
Abstract
PURPOSE:
Neurogenic bowel dysfunction (NBD) is a common comorbidity of myelomeningocele (MMC), the most common and severe form of spina bifida. The National Spina Bifida Patient Registry (NSBPR) is a research collaboration between the CDC and Spina Bifida Clinics. Fecal continence (continence) outcomes for common treatment modalities for NBD have not been described in a large sample of individuals with MMC. NSBPR patients with MMC and NBD were studied to determine variation in continence status and their ability to perform their treatment independently according to treatment modality and individual characteristics.
METHODS:
Continence was defined as
RESULTS:
At total of 3670 members of the NSBPR met inclusion criteria between November 2013 and December 2017. Overall prevalence of continence was 45%. Prevalence ranged from 40–69% across different treatments. Among continent individuals, 60% achieved continence without surgery. Antegrade enemas were the most commonly used treatment and had the highest associated continence rate. Ability to carry out a treatment independently increased with age. Multivariable logistic regression showed significantly higher odds of continence among individuals aged
Abbreviations
Introduction
Myelomeningocele (MMC) is the most common and severe form of spina bifida (SB) and is a permanently disabling congenital condition. Neurogenic bowel dysfunction (NBD) is a significant comorbidity that affects most individuals with MMC, resulting in fecal incontinence and/or chronic constipation. Fecal incontinence in MMC has been associated with decreased health-related quality of life, depression, discrimination by peers, decreased school attendance, lower educational attainment, and lower rates of employment [1, 2, 3]. Worrying about fecal continence contributes to emotional, physical, and psychological distress [4]. Families and caregivers of individuals with NBD report decreased quality of life, the causes of which include the time, effort, and unpleasantness of helping with NBD management [5, 6, 7, 8, 9]. Secondary concerns from NBD include urinary incontinence, urinary tract infections, ventriculoperitoneal shunt malfunction, skin breakdown, hemorrhoids, and anal fissures [10, 11, 12, 13, 14, 15, 16]. Of MMC individuals with NBD, 80% are on a management program for constipation and/or fecal continence [17, 18].
The National Spina Bifida Patient Registry (NSBPR) is a collaboration between the CDC and 35 clinics across the U.S. The purpose of the NSBPR is to provide a research platform to improve the care of people with SB. Data about fecal continence status and treatments used for NBD are collected annually. In the initial report from the NSBPR from 10 clinics, only 30% of individuals with MMC reported fecal continence. This was reported as a binary subjective report of continence [19]. Later, the prevalence of continence ranged from 24% to 59% among 12 clinics with more than 200 individuals enrolled. This variation suggests that there may be modifiable factors that could improve NBD outcomes. Additionally, prior studies with the NSBPR have shown that sociodemographic factors may be related to fecal continence rates [20].
To date, there is no standard of care for the management of NBD and its associated outcomes including fecal incontinence and constipation. Therefore, we used data from the NSBPR to compare continence outcomes across common treatment modalities for NBD and to identify sociodemographic factors associated with these outcomes and the individuals’ ability to perform their own treatment independently.
Methods
NSBPR
Standard data collection tools are used to obtain de-identified data from each of the multidisciplinary SB clinics. After initial enrollment, an annual visit form is used to update information on demographic and clinical characteristics as well as treatment history. Clinics can collect data for the visit form in various ways, including face-to-face interviews, written survey instruments, or clinician notes. Data collection for the registry was approved by the Institutional Review Board of each clinic site. To avoid diagnostic heterogeneity, our sample was limited to those with MMC.
Data from the most recent clinic visit were analyzed. Inclusion criteria were: MMC form of SB, last visit after October 2013 (when data collection forms were revised to include frequency of fecal incontinence episodes), age
Criterion treatment modalities included in National Spina Bifida Patient Registry in order of invasiveness (least to most)
Criterion treatment modalities included in National Spina Bifida Patient Registry in order of invasiveness (least to most)
Age was categorized by: early childhood (5– 11 years), adolescent (12–19 years), and adult (over 19 years of age). Health insurance status was recorded at each visit as either having any private insurance or no private insurance. Sex and race/ethnicity data were also collected.
