
Abstract
PURPOSE:
This study explores non-motor impairment of the upper dominant limb in children with diplegic cerebral palsy (CP). Specifically, it firstly investigates sense of position without visual control, ability to compare visual and proprioceptive information, and capacity to recognize effects of self-movement. Secondly, it explores the possible association between these items with cognitive function, perceptual disorder (PD), and manual ability (Manual Ability Classification System -MACS).
METHODS:
Ten subjects (7 female; 3 male) were tested with three protocols: the first one (A) explored sense of position, the second one (B) collimation between visual and proprioceptive information, and the last one (C) sense of agency with the use of videogames.
RESULTS:
All subjects executed Protocol A without making any mistakes, while in Protocol B the median percentage of mistakes was 4.8%. Mistakes were recorded more frequently in positions characterized by wrist extension. Data reported a significant correlation with Processing Speed Index (PSI). Sense of agency was positively associated with cognitive functioning, with a significant correlation with PSI.
PD, MACS, and Video-Gaming Experience (VGE) showed no correlation with Protocol C.
CONCLUSION:
In the observed sample with diplegic CP, preliminary data support the hypothesis that there is an alteration of both sense of position and sense of agency. They were both associated to PSI, with a positive trend of correlation with cognitive functioning. PD seemed to have no influence. Further studies, with a larger sample size, a control group, and involving children without CP, are required to corroborate the results obtained.
Introduction
Cerebral palsy (CP) is a permanent disorder produced by a brain injury occurring during pregnancy, at birth or shortly after birth, which causes a fixed encephalopathy. It represents the principle cause of childhood physical disability in industrialized societies (1/500 live births) [1]. Since CP affects the most sensitive period of development in humans, it is considered a neurodevelopmental disorder [2]. CP signs and symptoms are numerous and typically consist of motor impairment, poor coordination, spasticity, seizures, mental deficiency, and disturbances affecting perception, vision, hearing, swallowing and speaking [2, 3]. In recent years, the importance of non-motor CP signs and symptoms has been recognized, and several authors have underlined the role of cognitive impairment and perceptive alteration in influencing motor control and recovery possibilities [1, 3].
The ideo-motor model, proposed by Ferrari [4] and shown in Fig. 1, helps to explain the relationship between disorders of posture and movement (position and gesture) and sensory and perceptive disturbances, deficits or alterations in cognition, communication, and behavior.
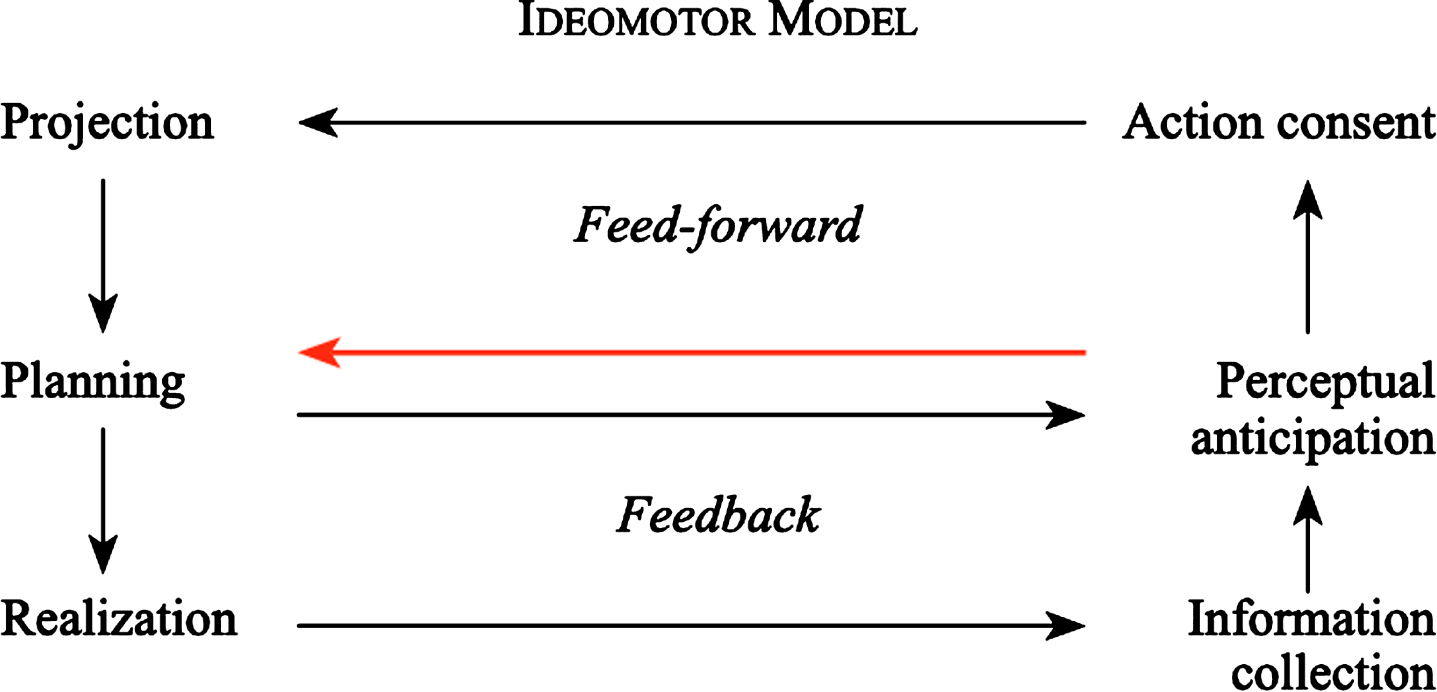
The ideo-motor model (with author’s permission) [4].
This model proposes a guide to understanding which kinds of errors a child with CP can exhibit: 1) projection (which includes motivation, ideation and programming of movement), 2) planning (praxia), 3) realization, 4) perceptual anticipation, 5) action consent, and 6) information collection and comparison.
This study focuses on the last three errors. Berthoz [5] talks about anticipatory configuration, a sort of internal anticipation and simulation of the results of an action before its execution. Then, the conceived, programmed, and planned action can be executed only if the central nervous system (CNS) gives the “action consent.” Once consent is given, the action execution will be performed, generating a series of information, which should be collected, compared and integrated into perception to create mental representation and memories [4] (Fig. 2).
