
Abstract
In clinical practice, intrathecal baclofen (ITB) therapy is used to control spasticity. After initial placement of the ITB pump, clinicians incrementally increase the dose until effectiveness in alleviating spasms and spasticity is optimized. However, this case describes a 4-year-old male with Leigh syndrome who developed a paradoxical worsening of spasticity and pain with incremental increase of his ITB pump. In this rare genetic disease with a poor prognosis, an ITB pump was trialed and implanted and titrated upwards with initial improvement. However, his spasticity and pain then began to worsen with each dosage increase. Subsequently, his symptoms improved significantly when the dose was weaned. This is the first case that describes this paradoxical reaction in a pediatric population and discusses recommendations about how clinicians should safely titrate the pump for patient care.
Introduction
Leigh syndrome is a rare but severe neurological disease that presents in early infancy with progressive loss of cognitive and physical abilities. There are many different enzyme defects that can cause this devastating syndrome and the majority are inherited in an autosomal recessive pattern [1]. Patients may initially have vomiting, diarrhea, and dysphagia and then develop hypotonia that progresses to spasticity [1]. Spasticity is reported using the modified Ashworth Scale (MAS), a qualitative assessment that goes from 0 (reflecting no increase in tone) to 4 (a rigid limb with all affected parts kept in flexion or extension). Generalized spasticity can be managed by oral medications such as baclofen, tizanidine, dantrolene, or benzodiazepines while focal spasticity can improve with localized neurolytic and/or chemo denervation injections.
When oral medications or chemo denervation agents are not effective in controlling spasticity and pain, surgical options may be considered. These include intrathecal baclofen (ITB) pump placement, deep brain stimulation, or selective dorsal rhizotomy. In this report, we discuss the treatment of a young male patient with Leigh syndrome. Given his diagnosis and clinical course he was deemed to be most appropriate for an ITB pump. After a trial of ITB and subsequent pump implantation, the dose is titrated upwards slowly to achieve appropriate spasticity control. However, as outlined in this case study, a rare and unusual phenomenon can occur whereby increasing ITB dosage results in paradoxical worsening of spasticity. This phenomenon was first reported in a case report by Cooper and Ridley who described two adult patients, one with a TBI with spastic hemiplegia and the second with a C5-6 spastic tetraplegia, where significant reductions in the dose of ITB led to improved spasticity [3].
Case description
This is a four-year-old male with a diagnosis of Leigh syndrome that resulted from an X-linked dominant pathogenic variant in the PDHA1 gene resulting in pyruvate dehydrogenase deficiency, that caused neurologic impairment and resultant spasticity of his bilateral lower extremities as well as left upper extremity. Initially, he was treated with oral baclofen 10 mg three times a day and diazepam 5 mg every 8 hours and received chemo denervation injections to his most affected extremities without relief. Given the progressive nature of his disease and the worsening of his spasticity, the plan for an ITB pump was established. Following implantation, he was admitted to the inpatient rehabilitation unit for titration of the pump dose.
Initially the pump dose was programmed to a rate of 50 mcg/day via continuous infusion. The pump dose was increased to a rate of 150 mcg/day and his oral diazepam need decreased with marked improvements. Over the following several days, the pump dose was incrementally increased to a total daily dose of 425 mcg/day with further improvement in spasticity control and enteral baclofen was discontinued.
However, when the ITB pump dose was increased to 675 mcg/day over the span of a week, his spasticity began to worsen. This was corroborated by an increase in MAS scores from 2 to 4 in physician documentation. External and secondary causes of spasticity were evaluated including infection, constipation, injury, and acute exacerbation of his metabolic disorder. At the time, there was no other change to his medication regimen. His therapists noted increased frequency and severity of spontaneous spasms and loss of head control, which was followed by excruciating and inconsolable pain. Dystonia and neuropathic pain were not believed to be contributing at this time due to visible spontaneous spasms and pain only during active spasms. Given the course and lack of external causes for worsened spasticity, it was hypothesized that he might have been showing signs of paradoxical reaction due to a narrow therapeutic range of ITB. He was re-admitted to the hospital for close monitoring and safe de-escalation of the baclofen. His pump and catheter were interrogated and evaluated and revealed no abnormalities. He was managed with scheduled morphine orally 3.75 mg every 4 hours, clonidine 0.2 mg daily, diazepam 6 mg every 4 hours, as needed midazolam 1.5 mg up to every 2 hours, and as needed IV morphine 2 mg up to every 2 hours. In addition, his pump was decreased by 50 mcg every 12 hours. Over the course of the several days, he stabilized at 450 mcg/day. Throughout this process, his therapists also noted consistent improvement in range of motion, head control, and tolerance of activity. Figures 1 and 2 showcase the correlation between his clinical progression in pain and spasticity with ITB therapy. Pain was monitored via the 0–10 pain visual analog scale (VAS) with 10 being the worst pain.
