
Abstract
PURPOSE:
To evaluate the efficacy and safety of radial extracorporeal shock wave therapy (rESWT) according to total number of pulses on hamstring muscle spasticity in children with spastic type cerebral palsy (CP).
METHODS:
This study is a randomized controlled trial consisting of thirteen patients with spastic CP, 9 males and 4 females, aged 5 to 14 years (mean age 9.2). Twenty-five spastic hamstring muscles were divided in four groups. Group I: 500 pulses, Group II: 1,000 pulses, Group III: 1,500 pulses, and Group IV: 2,000 pulses. Australian Spasticity Assessment Scale (ASAS) was measured at four different time points (pre-ESWT, post-ESWT, 2 weeks post-ESWT, and 4 weeks post-ESWT).
RESULTS:
All four groups showed improvement in ASAS relative to pre-treatment, although only significant in Group III (1,500 pulses). There were no statistically significant differences in ASAS between all four groups in pre-ESWT [|2(2) = 3.907, p = 0.272], immediately post-ESWT [|2(2) = 1.250, p = 0.741], 2 weeks post-ESWT vs pre-ESWT [|2(2) = 3.367, p = 0.338], and 4 weeks post-ESWT vs pre-ESWT [|2(2) = 1.566, p = 0.667].
CONCLUSION:
The effect of rESWT on spastic hamstring in children with spastic CP is not dependent on the number of pulses.
Introduction
Cerebral palsy (CP) is a group of permanent disorders affecting movement and postural development that are caused by non-progressive disruptions of the brain, usually occurring during fetal period or infancy. It is commonly accompanied with sensory disorders and learning disability [1]. In 2016, more than 17 million people are affected by CP with a prevalence of 1.5 to 2.5 per 1,000 live births [2]. CP remains to be the most common cause of severe physical disability in children. The Centers for Disease Control and Prevention (CDC) estimated an economic cost of US $4.1 million per CP patient that is comprised of medical services, special education, and productivity loss [3].
The most common form of CP is spastic motor type. Spasticity is defined as a velocity dependent hypertonia due to hyperexcitable stretch reflex [4]. In CP, it usually occurs in multiple muscle groups. The most commonly affected lower limb muscles in CP include gastrocnemius, soleus, hamstrings, rectus femoris, adductors, and psoas [5]. The severity of spasticity in CP can usually increase with age, and if left untreated, it can result in muscle weakness, muscle atrophy, permanent contractures, and deformities, leading to activity limitation [6]. As such, treating spasticity becomes a crucial part in the management of spastic type CP.
Current management of spasticity involves physical manipulation such as passive stretching and splinting, sometimes combined with oral pharmacologic treatment, intrathecal baclofen therapy, and botulinum toxin injection [7, 8]. At times, surgical procedures such as Selective Dorsal Rhizotomy (SDR) can also be considered [9, 10]. Botulinum toxin injection has been shown to reduce spasticity for up to 6 months, however, the cost of the procedure (Rp 5,000,000/vial –equivalent to US$ 360/vial) remains to be an issue in developing countries like Indonesia [11]. Moreover, botulinum toxin injection is currently not covered by Indonesia’s National Health Insurance program, making it inaccessible to many Indonesian CP patients. Therefore, other modalities such as a non-invasive therapy should be considered as an alternative treatment for spasticity.
Radial Extracorporeal Shockwave Therapy (rES-WT) is a non-invasive treatment that has been shown to effectively improve spasticity in patients with spastic motor type CP, despite unclear underlying mechanism [12–15]. It is a promising treatment, especially considering the cost of rESWT procedure, which is approximately Rp 300,000/session (equivalent to US$ 22/session). Some speculate that the decrease in spasticity is caused by physical changes to actin-myosin linkages, cellular membrane permeability, release of ATP, and modulation of angiogenesis through cellular mediators such as von Willebrand factor [14, 16–18]. According to the International Society for Medical Shockwave Treatment (ISMST), there has yet to be a recommended guideline for the treatment of spasticity in children using rESWT [19]. As such, the research that had been conducted for the treatment of spasticity in patients with spastic motor type CP has varying parameters in terms of Energy Flux Density (EFD), repetition frequency, and number of pulses [12–15]. One crucial physical parameter needed to be determined is the number of pulses required to efficiently reduce spasticity. Given the same frequency (Hz), the number of pulses directly affects the duration of ESWT per session (the higher the number of pulses given, the longer the therapy session). This may be a concern for spastic motor type CP due to accompanying sensory and learning disabilities. Therefore, the objective of this study was to understand whether the reduction in hamstring stiffness in children with spastic CP could be influenced by the number of pulses in a single ESWT session [20].