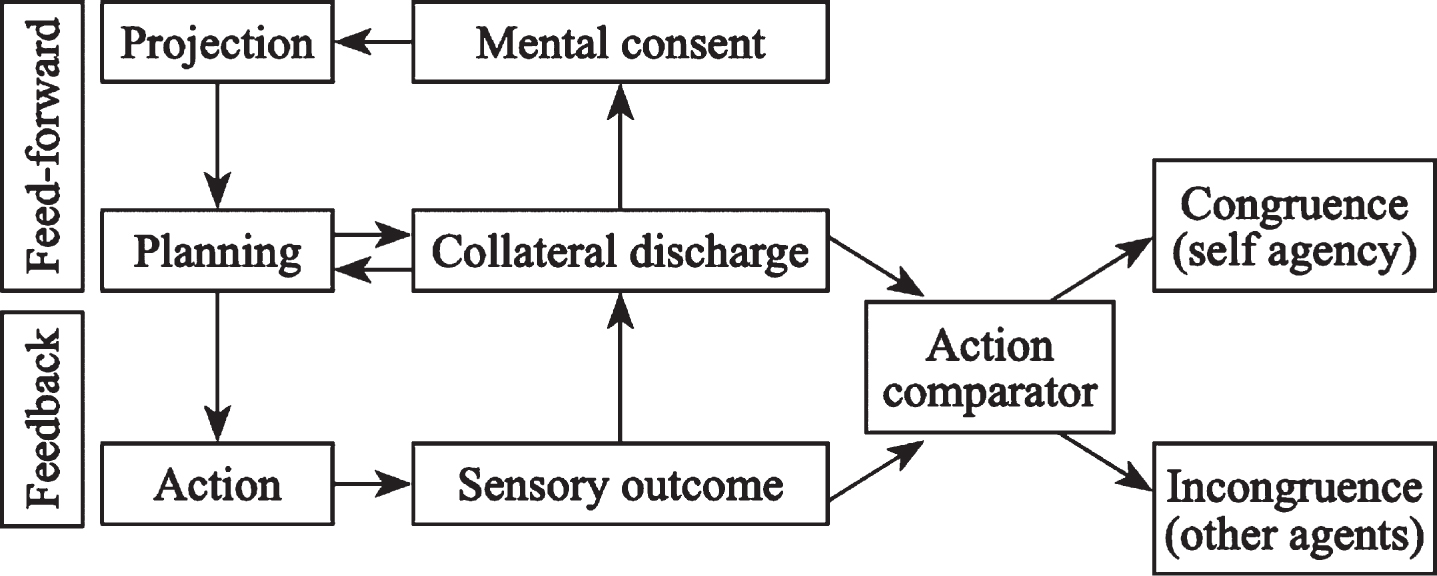
Action comparator (with author’s permission) [4].
Subjects with a perceptual disorder (PD) can have an altered emotional map, probably correlated to connections between the amygdala, sensorial areas and other regions of the CNS. As in panic disturbance, the PD can stop the action consent [6].
Some authors underline the discrepancy between motor repertoire and its functional use in CP, especially in the diplegic forms. For example, given the same Gross Motor Function Measure (GMFM), not all diplegic patients achieve the equivalent performance and autonomy and therefore the corresponding participation [6–8]. This discrepancy can be explained by the presence of a PD. PD in CP is the failure of a complex neurological process that enables the individual to collect, integrate, interpret and use the spatial-temporal aspects of sensory information from the body and the environment, to plan, control, guide and produce organized motor behavior. In other words, PD is a cognitive–perceptual–motor dysfunction that entails the inability to adapt and to integrate environmental experiences [6].
PD is defined by Ferrari et al. [9] as the combination of at least three of six clinical signs. The influence of PD on motor control is already described. A study conducted by Ferrari and colleagues shows that children with diplegic CP with PD have an anticipatory postural control and a different organization of the walking function, compared to children with CP without PD [10].
On the other hand, there is a lack of literature re-garding the description of the possible influence of the PD on the organization of the manipulative function.
Ritterband-Rosenbaum defines sense of agency as the ability to recognize the proper agent of a particular movement [11]. Ferrari’s ideo-motor model is also defined as the ability to compare the perceptual anticipation of the projected and planned action to the actual collected sensory information [4].
The sense of agency intervenes during the collection of information after carrying out an action, which must be compared with what had been imagined during perceptual anticipation.
In children with CP, a poor integration between intention of movement and visual and proprioceptive information related to the performed action can represent an important functional disorder (Fig. 2) [4]. In the Ritterband-Rosenbaum study from 2011, three groups (children with hemiplegic CP, healthy peers, and healthy adults) were compared while producing straight drawing movements on a pen-tablet that was not visible to the subjects [11].
The study explored the ability of participants to determine whether the movement of a virtual moving object is caused by themselves or by external sources, concluding that this ability is reduced in children with CP.
This suggests a poor integration of their intention of movement with visual and proprioceptive information about the performed movement [11]. The hypothesis is that an altered sense of agency may be relevant to the functional problem and may explain part of the above-mentioned discrepancy [12]. At present, few studies have analyzed this topic and this work represents an exploration of how to examine these issues.
This study aims to analyze sense of position without visual control; the ability to compare visual and proprioceptive information; the capacity to recognize the effects of self-movement (sense of agency); and, if incorrect, to adjust.
The secondary objective of this study is to inves-tigate the possible association between the above-mentioned abilities and Intelligence Quotient (IQ) [13], Processing Speed Index (PSI) [14], Working Memory Index (WMI) [15], PD, and Video-Gaming Experience (VGE) to explore the possible influence of cognitive functions on the sense of position and agency and collect preliminary data on cognitive domains involved and levels of competence required. IQ is the most useful evaluation of cognitive abilities, and it is the most reliable tool to describe the general cognitive functioning of each subject13.
PSI is a measure of the ability to quickly perform easy and repetitive tasks of a visual-motor nature. It is an index of the ability to pay attention, visually scan, discriminate and store simple visual stimuli in the short-term memory13. The index subtests cannot be considered as detectors of reaction times or the ability of visual discrimination.
WMI is a measure of short-term and working verbal memory skills and focused and sustained attention skills. It measures, categorizes or assesses the stored information for a short period of time, which allows this information to be quickly accessible to be then transformed based on rules and strategies. This allows the information itself to be continuously updated. It presupposes the existence of two processes: the registration and the mental manipulation of stimuli [15].
