
Abstract
PURPOSE:
Young adults with transversal upper limb reduction deficiency experience limitations regarding education, employment and obtaining a driver’s license. Contribution of rehabilitation care within these domains has been reported to be inadequate. This study evaluates the needs and suggestions of participants in rehabilitation care.
METHODS:
Two online focus groups with young adults and parents met during 4 consecutive days. Health care professionals joined a face-to-face focus group. Data analysis was based on framework analysis.
RESULTS:
The rehabilitation team was mainly consulted for problems with residual limb or for prostheses. Young adults and their parents were mostly unaware of resources regarding education, job selection or obtaining a driver’s license. Professionals stated that these subjects were addressed during periodic appointments. Young adults didn’t always attend these appointments due to limited perceived benefit. To improve rehabilitation care, participants suggested methods for providing relevant information, facilitating peer contact and offering dedicated training programs to practice work-related tasks, prepare for job interviews or enhance self-confidence.
CONCLUSION:
Periodic appointments do not fulfil needs of young adults with transversal upper limb reduction deficiency. To improve care, rehabilitation teams should offer age-relevant information, share peer stories, and create dedicated training programs.
Introduction
Young adults with a transversal upper limb reduction deficiency (tULRD) who are in transition to adulthood appear to experience limitations in choosing and finding a suitable education or job as well as obtaining their driver’s license [1]. Little research is available concerning the possible role of the rehabilitation team in assisting these young adults and their parents in dealing with limitations during the transition from adolescence to adulthood.
Several factors can contribute to the limited role of the rehabilitation team in assisting young adults with tULRD in various transition phases. First, the healthcare system changes from a child-centred to an adult-oriented approach [2]. In the child-centred system, parents or caregivers take responsibility for health care navigation, while in the adult-oriented care system, young adults are expected to be more responsible for their own health and make their own decisions regarding healthcare consultations. This change in expected responsibility might hinder young adults in contacting the rehabilitation centre when they leave the familiar child-centred setting. Second, loss of contact with the rehabilitation team can be caused by changing priorities, altered social relationships, and shifting social roles of young adults in puberty [3, 4]. Whether these findings are applicable to young adults with tULRD is unknown, since recent studies did not focus on the transition of persons with such physical disabilities. Third, in recent years, the development of communication techniques has changed the way patients obtain information on healthcare issues. Previously, information was provided by healthcare professionals, television programs or leaflets. Nowadays, relevant information can be obtained by searching on the internet or by participating in social media. In view of widely available healthcare information, it is questionable whether the more traditional rehabilitation care still meets the needs of young adults with tULRD who are in transition from adolescence to adulthood. Additionally, in some countries, limited reimbursement of rehabilitation care by insurance companies may also play a role.
Therefore, the use and accessibility of rehabilitation care should be evaluated as to whether it meets the needs and expectations of these young adults. A previous study concerning young adults treated in paediatric rheumatology practices described the preference of young adults for an online program in which they can find and store all their health care information together with health care providers [5]. As parents obviously play an important role during transition, it is important that not only young adults, but also their parents know what to expect from health care providers during and after this transition phase [6]. To facilitate transition for young adults and their parents, it is important to discuss expectations and prepare for transition together with young adults, their parents and healthcare providers [7]. In a previous study, professionals in hospital-based teams noted that sequential transition programs appeared to improve the coordination of care [8].
The primary aim of this study was to evaluate the opinions of young adults with tULRD, their parents and healthcare professionals regarding the current role and accessibility of rehabilitation care in addressing limitations encountered in finding suitable education and employment as well as obtaining a driver’s license during the transition to adulthood. The secondary aim was to evaluate the needs and suggestions to improve rehabilitation care for young adults with tULRD and their parents.
Methods
Study design
We conducted a qualitative study consisting of an online focus group with young adults with tULRD and their parents. An asynchronous mode was used in which participants were free to log-in during a period of 4 consecutive days. Additionally, we held a face-to-face focus group with professionals to explore their opinions on current rehabilitation care and their suggestions for improvement. The consolidated criteria for reporting qualitative research (COREQ) were used to ensure transparent reporting [9].