ITB dosing and pain.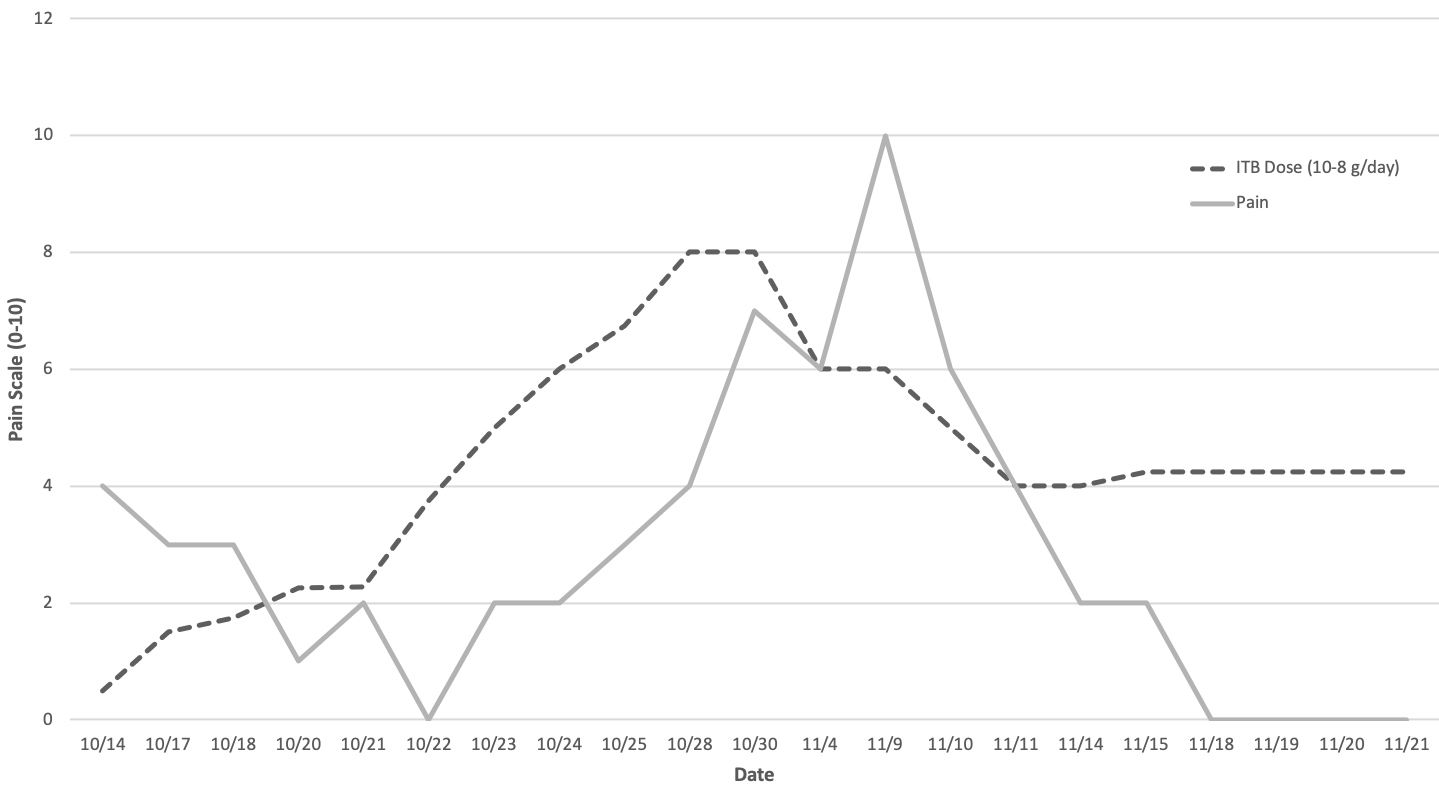
ITB dosing and spasticity.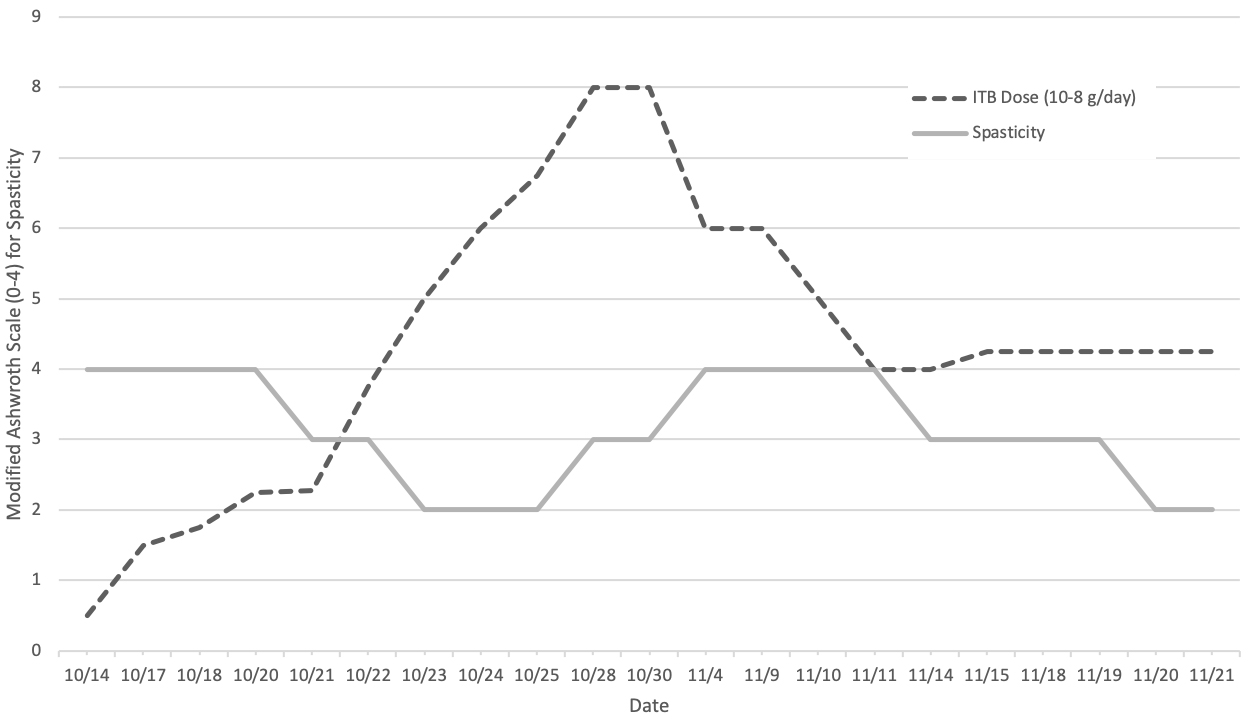
At our institution, the VAS is used to assess pain. While there are concerns with the reliability of the VAS score in patients less than five years old with no underlying co-morbidities [4], the VAS was used alongside nursing and daily physician documentation which led us to believe this was a true change in pain. As his ITB dose was increased from 375 mcg/day to 800 mcg/day, there was more pain noted on nursing assessments with reported pain scores gradually worsening from 0 up to 10. His pain was scored at a 10 and his spasticity worsened from a 2 to a 4 when his ITB dose was increased to 600 to 800 mcg/day. Many other types of pain and movement disorders were considered during this time but the only successful treatment for the worsening of his condition was ultimately a decrease in intrathecal dosing. Once the dose was adjusted and shifted to 425 mcg/day, his pain came down to 2 and later to a 0 and his spasticity improved to MAS 2. Shortly after he was discharged two weeks later, his sleep patterns stabilized and he was sleeping through the night and feeling refreshed for the day. He was discharged on 425 mcg/day of baclofen with significantly improved spasticity, manageable pain, and improved sleep. Additionally, he was discharged on 4 mg diazepam every 6 hours and 3.75 mg of morphine every 4 hours as needed for pain control.