The patients were enrolled from inpatient or outpatient services of the Pediatric department of IRCCS Fondazione Don Gnocchi of Florence.
The study was approved by the Ethics Committee of Area Vasta Centro of Tuscany Region. Written informed consent was obtained from all subjects and their parents.
Inclusion criteria
Patient affected by spastic diplegic CP (clinically and MRI defined); Aged 10 –18 years; Able to perform, with both upper limbs, the movements required in the three protocols (closing/opening of the 5 fingers, closing/opening the first finger in isolation, wrist flexion/extension, forearm pronation/supination, and elbow flexion/extension) as assessed by a clinician. The movement was considered proper if possible around the neutral position, regardless of Range of Motion (ROM) measurement.
Exclusion criteria
Previous multilevel upper limb surgery; Botulinum toxin injection in the upper limb in the previous 6 months; Central visual impairment that could hinder playing videogames.
Each patient received a neuropsychological evaluation to assess IQ, PSI and WMI through the Wechsler Intelligence Scale for Children –Fourth Edition (WISC IV) [13].
Video game experience was investigated by a graduated scale from 0 (no experience) to 10 (great exp-erience).
For each patient, the presence of PD [10], diplegia form according to Ferrari [16, 17], as well as manipulation ability through the Manual Ability Classification System (MACS) [18] were assessed.
Sample group features
The sample group included ten subjects (7 females/3 males, 6 right-handed) with a mean age of 15 years, ranging from 11 to 18 years.
Concerning diplegia classification, according to Ferrari [17], four subjects were given form I, two were given form II and four were given form III. Table 1 reports subject distribution on the basis of GMFM level.
Subject distribution for Gross Motor Function Measure (GMFM) Level
Subject distribution for Gross Motor Function Measure (GMFM) Level
To simplify the analysis of neuropsychological data, continuous variables of IQ, PSI, and WMI were converted into categories. Table 2 describes subject distribution in terms of IQ, PSI, WMI and MACS ranks, and the presence/absence of PD.
Subject distribution for IQ (Intelligence Quotient), PSI (Processing Speed Index), WMI (Working Memory Index), MACS (Manual Ability Classification System), and PD (Perceptual Disorder)
Protocols A and B explored the ability to detect and reproduce the position of the upper limb compared to the contralateral limb and to the limb of another subject.
The positions adopted in the two protocols are shown in Fig. 3. For Protocol A, the positions of photos 5, 9, and 10 were used; for Protocol B, all the positions shown in the figure were used as described in the figure’s caption.
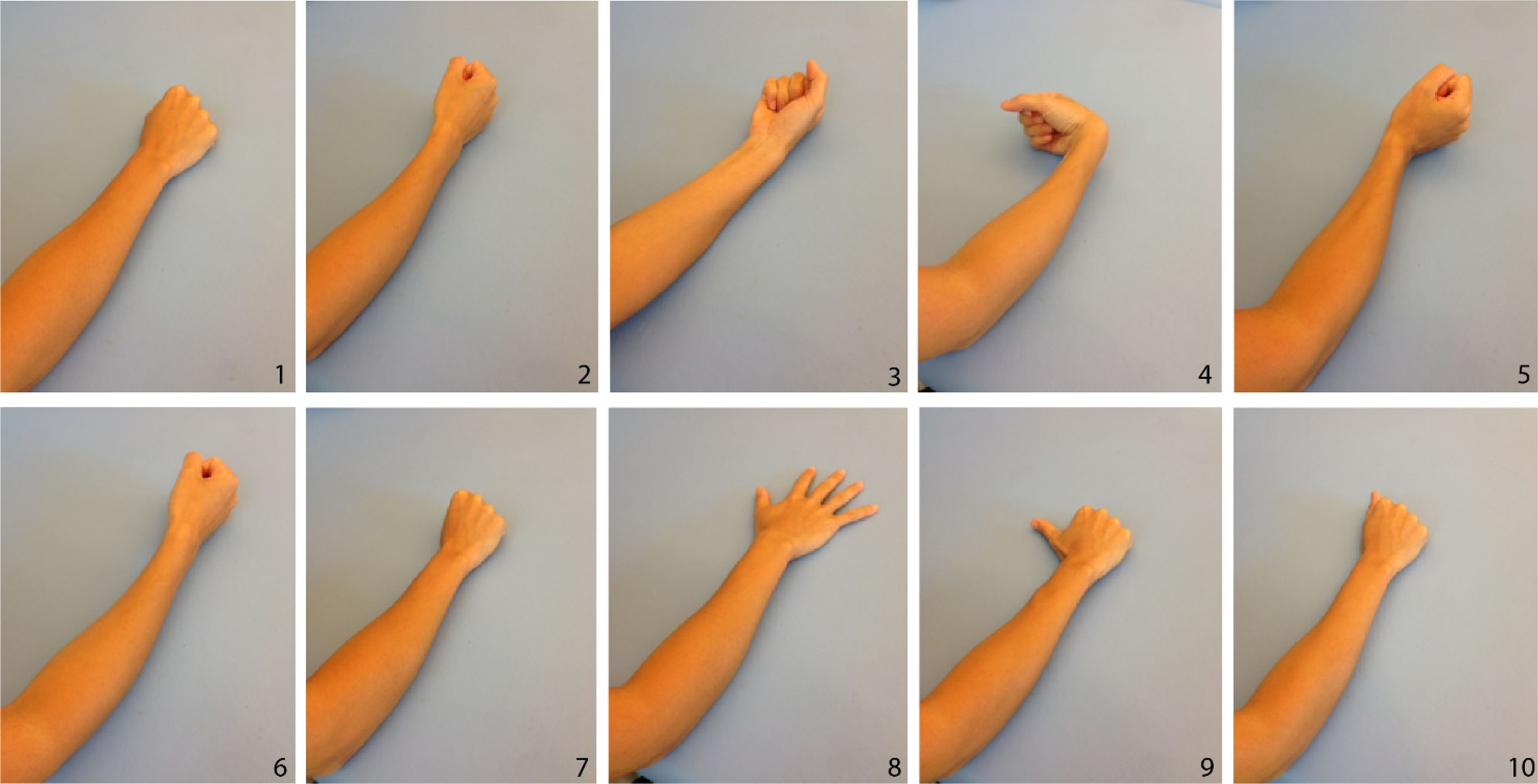
Pictures used to show the patient the 21 positions included in Protocol B. Photo 1 was used to show position 1 (patient’s upper limb was placed in the same position) and position 4 (patient’s upper limb was placed in the same position but with supinated forearm). Photo 2 was used to show position 2 (patient’s upper limb was placed in the same position) and 6 (patient’s upper limb was placed in the same position but with supinated forearm). Photo 3 was used to show position 3 (patient’s upper limb was placed in the same position) and 5 (patient’s upper limb was placed in the same position but with pronated forearm). Photo 4 was used to show position 7 (patient’s upper limb was placed in the same position) and 10 (patient’s upper limb was placed in the same position but with extended wrist). Photo 5 was used to show position 8 (patient’s upper limb was placed in the same position) and 11 (patient’s upper limb was placed in the same position but with flexed wrist). Photo 6 was used to show position 9 (patient’s upper limb was placed in the same position), 12 (patient’s upper limb was placed in the same position but with flexed wrist) and 13 (patient’s upper limb was placed in the same position but with extended wrist). Photo 7 was used to show position 14 (patient’s upper limb was placed in the same position) and 17 (patient’s upper limb was placed in the same position but with open hand). Photo 8 was used to show position 15 (patient’s upper limb was placed in the same position) and 16 (patient’s upper limb was placed in the same position but with fist clenched). Photo 9 was used to show position 18 (patient’s upper limb was placed in the same position) and 21 (patient’s upper limb was placed in the same position but with adduced thumb). Photo 10 was used to show position 19 (patient’s upper limb was placed in the same position) and 20 (patient’s upper limb was placed in the same position but with abducted thumb).