Participants
Three groups of participants were included: (1) young adults with tULRD, (2) parents of young adults with tULRD and (3) healthcare professionals treating young adults with tULRD. Young adults, aged 15 to 25 years, with unilateral tULRD at the transradial or wrist disarticulation level and internet access were eligible for the study if they were also proficient in Dutch. Exclusion criteria were other congenital limb deficiencies, acquired upper limb amputations, lower limb amputations and comorbidities influencing participation in the study, such as cognitive deficiencies. The young adults with tULRD were recruited from local databases of four rehabilitation centres in the Netherlands with expertise in the rehabilitation care of individuals with upper limb deficiencies. Eligible young adults received an invitation letter to participate. The only eligibility criterion for parents was proficiency in Dutch. Regardless of the willingness of their child to participate, parents could join the study independently and received separate invitation letters. Healthcare professionals with at least one year of experience in treating young adults with tULRD were eligible for participation. Professionals participated during an annual national meeting of rehabilitation expert teams treating people with upper limb deficiencies. These expert teams consisted of rehabilitation physicians, physical and occupational therapists and prosthetists. The medical ethics committee of the Isala clinics in Zwolle (METC) decided that formal approval of the study was not necessary (file number: 16.11190). Participants gave written informed consent before participating.
Procedure
Online-focus groups (including young adults and parents)
An information technology expert was involved in building two separate online forums for the online focus groups. The forums were pilot tested by five persons, including able-bodied young adults, recruited from the social network of the researchers. The online forums for young adults and parents were accessible from November 20 to 23, 2017, on a secured website. Young adults and parents could join the forum daily from 8:00 AM till 11:00 PM. If young adults or parents did not login, they received a reminder by email the same day. Anonymity was guaranteed by using assigned pseudonyms. Young adults and parents were also asked not to mention their own names or addresses, the names of healthcare professionals or the names of the rehabilitation centre where they were treated. The following topics were discussed: the role of the rehabilitation team regarding selection of education (day 1), job selection (day 2), obtaining a driver’s license (day 3), and the accessibility of rehabilitation care (day 4). During these four days, the forum was online and continuously monitored by two moderators (KH, IL). The moderators asked additional questions when needed and monitored adherence to forum rules. They also encouraged the participation of more reluctant participants. The first moderator (KH) was working as a resident in rehabilitation medicine. Although this moderator (KH) had no experience in conducting qualitative research, KH had taken many patient histories and collaborated with co-authors who had experience in performing qualitative research, including online focus group studies. The second moderator (IL) worked as a paediatric rehabilitation physician and was experienced in conducting qualitative research [1]. KH had no prior relationship to the participating young adults and their parents, IL had interviewed three of the participants for a prior study [1]. The first moderator (KH) assigned the pseudonyms, and the second moderator (IL) was not informed about the identity of the participants. The number of participants in both online focus groups was based on the recommendation to include 8–15 participants during an asynchronous online focus study [10]. Conducting an online focus study requires less effort from participants, since they can participate from home. The asynchronous mode of conducting an online focus study was used, as it provides flexible login times for participants [11]. The latter might have increased the willingness for participation given the low prevalence (long travel distances) of this diagnosis and low demand for healthcare in comparison to other diagnoses. Moreover, the asynchronous mode gives more time for reflection and additional questions [10].
Face-to-face focus group (including professionals only)
Healthcare professionals with relevant expertise participated in a videotaped face-to-face focus group discussion. Open-ended questions constructed by the researchers regarding choice of education, job selection, obtaining a driver’s license and accessibility of rehabilitation care were used to explore the opinions and suggestions of the professionals. The content of this face-to-face focus group discussion was transcribed by an independent secretary. Subsequently, participants received the transcribed text and were asked to add information if needed and provide corrections where applicable.