ITB dosage is slowly and incrementally increased every 24 hours until the desired clinical effect is observed. Based on best practices for ITB, the daily dose increases for children ranges from 5–15% once every 24 hours [2]. Paradoxical reactions causing worsening spasticity with increasing ITB dose are a rare phenomena. There have been reported cases of this reaction seen in the adult population, but previously not observed in pediatric patients. Cooper and Ridley first reported a case in 2006 where a patient with spastic hemiplegia secondary to a TBI showed improved spasticity with a 70% reduction in ITB dose from 1000 mcg/day to 300 mcg/day. They also described a second patient with a C5-6 spinal cord injury with spastic tetraplegia who presented with worsening spasticity after an increase in his pump from 185 mcg/day to 500 mcg/day. This patient had resolution of his truncal flexor spasms with reduction of the pump dose from 500 mcg to 100 mcg/day [3]. After this initial case report, another case report emerged in 2012. Murakami and Hirata described an elderly patient with a traumatic brain and spinal cord injury who suffered from spasticity in his lumbar spine and bilateral lower extremities resulting from ossification of the posterior longitudinal ligament, spinal canal stenosis, and cerebral infarction [5]. They found that a 50% ITB dosage reduction from 40 mcg to 20 mcg led to resolution of spasticity in his lower extremities. Though 20 mcg/day is not considered an efficacious or therapeutic dose [2], this particular patient developed myoclonic-like involuntary movements of bilateral lower extremities with the ITB screening test dose of 50 mcg. This change improved when the dose was decreased to 12.5 mcg and thereafter, he was maintained on 20 mcg/day.
Cooper and Ridley have postulated that with prolonged exposure to ITB, gamma aminobutyric acid (GABA)
There are several possible causes of the paradoxical effect of increased pain and spasticity observed in our patient. He was not rapidly weaned off his oral medications of baclofen, morphine, and diazepam which could have precipitated a reaction of worsening pain and spasticity. Also, there was no introduction of new medications that could offset the effects of his regimen. However, perhaps there could be an underlying biochemical change affecting the patient’s response. Glutamate receptors, such as N-methyl-d-aspartic acid (NMDA) receptors, receive excitatory signals that are sent to the brain via the spinal cord to enhance certain experiences like pain [8]. Contrarily, inhibitory signals are mediated by the GABA receptors. The interactions and modulations between these differing neurotransmitters have been well documented in animal studies. For example, there is communication between the expression of NMDA and GABA receptors in terms of diabetic neuropathy where NMDA receptors are increased in the dorsal horn of the spinal cord and GABA receptors are downregulated [9]. Earlier on, there could have been similar changes in our patient with the interplay between more NMDA excitation and less GABA inhibition which caused him to experience more pain and agitation. He did have an increase in pain a few days preceding the change in spasticity. Subsequently, there may have been a shift to offset this and increase the GABA inhibitory neurotransmitters to lessen the pain and spasticity. Whether this is what happened for this patient is difficult to determine. Biochemical studies and assays would be needed to see the change in receptor expression during the clinical paradoxical reaction to demonstrate and verify this idea.
The Naranjo scale was used to determine the likelihood that an adverse drug reaction is indeed due to baclofen use. The scale creates an algorithm that ranks the score into categories of definite, probable, possible, or doubtful drug reaction due to a drug [10]. The 4-year-old patient scored a 7, meaning that this paradoxical reaction to baclofen was a probable result of increased baclofen doses. Based on the scale, he received a point for his responses regarding the following: previously reported reaction, the adverse event appeared after the ITB was administered, alternative causes such as pump or catheter failure were ruled out, the reaction became more severe with dosage increases and less severe when reduced, and the adverse event was confirmed by objective evidence. His symptoms worsened with increased baclofen dosing, which improved once the dose was decreased. However, re-introduction of baclofen at a higher ITB dose as a means to demonstrate the paradoxical effect did not occur given our patient’s age and risk of placing him in further discomfort again. Therefore, taking these points in consideration, it is likely that ITB caused the observed paradoxical reaction.
Conclusion
Leigh syndrome is a rare genetic disorder resulting in spasticity and pain in afflicted patients which can be hard to manage and may ultimately need more advanced therapeutic options including an ITB pump. This case report describes an uncommon paradoxical reaction to increasing ITB dosing causing worsening spasticity. Clinicians need to be aware of this detrimental reaction in order to provide safe and effective care to patients and prevent worse overall outcomes and functionality.
Footnotes
Conflict of interest
The authors have no conflict of interest to report.