According to a qualitative criterion, wrong position (WP) was defined as the different positioning or direction of at least one of the joints compared to the reference position proposed in the two protocols, regardless of ROM.
Protocol A examined the patient’s ability to recognize and reproduce various positions of forearm, wrist and hand/fingers. The therapist placed the patient’s dominant (least impaired) upper limb in different combinations of positions of forearm, wrist and hand/fingers, and then asked the patient to replicate the analogous position with the other hand without any visual control. For each patient, the therapist recorded the number of WPs in an appropriate sheet.
Protocol B explored the patient’s ability to recognize imposed positions of forearm, wrist and hand/ fingers of the dominant upper limb. The therapist showed the patient a picture of an upper limb with a combination of positions of the forearm, wrist and hand/fingers (Fig. 3) and placed the patient’s dominant upper limb in a specific combination of positions of the forearm, wrist and hand/fingers. Then the therapist asked the patient whether the position of their upper limb matched the one shown in the picture. Patients were not allowed to look at their upper limb, which was hidden under the table. The positions of the forearm, wrist and hand/fingers were pre-established and consisted of 21 different combinations. Pictures were specifically made for right- and left-handed patients. For each patient, the therapist recorded in an appropriate sheet the number of WPs.
Protocol C explored the patient’s sense of agency. It investigated the patients’ ability to recognize themselves as the actors of movement, to recognize the consequences of their movements, and, if incorrect, to adjust them. The therapist submitted three videogames performed using Pablo® version 4.2 (Tyromotion GmbH, Graz, Austria) with two different controllers: multiboard and joystick. Each game featured a preliminary calibration phase to enable the patient to use the controller in compliance with ROM and personal abilities. This allowed every target to be reachable over the entire game field in any direction (up and down, left and right).
Game 1: The patient was positioned on the multiboard as shown in Fig. 4. The game consisted of picking apples falling from trees through a trunk inclination movement.
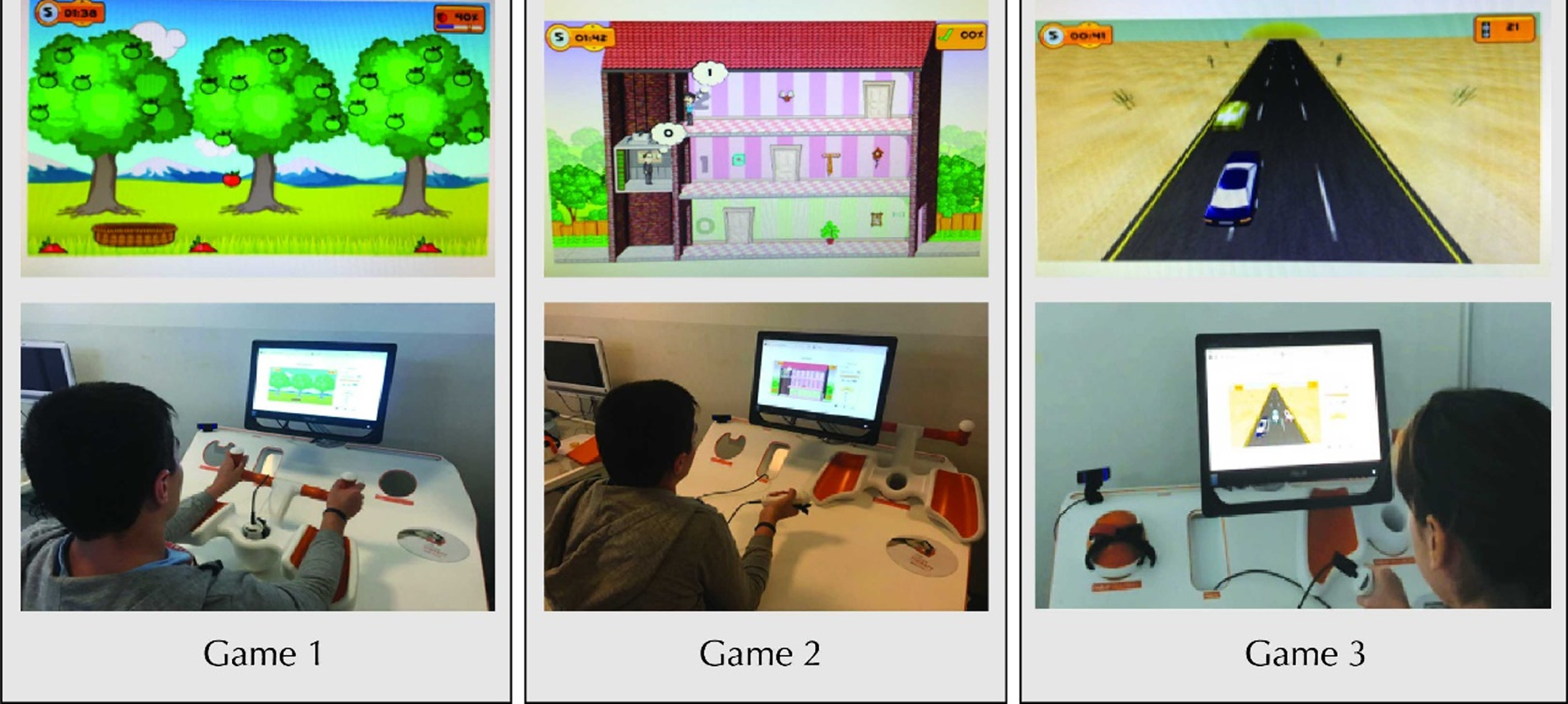
The three games used to evaluate sense of agency.