Data analysis
For defining an appropriate structure to analyse the data, a coding framework was designed by the researchers. In this framework, themes were formulated according to the study aims (deduction), and new themes that were raised during data analysis were added (induction). There were five stages of data analysis in the framework approach (Fig. 1) [12]. Atlas-Ti (version 8) was used for indexing the data [13].
Summary of coding process.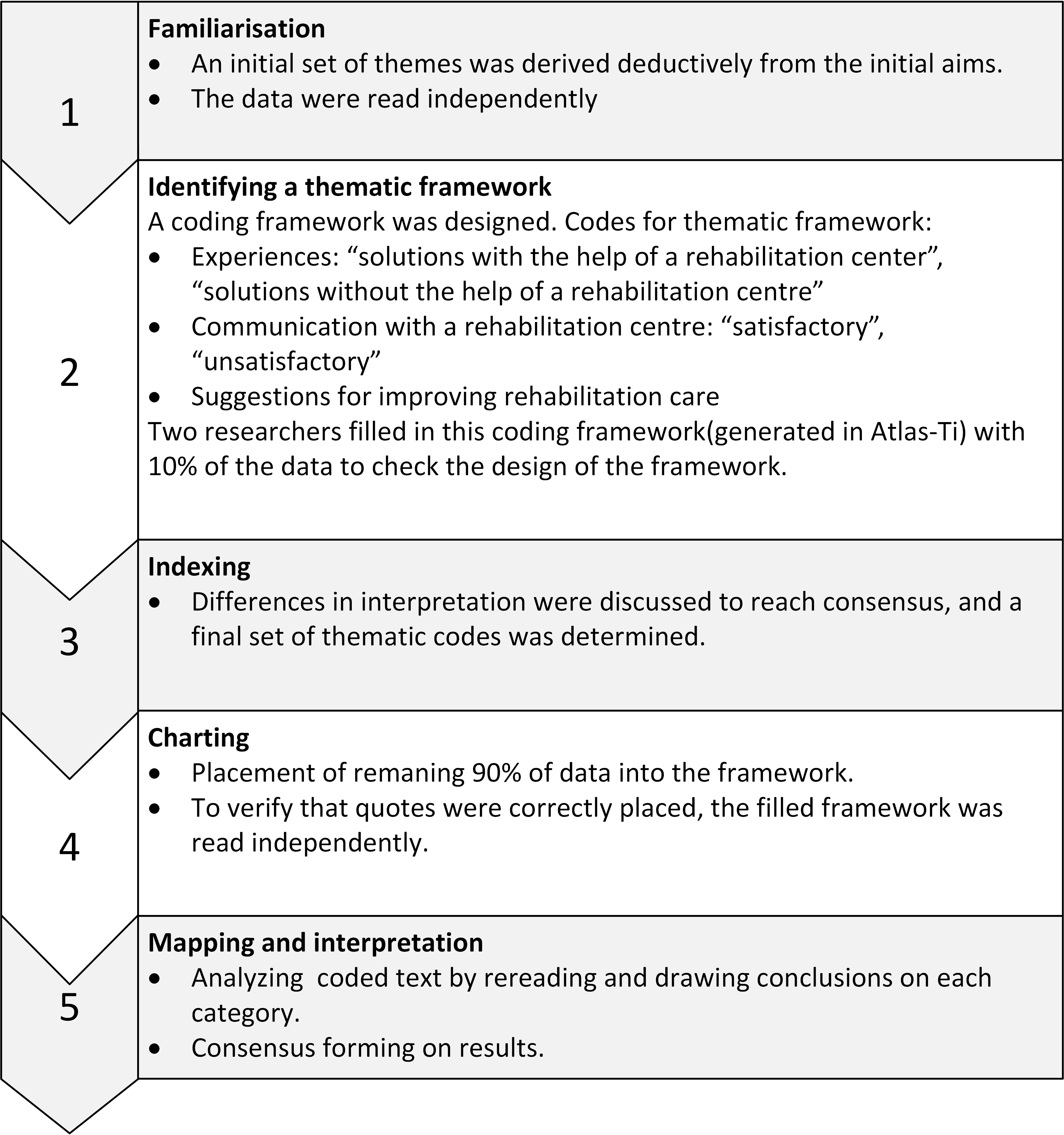
Participants
Online-focus groups (including young adults and parents)
Characteristics of young adults with tULRD (
16)
Characteristics of young adults with tULRD (
Number of postings per day (number of participants active on forum)
A total of 16 young adults and 11 parents participated in the online focus groups (Table 1). Nearly all participants logged in on each of the four days the forum was online (Table 2). One young adult only participated in the forum discussion on the first day. This participant responded by email to questions that were posted on the forum on days 2, 3 and 4. Data from this mail were included and analysed. Thirteen parents (4 males, 9 females) gave informed consent. Eleven pseudonyms were used; two sets of parents used the same pseudonym for responding. Only parents of young adults participating in the current study took part. In total, 192 responses (mean: 48 posts/day, range 37–60 posts/day) were collected. Most responses were collected on day 1 (Table 2).