Methods
This study was designed as a randomized controlled trial. The participants and clinician performing the ESWT were not blinded.
Subjects
Thirteen children with spastic CP from the outpatient clinic of the Department of Physical Medicine and Rehabilitation at Rumah Sakit Umum Pusat Nasional Dr. Cipto Mangunkusumo (RSCM) participated in the study. Patients were recruited using the following inclusion criteria: 1) patients with spastic CP aged 5 to 18 years old, 2) at least one hamstring with an Australian Spasticity Assessment Scale (ASAS) of 2 or more, 3) time gap of at least 6 months since the last botulinum injection on hamstring, 4) no surgical operation on lower limb within the last 12 months, 5) absence of severe contracture (loss of greater than two-thirds hamstring range of motion as measured with a goniometer) on hamstring, and 6) ability of legal respondent to give written informed consent. Twenty-five spastic hamstring muscles found in 13 patients were randomly allocated to four groups: 500 pulses, 1,000 pulses, 1,500 pulses, and 2,000 pulses. The left and right hamstring muscles for each individual were allowed to be allocated into different treatment groups. The study participants and guardians were not explicitly given information on the number of ESWT pulses, however since the duration of ESWT application was different between groups, blinding was not possible for this current study. All groups had routine rehabilitation, including physiotherapy. Ethical approval was obtained from the Ethical Committee of Faculty of Medicine, University of Indonesia –RSCM.
Data on spastic hamstring muscles in children with cerebral palsy
Data on spastic hamstring muscles in children with cerebral palsy
Values are presented as mean±standard deviation or number. Group I: 500 pulses; Group II: 1,000 pulses; Group III: 1,500 pulses; Group IV: 2,000 pulses. *p < 0.05.
Spasticity of hamstring was evaluated as the degree of resistance to passive movement using ASAS (0: no spasticity to 4: severe spasticity). Evaluations were done at four time points: 1) pre-ESWT, 2) immediately post-ESWT, 3) 2 weeks post-ESWT, and 4) 4 weeks post-ESWT. All patients were examined by the same physiatrist with the patient lying in a supine position on the stretcher. One physiatrist performed the ASAS measurement on all participants pre- and post-ESWT without being given information on the number ESWT pulses given to the hamstring muscles.
ESWT
BTL-6000 SWT Topline (BTL, Czech Republic) was used to apply rESWT on hamstring muscles, with the subject lying in a prone position. The pressure pulses were applied to each hypertonic hamstring muscle at the biceps femoris long head, semitendinosus, and semimembranosus. All impulses were applied in the middle of the respective muscle belly with a radius of 2.5 cm. The energy flux density was constant at 0.1 mJ/mm2 and the repetition frequency was at 4 Hz, with a pressure of 1.5 bars. Twenty-five different spastic hamstring muscles from 13 CP patients were allocated into four groups –each receiving a varying total number of pulses (group I: 500 pulses, II: 1,000 pulses, III: 1,500 pulses, and IV: 2,000 pulses).
Number of pulses in respective muscle belly in each group
Number of pulses in respective muscle belly in each group
No anesthesia was given. Adverse events were closely monitored during and after therapy.
Intra-group changes in ASAS were evaluated with Friedman analysis of variance from baseline immediately post-ESWT, 2 weeks post-ESWT, and 4 weeks post-ESWT; followed by post-hoc Wilcoxon signed-ranked test. Inter-group ASAS at 4 time points were analyzed using Kruskal-Wallis test. Statistical analysis was conducted using SPSS ver. 23.0 (IBM Corporation, Armonk, NY, USA). The level of significance was set at < 0.05.
Results
No significant difference between pre-treatment groups was observed with respect to age, sex, body weight, and ASAS of hamstring.
Friedman analysis of variance identified significant intra-group differences in four different ASAS measurements (pre-ESWT, immediately post-ESWT, 2 weeks post-ESWT, and 4 weeks post-ESWT) in all four groups. Group I |2(2) = 10.026, p = 0.018; group II |2(2) = 13.997, p = 0.003, group III |2(2) = 17.019, p = 0.001, and group IV |2(2) = 14.122, p = 0.003.