Game 2: The patient used the joystick and was asked to flex/extend the elbow to guide an elevator up and down while keeping the forearm in a neutral position.
Game 3: The patient used the joystick and was asked to drive a car along a road avoiding other cars through a movement of forearm supination and pronation.
The level of difficulty was the same for all subjects, set on the basis of the result of a previously tested convenience sample. Before beginning, the therapist made sure that the subjects understood the tasks and movements they were asked to perform. Each game lasted four minutes. In the first two minutes (phase 1 –P1), the videogames reproduced patient movements in a coherent way: the apple basket went to the right when the patient trunk tilted to the right and to the left when it tilted to the left; the elevator went upstairs when the patient’s elbow flexed and downstairs when it extended; using the right arm, the car went to the right when the patient’s forearm supinated and to the left when it pronated (using the left arm the car went to the left when the patient’s forearm supinated and to the right when it pronated). After 2 minutes, the therapist reversed the control mode without informing the patient (phase 2 –P2). Therefore, the apple basket went to the left when the patient’s trunk tilted to the right, the elevator went downstairs when the elbow extended, and the car went to the right when the forearm pronated (for the right arm).
Each performance was recorded on video.
In line with the game scoring proposed by the manufacturer (i.e., Game 1 recorded an apple falling out of the basket as a mistake), it was recorded whether tasks were properly executed or not (mistakes).
The number of mistakes made in P1 (mistakes-P1), in P2 (mistakes-P2), and the total number of mistakes (mistakes-TOT) for each game were recorded and expressed as a percentage [(number of errors/ number of tasks) *100].
The therapist also noted the patient’s verbal expressions. During P2 of each game, some patients became aware of the control reversal and informed the therapist; those were referred to as Aware Subjects (AS). Subjects that did not notice the control reversal were referred to as Not Aware Subjects (NAS).
During P2, some patients corrected their movement (CM) according to the reversal of control and maintained the correction over the entire test phase. Other patients did not correct their movements or corrected them casually (NCM), without maintaining the correction over time. The time required to correct movements was also recorded.
To avoid the learning bias, a single evaluation was made in all three protocols.
The VGE was recorded to verify possible interference on the performance.
Data were analyzed using SPSS software (IBM SPSS software version 25). The Spearman correlation coefficient was used to evaluate the association between the percentage of mistakes-TOT and in every sub-phase of each game with patient neuropsychological characteristics. The significance level of correlations was considered as follows; rs = 0.00–0.25, no/very weak correlation; rs = at least 0.35, weak correlation; rs = at least 0.60, moderate to strong correlation; rs = at least 0.75, strong correlation [19]. Differences in errors performed between AS and NAS were investigated using a Mann-Whitney test as the data distribution did not meet requirements for parametric comparisons. The level of significance was set at a p-value < 0.05.
A descriptive analysis was conducted to explore the existence of a trend between neuropsychological scores and the score of each game phase.
Results
All subjects executed Protocol A without making any mistakes.
The median percentage of sample mistakes performed in Protocol B was 4.8% (Inter Quartile Range 11.9%). Two subjects did not make any mistakes, five subjects failed 5% of the tasks, and the remaining three subjects failed, respectively, 14%, 19% and 29% of tasks. Positions characterized by wrist extension had the highest percentage of mistakes followed by the position of wrist flexion, as shown in Fig. 5.