A total of 17 healthcare professionals, consisting of 6 rehabilitation physicians, 9 occupational therapists, 1 prosthetist and 1 hand therapist participated in the face-to-face focus group. They were employed at 13 rehabilitation centres and 1 orthopaedic workshop; all were employed in the Netherlands.
Current role and accessibility of rehabilitation care
Young adults contacted the rehabilitation team mainly when they had problems concerning the residual limb, physical complaints due to overuse in their arm, back, neck or if they needed a prosthesis or an adaptive device. Most young adults and parents mentioned that they expected the rehabilitation team to address prevention and treatment of overuse symptoms. Occupational therapists stressed the importance of preventing overuse symptoms by giving ergonomic advice.
“We see people who have complaints about muscle pain but who are not aware that it could be the beginning of overuse symptoms.” (occupational therapist).
Nearly all young adults and parents described the rehabilitation team as being accessible when needed. However, many young adults and parents were unaware of expertise of the rehabilitation team regarding transition domains such as education, job selection or transportation.
“The rehabilitation centre didn’t play any role. I didn’t know that I could ask questions about job selection at the rehabilitation centre.” (young adult, female, 17 years old) “I think the accessibility is good, but people don’t always take time to consider this. Usually, things just happen by themselves.” (parent of a 16-year-old female young adult)
Most young adults and some parents indicated that periodic appointments had little added value for them. The unclear goals and limited benefits of periodic appointments were the main reasons given for no longer visiting the rehabilitation centre. Some parents stated that it was difficult to motivate their child to attend periodic appointments.
“I felt that members of the rehabilitation team thought I needed support, while I did not want it [periodic appointment] myself.” (young adult, female, age 24 years). “I haven’t visited the rehabilitation centre for the past two years. I do not need to go, but my parents think differently about this.” (young adult, female, age 17 years). “We would prefer to have more contact with the rehabilitation centre, for example by e-mail. My son has not had an appointment since his 18th birthday. He did not want me to make an appointment either.” (parent of a 23-year-old male young adult).
Most professionals indicated that topics concerning transition were addressed during periodic appointments and that they experienced difficulties in maintaining contact with these young adults. Various methods for providing relevant care were used by the professionals. Some continued to invite young adults for periodic consultations, while others organized peer meetings or invited them to join specific transition treatment modules. Most young adults and parents contacted the rehabilitation team by phone or by email.
Education/employment
Most young adults selected an education or employment within their field of interest and within their capabilities. However, when looking for an education program or a job, they did consider possible limitations related to tULRD. Less physically demanding education programs and jobs were often chosen by these young adults. Some parents stated that it was more difficult for those with a lower level of previous education to find a subsequent study compatible with their interests and capabilities compared to those with a higher level of previous education. Professionals indicated the importance of choosing an education program or job within the field of interest of the young adult and described their role in creating awareness of capabilities, possible limitations and the risks of overuse.