Post-hoc analysis with Wilcoxon signed-rank tests was conducted with a Bonferroni correction applied, resulting in a significance level set at p < 0.017.
For group I, there were no significant differences between pre-ESWT and immediately post-ESWT (Z = –1.633, p = 0.102), between pre-ESWT and 2 weeks post-ESWT (Z = –1.890, p = 0.059), and between pre-ESWT vs 4 weeks post-ESWT (Z = –2.060, p = 0.039).
For group II, there were no significant differences between pre-ESWT and immediately post-ESWT (Z = –2.271, p = 0.023), between pre-ESWT and 2 weeks post-ESWT (Z = –2.232, p = 0.026), and be-tween pre-ESWT and 4 weeks post-ESWT (Z =–2.060, p = 0.039).
For group III, there were no significant differences between pre-ESWT and immediately post-ESWT (Z = –2.121, p = 0.034). However, there were statistically significant reduction in ASAS in pre-ESWT vs 2 weeks post-ESWT (Z = –2.460, p = 0.014) and between pre-ESWT and 4 weeks post-ESWT (Z = –2.456, p = 0.014).
For group IV, there were no significant differences between pre-ESWT and immediately post-ESWT (Z = –1.857, p = 0.063), between pre-ESWT and 2 weeks post-ESWT (Z = –2.271, p = 0.023) and be-tween pre-ESWT and 4 weeks post-ESWT (Z =–2.232, p = 0.026).
To compare ASAS between the four groups (inter-group) at four different time points, a Kruskal-Wallis test was conducted. There were no statistically significant differences in ASAS between all four groups in pre-ESWT [|2(2) = 3.907, p = 0.272], immediately post-ESWT [|2(2) = 1.250, p = 0.741], 2 weeks post-ESWT vs pre-ESWT [|2(2) = 3.367, p = 0.338], and 4 weeks post-ESWT vs pre-ESWT [|2(2) = 1.566, p = 0.667].
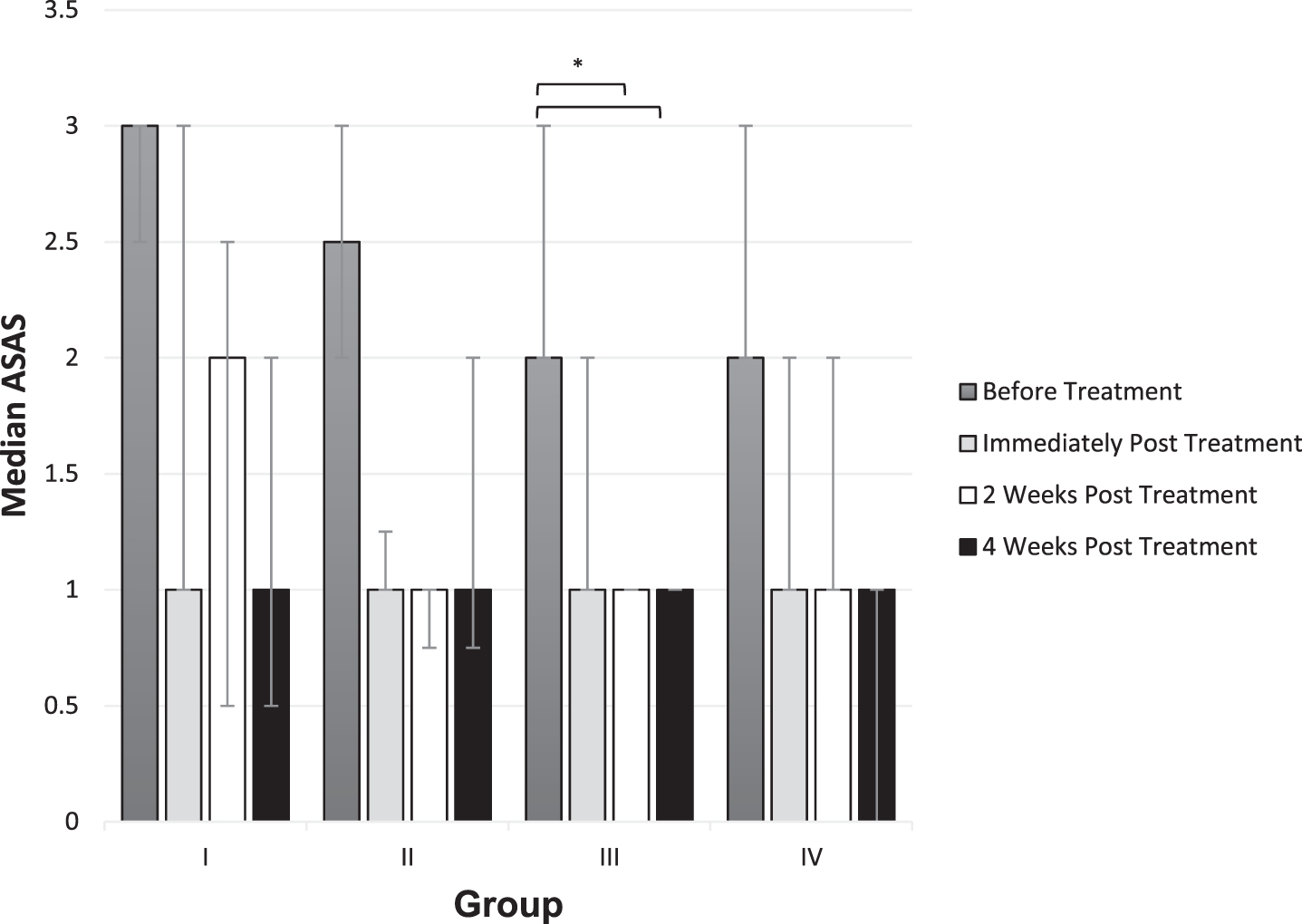
ASAS Measurement - before treatment, immediately post-treatment, 2 weeks post-treatment and 4 weeks post-treatment. There are no significant differences between groups. Whiskers represent IQR. *p < 0.017, derived from Wilcoxon signed-rank test with a Bonferroni correction for assessment time relative to BT (intra-group).
Immediately after one ESWT, children with spastic type CP showed reduced hamstring muscle spasticity in all doses. This was the first study to assess the effect of ESWT dose on spasticity in spastic CP children.