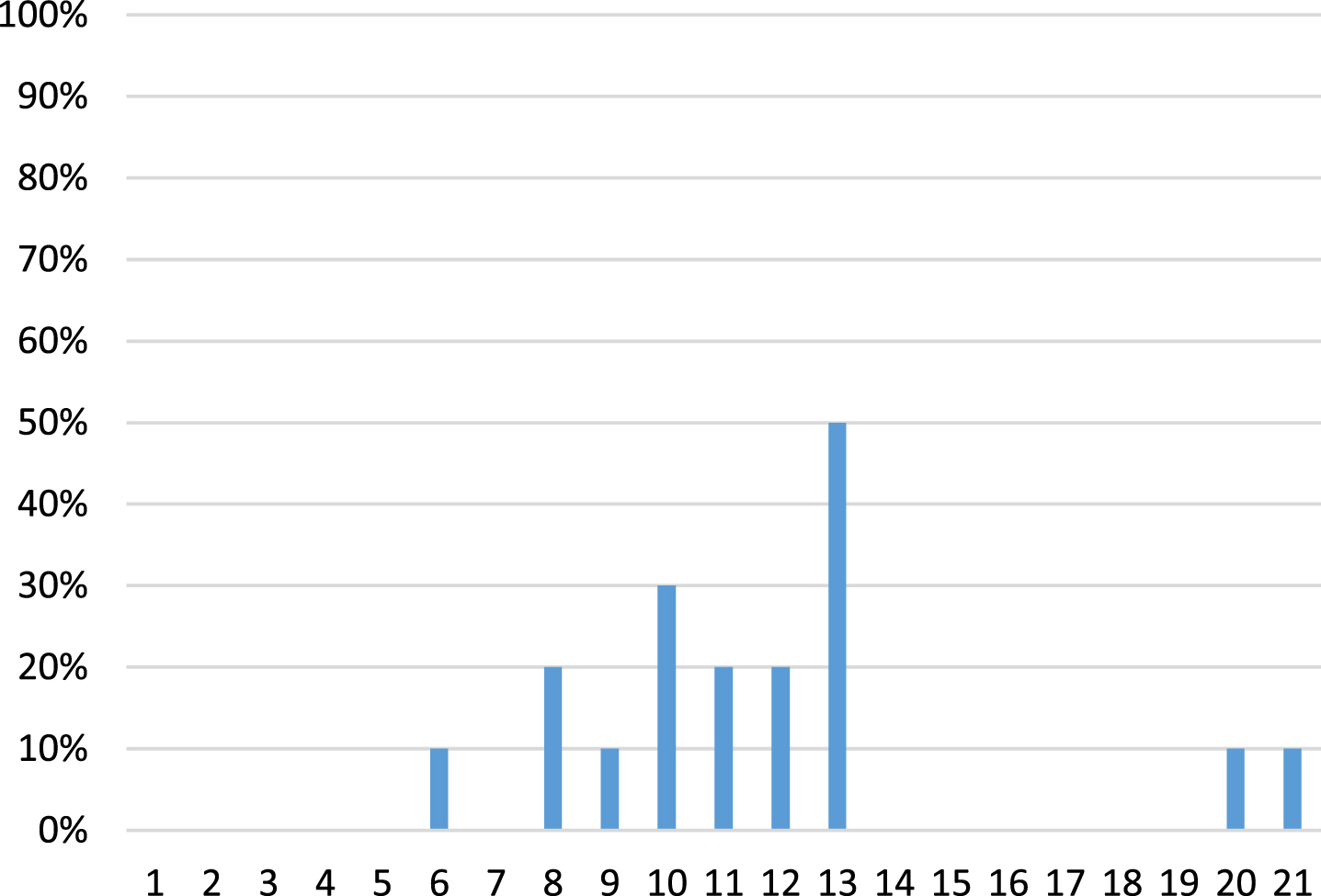
Percentage of mistake per position.
While being tested, 30% of subjects asked to look at or touch their arm to confirm the given answer.
In Protocol B, significantly fewer mistakes were recorded in the AS group compared to the NAS group (Table 3).
Comparison between mistake percentage performed by Aware Subjects (AS) and Not Aware Subjects (NAS) in Protocol B (referred to all positions) and in Protocol C
IQR: Interquartile range. *p < 0.05.
Table 4 shows correlation coefficients and levels of significance between percentage of mistakes and neuropsychological scores. No significant correlation was found between IQ and mistake percentage (p-value = 0.606, r = 0.186), while PSI and the reported mistake percentage were significantly and positively associated (p = 0.021) showing a good correlation (r = 0.711). WMI correlation with mistake percentage was not significant (p-value = 0.456, r = 0.267).
Spearman’s correlation coefficients and levels of significance between mistake percentage and neuropsychological scores
IQ: Intelligence Quotient; PSI: Processing Speed Index; WMI: Working Memory Index; VGE: video-gaming experience. *p < 0.05.
During the first phase of Games 1 and 3 in Protocol C, neither help from the therapist nor further instructions were required by the participants. On the contrary, 30% of subjects needed help in movements required in Game 2.
The following data were recorded:
Game 1: mistakes-P1 11%, mistakes-P2 23%, mis-takes-TOT 34%;
Game 2: mistakes-P1 18%, mistakes-P2 12%, mistakes-TOT 30%;
Game 3: mistakes-P1 2%, mistakes-P2 7%, mista-kes-TOT 9%.
Figure 6 shows the distribution of mistakes made in P2 concerning movement correction and awareness.
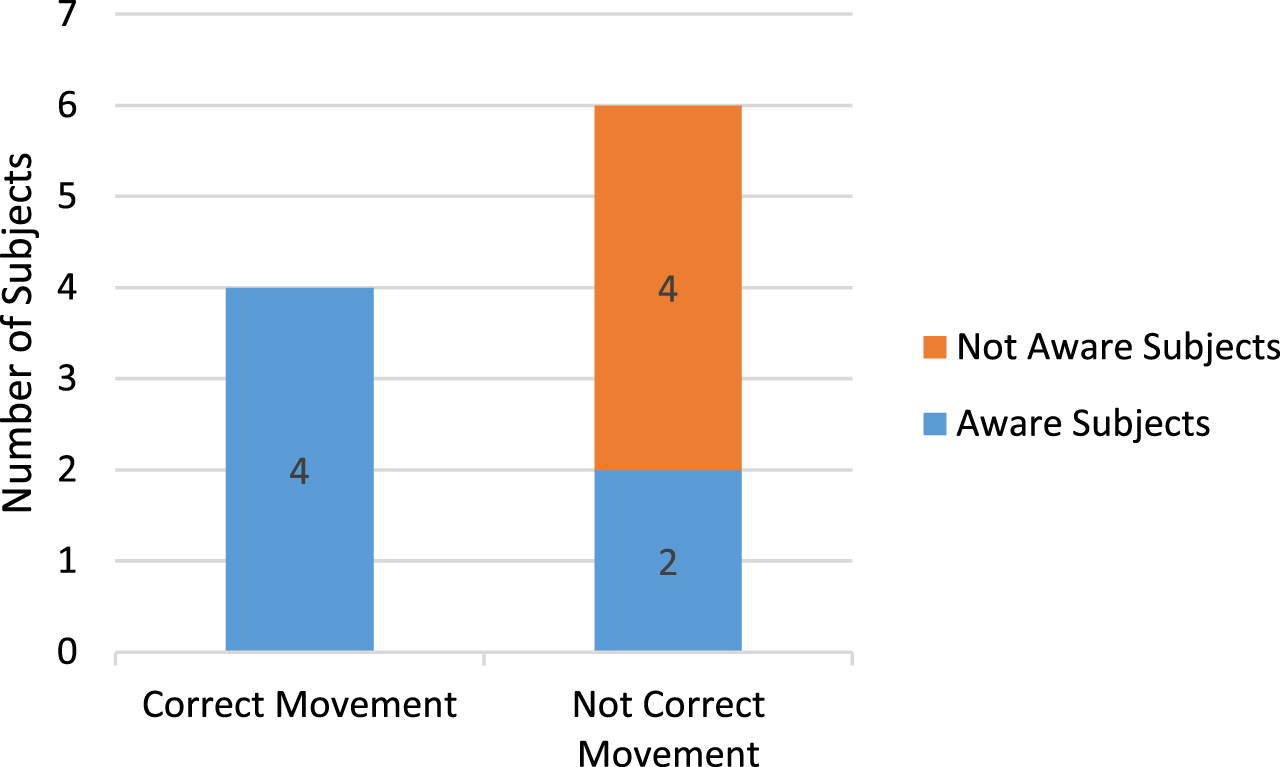
Distribution of Aware Subjects (AS) and Not Aware Subjects (NAS) in Correct Movement (CM) and Not Correct Movement (NCM) groups.