“Concerning selection of an education program, you take your capabilities and interests into account. If you have a disability you know there are still a lot of possibilities, but not everything will succeed.” (parent of a 16-year-old female young adult) “It [selection of an education program] starts with two questions: What are you excited about? What do you want?” (occupational therapist)
Some young adults and their parents stated that they had a slower working pace while typing or when performing other job duties. One young adult contacted the rehabilitation centre for information on how to qualify for governmental funding to compensate for limitations encountered during employment. Young adults and parents appreciated the role of the rehabilitation team in informing schools and employers about the capabilities and possible limitations of living with tULRD. Professionals also mentioned this educational role of the rehabilitation team.
“After my daughter was rejected for an education program, the occupational therapist joined her for a meeting at school and she was accepted afterwards.” (parent of a 21-year-old female young adult) “…and in this phase of life, they do not always want to take advice for granted …it is important to stay proactive in offering information regarding rehabilitation care.” (paediatric rehabilitation physician)
Transportation
Some young adults experienced difficulties while obtaining a driver’s license, but others did not. Experiences were varied and ranged from enrolling in a special driving school for disabled people to taking lessons at a regular driving school. Some drove in cars with automatic transmissions, while others had cars with a manual shift. Some used adaptive devices in the car, while others used no adaptive devices. Young adults who reported difficulties in finding a driving school also stated that some regular driving schools refused to enroll them but without giving a valid reason. Some young adults stated that they could not apply for special rate lessons and had to pay more per lesson. Some stated that it took longer to pass their exam. Some rehabilitation centres had their own driving school or provided a list with references of driving schools that could be contacted. Such information was highly appreciated by young adults and their parents.
“It felt like I had to pay more because of my short arm and that they were not prepared to offer special rates to people like me.” (young adult, female, 24 years old) “She needed a little boost from us to start driving lessons, …her hesitation was due to the emphasis on being different and having to deal with more rules and regulations ….” (parent of a 23-years-old female young adult)
Suggestions to improve rehabilitation care
Consultation and communication
Most young adults reported a need to receive or find relevant information themselves so they could make their own decisions concerning their healthcare. Information could be obtained from the internet, newsletters, forums or booklets. Many parents expressed the same need for information, but also valued informative meetings at the rehabilitation centre with or without their child. A joint appointment with their child-centered rehabilitation team and the new adult rehabilitation team at the time of transition was mentioned by some professionals as a way to facilitate this transition. This was mentioned once by a young adult. Professionals also suggested making relevant information and peer experiences easier to find. They emphasized the importance of quick responses to digitally posted questions from young adults and parents. Some professionals also mentioned social media, especially contact by mobile phone using dedicated apps as a possible solution for young adults to facilitate communication with the rehabilitation team. However, this possibility was hardly mentioned by the young adults themselves.
Rehabilitation training programs
To prepare for future tasks, young adults and parents suggested that the rehabilitation team should develop dedicated training programs for practicing work-related tasks and job interviews. Feelings of insecurity were mentioned by several young adults, especially when dealing with new situations such as applying for a new study or job. The rehabilitation team could play a role in enhancing self-confidence and could offer courses to help the young adults deal with new situations. This was suggested by young adults, parents and professionals.
An overview of suggestions for improving rehabilitation care is presented in Table 3.
Suggestions for improving rehabilitation care
Suggestions for improving rehabilitation care
Young adults with tULRD and their parents were often unaware of the expertise of rehabilitation teams regarding the selection of education and employment or obtaining a driver’s license. Professionals reported that they discussed these topics during periodic appointments. However, not many young adults attended these appointments because they believed that the goals were unclear or that little benefit would result.
Rehabilitation services that were seen as helpful informed schools and employers about the capabilities and possible limitations of young adults with tULRD as well as offering them dedicated training programs.
Self determination
Findings from this study were referred to the Self Determination Theory which argues that humans are optimally motivated and experience well-being when they have three basic psychological needs satisfied: the need for competence, the need for relatedness and the need for autonomy [14].
The need for competence can be described as the need to feel a sense of mastery over the environment and to develop new skills [14]. Our participants indicated that they felt a need for information to assist them with selecting jobs and education programs along with obtaining a driver’s license. Need for competence also relates to the finding that young adults mentioned that professionals could play a role in enhancing self-confidence.