Spinal cord level of motor function
The lowest spinal cord level of motor function found on examination was recorded for each lower limb as: thoracic (flaccid lower limb); high-lumbar (hip flexion present); mid-lumbar (knee extension present); low-lumbar (foot dorsiflexion present); or sacral (foot plantar flexion present). When the left and right sides differed, the more severely involved side was used to represent that individual’s overall functional level.
NBD management techniques and treatment modalities
Data were collected on 11 frequently used treatment modalities for NBD (Table 1); the online Supplementary Appendix B has more detailed information about these modalities). As a construct for the analyses, criterion treatment modalities (CTMs) for NBD were ranked based on invasiveness of administration. Treatment options requiring surgery were judged to be more invasive than non-surgical options. When a person reported more than one CTM, the most invasive treatment modality was used to classify that person’s CTM. The continence rates associated with using a CTM exclusively versus in conjunction with other CTMs was analyzed.
Ability to perform CTM independently
CTM data for each individual was collected as a binary variable regarding their ability to perform their own CTM independently.
Statistical analysis
Associations among independent categorical variables were evaluated by chi-square tests. When an expected cell count was
Individuals were stratified by motor function category. Univariate logistic regression models were used to determine the odds of continence for each CTM, compared to timed defecation (referent). Timed defecation was used as referent because it is the least invasive CTM. Statistical analyses were performed using SAS version 9.4 (Cary, NC, USA).
Results
Study population
Through December 2017, 8662 individuals were enrolled in the NSBPR and 3670 met our inclusion criteria and composed our study population (Fig. 1). Demographic and clinical characteristics are shown in Table 2. Similar to other NSBPR studies, this study had high proportions of females (56.2% among those 20 years old or older), non-Hispanic whites (63% overall), individuals with mid-lumbar level lesions (31.6% overall), and individuals with no private insurance (57.1%) [3, 20, 21].
CONSORT of study population from National Spina Bifida Patient Registry, December 2017. Version 2 data collection started October 2013; additional questions were added to the registry to obtain more detailed data on outcomes, additional procedures, imaging studies, and lab results. Also, two other diagnoses (Terminal Myelocystocele and Split Cord Malformation) were added to the eligible diagnoses. Specifically, answer choices for continence were changed from previous Yes/No to more detailed incontinence frequency.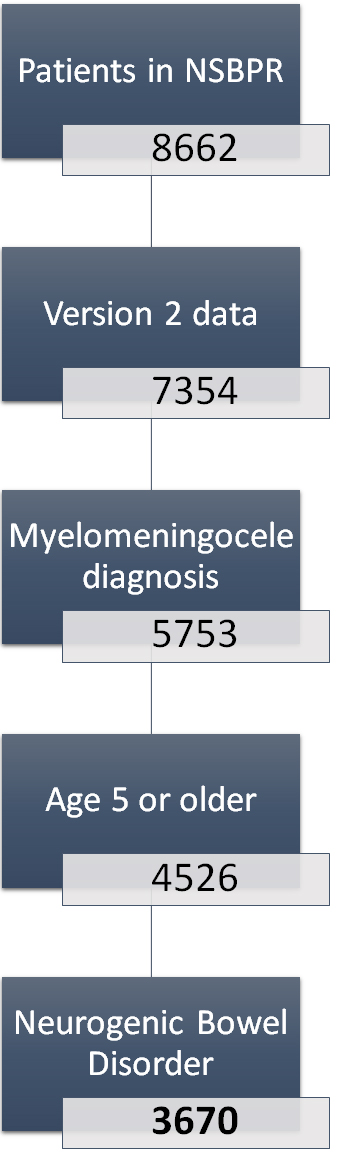
Key demographic and clinical characteristics of individuals
Rates of usage of each CTM is presented in Table 3. The most commonly used CTM in this population with NBD was antegrade enemas (27%), followed by oral medications only (23%). The prevalence of use of each CTM by age category and by level of motor function is presented in online Appendix Tables A1 and A2. The factors that increased the odds of using any CTM were adolescent age, female sex, non-Hispanic ethnicity, and having private insurance (see online Appendix Table A3).