Figure 7 shows the trends between the percentage of mistakes in each phase of each game and neuropsychological scores.
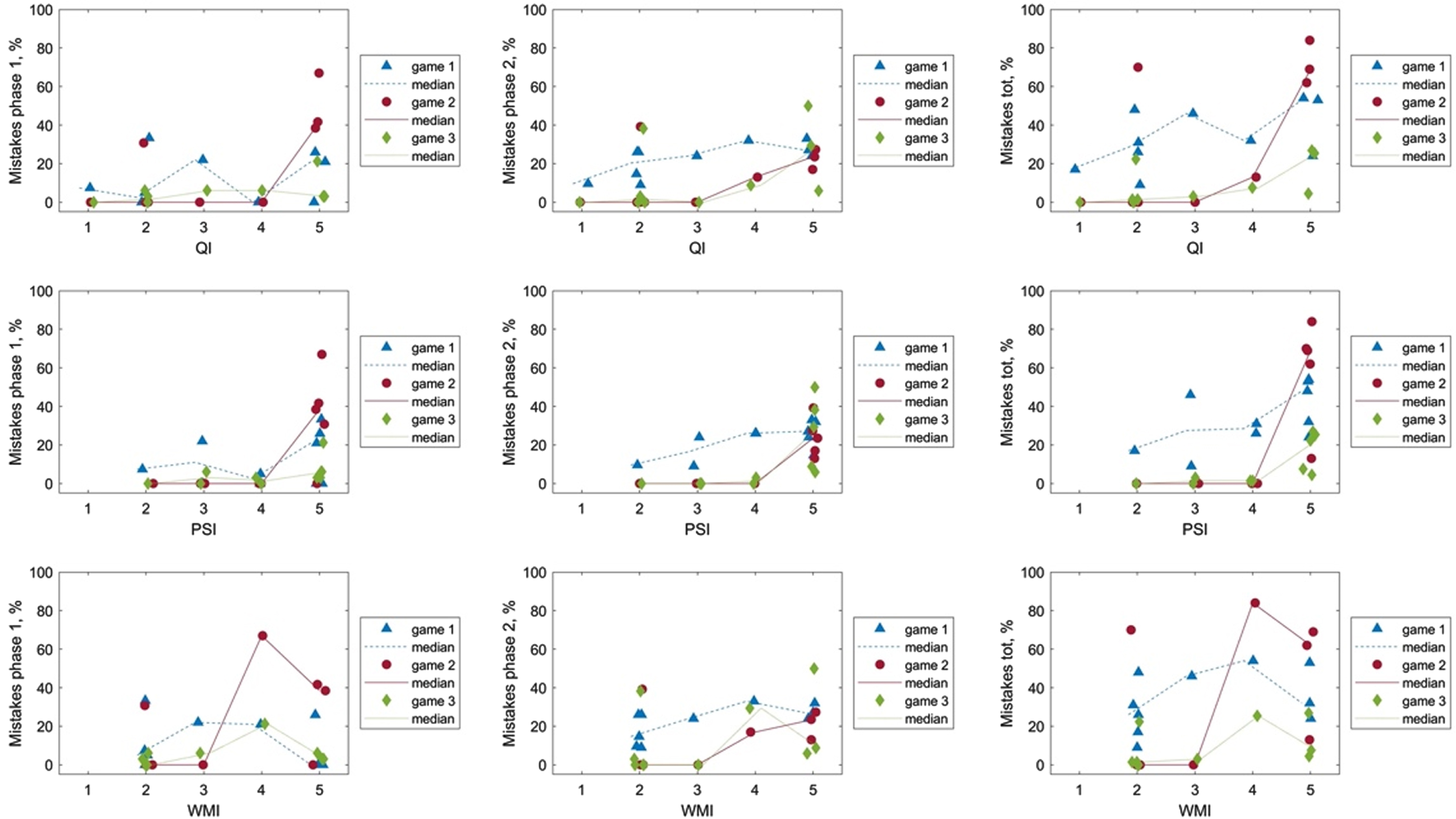
Neuropsychological score trend in each phase of each game.
In the group of patients with PD, three patients corrected their movements and four patients did not. In the group of patients without PD, one patient corrected their movements and two patients did not.
Evaluating the association between diplegia form and mistakes made in Protocols B and C, a trend in reducing mistakes-P1 from diplegia form I to diplegia form IV (r = –0.703, p value = 0.023) was observed. In other words, subjects belonging to diplegia III and IV made fewer mistakes than subjects belonging to diplegia I and II in P1 of Game 1.
The association between the percentage of mistakes for each phase of each game and MACS level was not significant (Table 5).
Spearman’s correlation coefficients and levels of significance between mistake percentage and manipulation scores
MACS: Manual Ability Classification System *p < 0.05.
The sample’s mean age (15 years) leads the authors to believe that sense of position and judgment of movement has already been acquired.
The mental representation of sense of position without visual control was well-preserved in this sample, as shown by the absence of mistakes in Protocol A. To the authors’ knowledge, standardized tests that specifically explore this item in CP are not yet described in the literature. Wingert et al. explored the sense of joint position but with a different task [20]. Results from this study are in line with Wingert’s findings, which describe a deficit in joint position sense without visual control in all limbs except for the dominant arm, in both hemiplegic and diplegic CP. It might be relevant that the protocol used in this study did not include a position with supinated forearm, flexed wrist, open hand, and adduced thumb as well as did not explore the sense of position of the non-dominant arm.