In this study, rESWT was conducted at energy flux density constant at 0.1 mJ/mm2 and repetition frequency at 4 Hz, with a pressure of 1.5 bars, similar to Vidal et al., except for the fact that Vidal et al. used 8 Hz instead of 4 Hz. A frequency of 4 Hz was chosen to reduce pain during the rESWT procedure [13, 21]. Several studies such as Park et al. also used a frequency of 4 Hz to treat gastrocnemius spasticity in children with CP [15]. Additionally, the pressure pulses were applied to each hypertonic hamstring muscle belly at the biceps femoris long head (50%), semitendinosus (25%) and semimembranosus (25%) with a radius of 2.5 cm [22, 23].
In one previous study, a single session of ESWT with 1,500 pulses (energy flux density 0.030 mJ/mm2 and repetition frequency of 4 Hz) was given to spastic gastrocnemius muscles in children with spastic type CP. It was found that there was a significant immediate reduction in spasticity, however, this improvement did not persist 3 weeks post-ESWT [15]. In this study, 1,500 pulses were given to hamstring muscles at energy flux density 0.1mJ/mm2 and repetition frequency of 4 Hz, showing a significant immediate improvement in spastic hamstring that lasted for 4 weeks. In one other study, a single ESWT with 1,500 pulses and energy flux density 0.030 mJ/mm2 directed at plantar flexor muscles in patients with spastic type CP reported a significant reduction in spasticity 4 weeks post-treatment, similar to the present study [12]. The differences in muscle groups (gastrocnemius vs plantar flexors vs hamstrings) and energy flux density (0.03 mJ/mm2 vs 0.1 mJ/mm2) might account for the differences in duration of spasticity improvements between the three studies. However, this current study is consistent with findings in Park et al. and Amelio et al. that rESWT with 1,500 pulses, even with different EFDs, can result in immediate improvement in spasticity [12, 15].
In another paper, a single session of ESWT with 2,000 pulses (energy flux density 0.030mJ/mm2 and repetition frequency of 8 Hz) was delivered to a group of spastic muscles (biceps brachii, wrist flexors, hip adductors, gastrocnemius, soleus, and hamstrings) in patients with spastic CP. It was found that there was a reduction in spasticity one month post-ESWT [13]. Similar to this present study, with 2,000 pulses, there were significant improvements in ASAS in spastic hamstring muscles 1 month post-ESWT. There was no information regarding whether there was an immediate reduction in spasticity post-ESWT.