Prevalence of fecal continence
by criterion treatment modality and age in individuals with myelomeningocele and neurogenic bowel dysfunction in the National Spina Bifida Patient Registry, November 2013–December 2017
Prevalence of fecal continence
The overall prevalence of fecal continence in the study population was 45%. Among those that were continent, 60% had no record of surgical intervention. Additionally, 14.1% of the study population did not report any CTM and were incontinent.
On multiple logistic regression analysis, higher odds of continence were associated with being older, female, non-Hispanic white, or having any private health insurance. Individuals with sacral and low-lumbar level of motor function also had higher odds of continence than those with higher levels of motor function involvement (Table 4).
Summary of multiple logistic regression on fecal continence
among individuals
5 years of age with myelomeningocele and neurogenic bowel dysfunction in the National Spina Bifida Patient Registry, November 2013–December 2017 (
3589, patients with pouched fecal diversion were excluded)
Summary of multiple logistic regression on fecal continence
The overall rate of continence associated with each CTM ranged from 35.9% (manual disimpaction) to 68.6% (antegrade enemas) (Table 3). Antegrade enemas were also the most commonly used CTM (26.5%). Cone/balloon large volume enemas and Peristeen
The prevalence of continence increased with age for all CTMs except cone/balloon enemas and mini-enema, for which peak continence rates were found in adolescents. In children, antegrade enemas had the highest associated continence rate (66%), followed by cone/balloon enemas (57%). In adolescents, transanal irrigation had the highest associated continence rate (80%), while antegrade enemas had the second highest rate (70%). In adults, timed defecation had the highest associated continence rate (79%), followed by standard rectal enemas (76%) (Table 3).
The variation in continence rates by level of motor function was statistically significant for only two of the CTMs: oral medications and rectal suppositories. These two CTMs both showed higher rates of continence in individuals with low lumbar and sacral levels than those with higher levels (Appendix Table A4).
Prevalence of independent use by criterion treatment modality and age in individuals with myelomeningocele and neurogenic bowel dysfunction in the National Spina Bifida Patient Registry, November 2013–December 2017
Prevalence of independent use by criterion treatment modality and age in individuals with myelomeningocele and neurogenic bowel dysfunction in the National Spina Bifida Patient Registry, November 2013–December 2017
Prevalence of fecal continence
Univariate logistic regression analysis for continence with a CTM by level of motor function found that antegrade enemas were significantly associated with continence in each level of motor function (Table A5). Retrograde large volume enemas (combined Cone/balloon large volume enemas and Peristeen
Only 23% of individuals were independently able to perform their own CTM. The overall rate of independence in carrying out a CTM ranged from 13% for transanal irrigation to 56% for antegrade enemas. The rate of independent use for each CTM increased with age (Table 5). Timed defecation was the CTM with the highest probability of being carried out independently in all age groups. Most individuals, regardless of age, were not able to administer other CTMs independently.
Combinations of CTMs
The continence rates for each CTM when used on its own or in conjunction with an oral agent are listed in Table 6. The addition of oral agents to a CTM was associated with a lower rate of continence for all CTMs, which was statistically significant for six of the nine CTMs examined.
Only 5.5% of individuals utilized more than one CTM (177 used 2 CTMs, 21 used 3 CTMs, 3 used 4 CTMs, and 2 used 5 CTMs). Over half (53%) of those who used 2 or more CTMs had timed defecation as their second CTM. When a CTM was used in conjunction with another CTM, the continence rate did not increase, except for manual disimpaction (see online Appendix Table A6).
