorption should be suspected when this association is noted [15]. The findings of the current study were compared with that of Omeroglu et al. [9] with respect to the following parameters: MCV (fL) (81.0±4.1 vs 76.54±9.7); MCH (27.8±1.7 vs 24.58±3.52); RDW (13.5±0.9 vs 15.73±3.28) and platelet count (309.0±77.1 vs 301.24±102.88) respectively. The similarity in the findings between this study and Omeroglu et al.’s suggests that iron deficiency anemia may be a common finding among children with CP. There was wide variation in WBC (x 109/L) between the study by Omeroglu et al. and this study (7.8±1.9 vs 11.13±3.78), suggesting that changes in WBC is not a common finding in childrenwith CP.
Platelet count
Approximately 5% (14/282) of the patients had a platelet count of less than 150×109/L. These were incidental findings, and there were no symptoms attributable to the thrombocytopenia. As such, thrombocytopenia was not a common finding in CP. A detailed literature search led to the identification of only a few case reports on associations that have been inadequately studied such as the relationship between neonatal alloimmune thrombocytopenia, subsequent intracranial vascular events, and CP [16].
Micronutrients
Though various micronutrient levels were not measured in this study, they have been shown to be lower in children with CP. In a North Indian population described by Kalra et al. [17], copper, zinc and magnesium levels were much lower in children with CP compared to controls, and supplementation of these micronutrients has been recommended.
Calcium, ALP, and bone health
In this study, low calcium values were seen in 16 children (5.67%) and high ALP values were seen in 75 children (26.59%), but vitamin D levels were not available. In a systematic review conducted by Mergler et al. [18], it was found that only low-quality evidence existed in the matter of bone health among patients with CP. The risk of fractures approached approximately 4% (which is much higher than a general population), highlighting the importance of assessing bone health in children with CP. Scheinberg et al. [19] have also described poor bone health in children with CP in Brazil.
In a study from Pakistan [20], 86 children with CP with a mean age of 6.08±2.89 years were studied. Hypocalcemia was noted in 40.7% of the study population. However, in the current study, only 5.73% (14/244) of the study population showed hypocalcemia.
In Akhter et al.’s study [20], 37.2% showed low values of ALP, whereas in the current study, there were no patients with low ALP values. Most of the younger patients had a higher ALP value than expected. The significance of this finding is not clear, especially in the context of vitamin D values not being available. This merits further study. Low phosphorus (39.53%) and low vitamin D levels (66.2%) were seen in Akhter et al.’s study [20], but these parameters have not been evaluated in the current study.
Poor bone metabolism is a significant problem in children with CP, and various measures such as oral calcium (with vitamin D) supplementation, weight bearing exercises, and bisphosphates have been suggested by many studies [21]. The large number of patients with near-normal bone metabolism in this study may imply good compliance totherapy.
Hematological and biochemical parameters of a large set of patients with CP have been presented, and it is hoped that this can be used as a reference range when dealing with children with CP. Anemia was more common in younger patients and males. Abnormal bone turnover markers (ALP) were more common in young patients and females. To conclude, understanding the differential effect of age and gender on various investigational parameters will help improve care of children with CP by initiating appropriate and timely clinical interventions. Aside from rehabilitative measures, treating the underlying hematological and biochemical abnormalities in children with CP will help them achieve a better quality of life and respond to treatment earlier in their rehabilitation journey.
Conflict of interest
No conflicts of interest or funding to disclose.