Relatedness can be described as the need to feel connected to others [14]. Different methods of communication were mentioned to fulfil this need with professionals as well as share peer stories. According to the young adults, there is a need to gather information about strategies to overcome limitations encountered in selecting an education program or job and obtaining a driver’s license.
Based on the data acquired in the present study, young adults seem to desire to make their own decisions about healthcare. As autonomy is important in this phase of life, self-management skills should be a central part of any transitional program [15]. Therefore, it could be advisable for rehabilitation teams to develop a structure in which information reaches young adults that support and empower them to find solutions to their perceived limitations. Gaining access to the right information and sharing experiences may support young adults to gain more insight into their own situation, enhance autonomy and improve participation [16].
Consultation and communication
Using the internet was mentioned by young adults in this study as an option for gaining reliable information on demand. Online health communities are internet-based platforms for specific groups of patients [17]. Based on their accessibility, they can be classified as open access, closed access, or personal health communities [18].
An open access community consists of online information that is accessible to anyone [18], such as a website that could be used by young adults reading general information and peer stories as mentioned in this study. Sharing information in this way has the advantage of reaching a broad population, such as other young adults with a rare condition, their parents, teachers or employers and young adults who do not visit a rehabilitation centre or patient support organization. A drawback of open access systems is that personal information should not or cannot be shared due to safety issues and privacy regulations.
A closed access community is accessible only by members [18]. Communication and collaboration between a group of professionals and patients can be accomplished in this way, for example, by joining a patient support organization. Visible collaboration between professionals and patient support organizations, as well as exchanging information between those groups, was suggested to improve rehabilitation care by young adults and parents in this study. A closed access online health community could fulfil this need. Disadvantages of this type of community include inaccessibility for non-members and the need for a host to ensure the continuation of the closed access system in terms of content and financing.
Personal health communities give members the option of storing their private medical information at a central location and also allow communication between invited members [18]. Such a community is personalized and has more security; the patient is the owner of this system. Personal health communities were not mentioned in our study, probably due to a lack of knowledge by young adults and their parents about such systems.
Developing an online program, with open or closed accessibility, could actively empower young adults in their healthcare process and address their individual needs [18]. In contrast to most young adults and parents, professionals suggested using apps on mobile phones to improve the accessibility of care. Although apps are being used frequently nowadays, this was not mentioned as a preferred way of communication by the young adults in our study. It might be that a synchronous online focus group or face-to-face focus group discussion for the young adults might have facilitated more conversations about this idea.
A previous study reported that patients preferably received information by e-mail or websites, rather than by social media, because the participants were more confident using those platforms [19]. This may also apply to participants in our study and may explain why they did not mention apps as an option. Additionally, social determinants such as lack of a computer in the home or poor internet access may pose barriers for some individuals in using this technology.
Organization of rehabilitation care
If rehabilitation care for young adults with tULRD were improved by offering dedicated information on demand and by enhancing autonomy, the work processes of rehabilitation professionals would require adaptation to modern communication technologies. The use of such tools requires digital security measures, which entail additional costs [18]. To improve and modernize rehabilitation care, options to reimburse finances for more types of e-health activities should be discussed with health insurers in the future.
An important finding of our study was that regular appointments at the rehabilitation centre were often not valued by the young adults due to the lack of perceived benefits.
Young adults suggested that appointments should be made on demand to enhance the perceived benefit. Enhancing benefits and motivation, as part of the self-determination theory, could possibly be achieved by assessing meaningful goals for young adults in an early stage of rehabilitation treatment, for example by regular administration of the Canadian Occupational Performance Measure [20] or similar tools or checklists. To modernize rehabilitation care, rehabilitation teams should revise the structure of regular appointments or be more clear about the content, aims, and possible benefits of these appointments.