There were no differences in ASAS between all four groups immediately post-ESWT, 2 and 4 weeks post-ESWT. In this present study, a single ESWT session with 500 pulses can result in immediate spasticity improvements similar to all other doses. A smaller number of pulses, with the same frequency (Hz) would mean a shorter session of ESWT. A 500 pulses ESWT with a frequency of 4 Hz requires 2 minutes and 5 seconds while a 2,000 pulses ESWT with similar frequency requires 8 minutes and 20 seconds. This is an important factor for consideration since most CP patients also have accompanying sensory disorders and learning disabilities. Furthermore, in order to target the hamstring muscles, the patients had to lie in a prone position, which was uncomfortable for CP patients. As such, a single session of ESWT with a total of 500 pulses could be preferred over higher number of pulses for the treatment of hamstring spasticity in CP patients.
All of the patients completed the study. No adverse events such as pain, dysesthesia, headache, or swelling were reported during the treatment session and up to four weeks post-ESWT. The parents of all participants were satisfied with the improvements in spasticity, stating that the process of dressing and undressing became more manageable. All parents were willing to undergo another session of ESWT. Many stated that the study on quality of life, such as using Pediatric Quality of Life Inventory (PedsQL) could be conducted to understand the improvement in quality of life of spastic CP patients from ESWT [24]. Determining specific individual scales of PedsQL that are related to hamstring muscles such as “Daily Activities”, “Movement and Balance” and “Pain and Hurt” could be recommended instead of using the entire PedsQL [25]. Considering that ASAS is a subjective assessment and a blunt instrument to measure spasticity, supplementing it with other measurements such as participant and carer (parent) satisfaction and inclusion of range of motion at joints pre-post using the Tardieu scale would be valuable to further support this study. It should be noted that only the severity of spasticity was taken into consideration and not the current functional status of the subjects.
Some limitations of this study include small sample size and short follow-up period. It only showed that all four different doses of ESWT can result in spasticity improvement up to 4 weeks post-treatment. A longer follow-up period would be necessary to determine the duration of spasticity improvement in a single ESWT session. This would translate to the time needed for the patients to undergo another session of ESWT. Another limitation was that different doses of ESWT (one dose in the right hamstring and a different dose in the left hamstring) were given to the same patient as the randomization process was done based on a single hamstring muscle. Given the fact that spasticity can vary according to many factors such as fatigue and stress of the study participants [26], applying ESWT to one hamstring of subjects with symmetrical spasticity (same ASAS between left and right hamstring) would be more ideal. In this study, all four groups received ESWT and were assessed by a single rater who was informed that all subjects had undergone ESWT despite not being given information on the dose received by each subject. To minimize rater bias on assessment of the actual treatment’s effects, it is recommended to include a fifth group of subjects who did not receive ESWT.
Even so, this novel study revealed that the number of pulses of ESWT did not affect the improvements in hamstring spasticity in children with spastic type CP. The results showed that there were no significant differences between 500 pulses, 1,000 pulses, 1,500 pulses, and 2,000 pulses in reducing hamstring spasticity up to four weeks post-treatment. Further studies with larger samples, longer follow-up durations, as well as targeting different muscle groups are essential to substantiate the findings of this study. Other studies focusing on the effect of other physical parameters of ESWT such as energy flux density and repetition frequency should also be conducted to understand potential effect on spasticity improvement in CP patients.
Conclusion
On the basis of the results in this study, it could not be concluded that ESWT is a safe and non-invasive treatment for spasticity in children with CP. A session with an energy flux density of 0.1 mJ/mm2, a repetition frequency of 4 Hz and a pressure of 1.5 bars is tolerable to CP children. Even though this study suggests that total number of pulses may not have an effect on spasticity improvement, it is important to consider the small sample size and initial heterogeneity of groups being compared which would mean that the former statement is not definitively proved. Nonetheless, ESWT can be a treatment of choice for CP patients especially in developing countries such as Indonesia, where botulinum toxin injection treatment is not covered by Indonesia’s National Health Insurance. Further investigations are required to clarify the exact mechanism of ESWT in the treatment of spasticity, the right protocol of ESWT in CP and the duration of effect of ESWT.
Footnotes
Acknowledgments
The authors would like to thank all the study participants whose data contributed to this study. R.K.W. wishes acknowledge PT. Bold Technologies Leading Indonesia for sponsoring BTL-6000 SWT Topline.
Conflict of interest
The authors have no conflict of interest to report.