Discussion
To our knowledge, this is the first study to systematically evaluate the use and effectiveness of common treatment modalities for NBD in individuals with MMC. The goal of NBD treatment is to find the most effective and least intrusive management for each individual. The use of a large multi-institutional cohort allowed acquisition of sufficient statistical power to allow meaningful comparisons between CTMs.
The fecal continence rate for the overall actively managed cohort was low at 45%. Of this MMC cohort with NBD, 14% did not report using any CTM and reported being incontinent. Given the association of fecal continence with employment and educational attainment for adults with MMC [3], we believe this overall low fecal continence rate to be a major problem for this population.
Our definition of fecal continence was having less than one fecal incontinent episode per month. Some individuals may have more than one incontinent episode but are satisfied with their continence; satisfaction was not directly evaluated in this study. Furthermore, the registry does not collect the quantity of incontinency episodes, so a CTM could greatly reduce the number of these episodes or the volume of the episodes but still not be reported as “successful” by our definition. The data collected were from the most recent clinic visit, therefore fluctuations in continence could also over- or underestimate reported continence rates [22]. Given that this study evaluated cross-sectional data, we were unable to determine the length of time that an individual had been on their CTM. There may have been individuals who recently changed to a new CTM and the effect of that change was not captured in the analysis.
One of the most striking findings of our analysis was the association of fecal continence with the socioeconomic factors of race/ethnicity and private insurance. Similar to the conclusions of previous studies that reported similar results, this finding is unlikely to be explained by biological factors alone [23]. This could be related to caregivers, providers, or both. Provider biases may exist in offering more invasive modalities to those of higher socioeconomic status or certain ethnic/racial groups. Some CTMs are not covered by all insurances within all states and therefore the ability to use a CTM may be affected by insurance coverage, socioeconomic status of the individual, and state of residence. Uncovered medical expenses and cost to families to attend multiple follow-ups for closely monitored CTMs may not be as easily attained by those of lower socioeconomic status. Antegrade enemas require surgery or percutaneous access, which creates a potential for variation in referral patterns.
It is clear from our analysis that there is not one overall best CTM for management of NBD. We think that the CTM hierarchy in Table 1 may be used as a guide for sequentially offering NBD treatments until continence is achieved. This suggestion follows updated expert panel guidelines for bowel function and care for people with SB which recommends beginning with non-intrusive treatments or dietary management (“Guidelines from the official Spina Bifida Website”:
Sixty-percent of the continent individuals in this analysis appear to have achieved continence without surgical intervention. Antegrade enemas were associated with the highest continence rates in all age groups but require surgical intervention or percutaneous tube placement, often with revisions. In a meta-analysis of NBD management in SB, Velde et al. found that retrograde enemas resulted in a continence rate of 80%, compared to 81% for antegrade enemas, and 23% of the latter cohort required “redo” surgery for stoma complications [24]. Due to the invasive nature of antegrade enemas we believe they should not be offered without first determining if fecal continence can be achieved with a less invasive, non-surgical method.
Retrograde devices (transanal irrigation and cone/ balloon large volume enemas) were associated with continence rates that were below that of antegrade enemas, but they were not greatly inferior and may be tried before surgical intervention.
The risks and benefits of any treatment modality must be weighed carefully and the choice of a CTM tailored for each individual and family. Sturkenboom et al. discussed the potential impact of antegrade enemas on outcomes such as pain, well-being, function, surgical complications, and quality of life, in addition to continence [25]. Optimization of a bowel treatment must include an evaluation of the need or want for independence and fecal continence, manual dexterity of the patient, ability of the patient to transfer to a commode or toilet for the program, and other factors that are unique to each individual.