Furthermore, dedicated training programs could be offered to overcome limitations in work-related skills or to enhance self-confidence. When obtaining a driver’s license, it was striking that many different regulations were applied and various experiences were shared while all young adults had a comparable level of deficiency and all were tested by the national Central Agency of Driving skills before they started their driving lessons. Equalizing rules and regulations for driving with a physical disability needs more attention from governmental organizations.
Strengths and limitations
Young adults, aged 15 to 25 years, with tULRD at the transradial or wrist disarticulation level were included to provide a homogenous study population regarding level of deficiency. These participants were heading towards transition, were currently in the process of transition or had already gone through transition. Our participants were in different stages of transition, which gave a broad view in experiences and ideas. However, this might have also influenced the responses, since a number of participants already passed the transitional phase and may have answered from a different perspective. For future research, we would recommend stratifying participation by transitional stage, preferably in a larger sample size. Including participants from four rehabilitation centres ensured that the range of current practices in the Netherlands were taken into account.
Rehabilitation centers in the Netherlands may differ in the specific type of care they provide to these young adults, possibly limiting generalization which can be seen as a limitation of the study. However, the opinions of the young adults concerning the different rehabilitation centres seemed to be rather similar, so our multi-centre approach likely influenced the results in a positive way and increased the external validity.
Our present study included only young adults who actually visited the rehabilitation centre, which may have provided skewed results. Young adults with tULRD who have never visited a rehabilitation team may not experience any limitations or may have solved problems autonomously by finding information and applying problem-strategies themselves.
An aspect that needs attention in conducting an online focus study within the asynchronous mode is the absence of real-time discussion, as in a face-to-face focus group [21]. Less interaction between participants may have resulted in less detailed information. On the other hand, it could be that the anonymity of an online focus group compared to a face-to-face focus group created more openness in answering the questions. To support constructive discussions and to optimize the results, two moderators were constantly online during the opening times of the forums.
Professionals joined a face-to-face focus group instead of an online focus group. We took the opportunity to include a broad selection of professionals from a national meeting on the topic of working with these young adults. The format of the online focus group study could have led to a lower number of participating professionals with this expertise, since the preferred number of participants of a focus group is limited and it would have required more time investment of each individual.
We used the framework approach to gain transparency in creating the set of outcomes and used the COREQ criteria to present the methodology transparently [9]. Concerning the COREQ criteria, we cannot provide information on reasons for non-participation. We do not know why young adults did not respond to invitation letters or if they would have had other needs and suggestions.
The results of this study are not directly applicable to other patient populations in the transition phase. This is because young adults with tULRD have a low demand for healthcare and may have other needs and suggestions compared to young adults with a higher demand for healthcare. At the same time, the study suggests low demand for healthcare might be due to a lack of understanding of the scope of rehabilitation care services in the transition phase and professionals may not fully engage the young adults. This could cause underestimation of the need for healthcare by these young adults as well as that of young adults with other diagnoses in transition phase.
Finally, the rehabilitation service for our participants is based on the Dutch healthcare system and the results of this study cannot be directly generalized to other countries.
Conclusion
The role of the rehabilitation team regarding the selection of education and employment along with obtaining a driver’s license is often unclear, and periodic appointments with rehabilitation professionals do not adequately match the needs of young adults with tULRD in transition to adulthood and their parents. Rehabilitation care for young adults with tULRD and their parents should aim at developing methods for providing reliable information and sharing peer experiences in order for them to stay connected and meet their needs for developing autonomy.
Footnotes
Acknowledgments
The authors would like to thank J. Luiken (ICT student) for developing the online forum on a website and being accessible during the online focus groups, J. Bouwman, secretary, for transcribing the videotape of the group discussion and Charles Frink from v.o.f. Frink Communications for his English language editing service.
Conflict of interest
The authors report no declarations of interest. There was no potential conflict of interest because the funding bodies were not involved in designing or performing the study and were not informed about the results before finishing the study.
Funding
This study was funded by ProReva, orthopaedic specialists and suppliers, the Netherlands, Educational budget Rehabilitation Centre Vogellanden, Foundation Beatrixoord Northern Netherlands, The Hoogstraat Rehabilitation Research foundation.