Protocol B explored the ability to compare visual and proprioceptive information. As shown in Table 3, this study group made a significant amount of mistakes in this task. A great part of the mistakes concerned wrist extension and in particular the ability to distinguish the extended position from an intermediate position between flexion and extension. This was probably caused by a poor cortical representation of the extended wrist. Patients with CP commonly resort to simplified wrist movements to facilitate finger activity, reduce ROM during spontaneous activities, and choose a position with flexed wrist to facilitate finger movements, also in order to comply with spastic tone of flexor muscles. Indeed, Mailleux et al demonstrated that a higher MACS level corresponds to a larger ROM of wrist flexion [21] while the correlation between supination and level of MACS was not investigated.
The significant correlation found between mistake percentage and PSI may suggest that the judgment of sense of position requires the ability to hold back simple visual stimuli, although for a very short time. Probably for this reason, some subjects asked to look at their arm. The engagement of major cognitive functions (IQ) did not seem to be required.
The observed significant difference between AS and NAS groups was probably due to the explicit request for a verbal response, which presupposes a certain grade of awareness.
Protocol C explored sense of agency. Results suggest that an alteration of sense of agency is recognizable, with a significant difference in the percentage of mistakes between the AS and NAS groups in P2.
Results on the association and trend between IQ and percentage of mistakes (Table 3 and Fig. 7) suggest that IQ influences the global performance in videogaming, without a significant difference between P1 and P2. In other words, higher levels of intelligence do not seem to be required to develop a reliable sense of agency. Since IQ explores major cortical functions, it can be hypothesized that intelligence and knowledge do not influence the sense of agency.
The significant association found between PSI and mistakes made in P2 in Games 2 and 3 suggests that the ability to compare the information belonging to planned action with information coming from the generated action could be attributable to the speed with which a subject receives visual and proprioceptive inputs and re-uses them to remodel the oculo-manual coordination task.
WMI showed a significant association with only mistakes-TOT in Game 3, with a positive trend in all three games; thus it did not seem to influence sense of agency.
These data suggest that the proper execution of a motor task requires subjects to pay attention to the effects of their movement which could lead to awareness. “Paying attention” in particular means the ability to process visual and proprioceptive information in an adequate and sufficient time.
The short duration of each game did not allow learning, excluding the influence of IQ.
A significant difference between AS and NAS in sense of position and correction of movement in P2 was found in Games 2 and 3. Looking at the distribution of AS and NAS in the CM and NCM groups (Fig. 6), it can be noticed that the whole CM group consisted of AS. No subjects corrected the movements without being aware of them; however, not all of the AS corrected their movement. It can be argued that the ability to collimate planned action information and the performed information needs patient attention, and this could lead to awareness that is not necessarily dependent on cognitive performance (IQ). It can be supposed that awareness is a necessary but not sufficient prerequisite to correct movement. From the data collected, it is not possible to draw further considerations about awareness, the degree of which is not quantifiable as the question posed to the subject (“Did you notice?”) provided only a binary answer (yes / no). There are likely different levels of awareness: a first level of awareness may therefore lead to recognizing non-collimation; the second may lead to recognizing the need of correction; the third may lead to correction itself.
The positive trend observed between IQ and percentage of mistakes needs to be confirmed in a larger sample and with respect to a control group.
Considering only permanent correction, the time required to correct movements was progressively shorter in Games 1, 2, and 3. In the CM group, a positive trend in reducing the percentage of mistakes in P2 from Game 1 to Game 3 was noticed. Game 3 had the lowest percentage of mistakes-P1, mistakes-P2, and mistakes-TOT compared to the other two games.
This was probably due to a progressive comprehension and learning of the command inversion and not to a different level of difficulty among the three games. Indeed, games were always played in the same order, which is a limitation of this study.
PD was recorded in both CM and NCM groups, suggesting that PD and sense of agency were not strictly related. This is in line with what is described in the ideo-motor model. In fact, PD refers to action consent or to a sort of “emotional” cortical map that could lead to disproportionate reaction (error type IV in ideo-motor model); once a subject receives the consent, the next step is to act, to collect the information generated (feedback loop), and to compare it with the planned action (feedforward loop) –sense of agency (VI type of error), as shown in Figs. 12.
Considering the association between diplegia form according to Ferrari classification [17] and mistakes in Protocols B and C, diplegia form did not seem to influence the mistake percentage.
The absence of correlation between VGE and mistake percentage in the three games suggests that the results were not affected by the use of videogames at home.
This study presents some limitations that could be addressed by future research. Protocol A employs a limited number of positions that could be increased to carry out a more sensitive search in the sense of position. Protocol B does not provide the assessment of forearm supination, which deserves to be investigated. In Protocol C, in the absence of games sequence randomization, it is not possible to establish whether the positive trend of mistakes is due to learning or to the type of movement required.
MACS distribution in the studied group was homogeneous, as shown in Table 2. This does not allow for evaluation of a possible correlation between sense of agency and manual ability. The diplegic classification used in this study was based on gait pattern; this could create a bias because patients belonging to the same group may not have the same manipulation pattern.
The main limit is the small sample size and the absence of a control group, which prevents any firm conclusions. For these reasons, other studies should further investigate sense of agency using a larger sample and exploring possible correlation with IQ, PSI and WMI in patients without CP.
To conclude, this study demonstrates the importance of exploring sense of position and sense of agency in children with CP. These preliminary data support the idea that there is an alteration of both sense of position and sense of agency, and that they are both closely related to the ability to collect and maintain visual and proprioceptive information properly and fast enough. Given the possible correlation with the PSI, it might be useful to explore the association with some sub-tests of the PSI (e.g., coding score, which measures visual-motor dexterity, associative non-verbal memory, and non-verbal short-term memory). The probable absence of correlation with IQ and WMI supports the idea that sense of agency requires neither “intelligence” nor the maintenance of information in memory circuits.
Further studies exploring sense of position and sense of agency in subjects without CP with IQ, PSI and WMI are required in order to understand whether or not these characteristics are typical of CP.
It would be interesting to assess the evolution of sense of agency from early childhood to adolescence. This study suggests that disorders related to sense of agency can be explored though videogames; more complex applications can be elaborated, for example by the use of an “avatar”.
Footnotes
Acknowledgments
The authors thank all the children and their parents for their voluntary study participation.
Conflict of interest
We declare no conflict of interest.
Funding
This study was funded by “Ricerca Corrente” Funds from the Italian Ministry of Health.