The number of individuals able to complete their bowel management treatment independently were low for the entire group with only 23% of individuals able to carry out their regimen independently. The ability to complete a regimen independently increased with age, as would be expected, to 33% in adults. Antegrade enemas and timed defecation were the CTMs most likely to be performed independently.
We did not analyze if starting interventions at a younger age would result in better continence rates because this was a cross-sectional and not longitudinal analysis. Hypothetically, earlier active management of NBD could result in better long-term outcomes by improving expectations in continence outcomes and possibly preventing long-term consequences of chronic constipation. This issue deserves further inquiry.
Proper and repeated education regarding the importance of NBD management and continence is crucial. Education should include a realistic expectation of continence and independence and an understanding that multiple CTMs likely will be trialed until a satisfactory regimen is found. Clinically, we believe that achieving continence in early childhood is advantageous to limit bullying, increase or preserve self-esteem, and improve quality of life associated with fecal incontinence [26, 27, 28].
The findings of our study must be interpreted in the context of several limitations. While definitions are provided for continence outcomes, these can be subject to variation in their interpretation and reporting. This raises particular caveats when attempting to compare outcomes among different centers, as the data may have been collected in subtly (though significantly) different ways. For example, continence data taken from face-to-face interviews may not be identical to that taken from written survey instruments, or data derived from clinician notes. Recall bias from individuals may also occur in reporting their continence. It is tempting to compare the effectiveness between the different CTMs, however a rigorous comparative analysis between CTMs was not performed. It was not carried out since this was cross-sectional and individuals utilizing a more invasive CTM may have previously had poorer results on less invasive therapy in the past, thus overestimating the latter’s efficacy. Future analysis of longitudinal data in the NSBPR may better clarify that issue.
Similarly, selection bias may reduce the generalizability of these results. NSBPR involves multidisciplinary clinics at selected centers of excellence, so our findings may not be applicable to individuals with SB who either do not attend multidisciplinary SB clinics or attend clinics that are less rigorous than the clinics participating in the registry.
Despite these limitations, there are many strengths of this analysis. This is the first systematic analysis of a large cohort of individuals with MMC in regards to NBD and treatment outcomes. The analysis was carried out utilizing a novel hierarchical approach to the CTMs. Further studies assessing longitudinal data from this cohort would build on the effort to best manage these patients.
Conclusions
Our findings, in a large group of subjects with MMC and NBD, demonstrate statistically significant higher odds of continence in adolescents, females, and non-Hispanic whites, as well as those who have private insurance. Overall continence rates for those with NBD in this data registry group who used a CTM (or more than one) were modest, ranging from 36% to 69%. Although antegrade enemas were associated with the highest rate of continence in this population, our findings do not imply a causal connection between antegrade enemas and continence. Personalized treatment algorithms should be used for individuals with MMC to achieve continence, independence in carrying out their treatment, and satisfaction.
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/PRM-190667.
Footnotes
Acknowledgments
The authors thank the many individuals with SB and their family members who participated in this research, without whom the NSBPR would not be possible. The authors also wish to acknowledge the Jones and Guerrero Fund and the Kenneth and Elaine Jones family for their support of this project.
The National Spina Bifida Patient Registry is funded by the National Center on Birth Defects and Developmental Disabilities, Centers for Disease Control and Prevention, Atlanta, Georgia (Grants 5U01DD001065-03, 5U01DD001069-03, 5U01DD001071, 5U01DD001 093-03, 5U01DD001063-03, 5U01DD001080-03, 5U0 1DD001091-03, 5U01DD001082-03, 5U01DD001078-03, 5U01DD001062-03, 5U01DD001073-03 and 5U01 DD001074-03).
Conflict of interest
Drs. Sawin, Wiener, Routh, Castillo, DiCianno, Sherburne and Smith are currently funded investigators on the NSBPR funded by the CDC. Dr. Kelly serves on an advisory board and received an honorarium from Coloplast Corp., manufacturer of Peristeen