
Abstract
PURPOSE:
The purpose of this study was to assess the knowledge, attitude and practices of health care professionals in pediatric settings on developmental surveillance and screening programs and also to identify the barriers and facilitators during its implementation.
METHODS:
The data were collected from health professionals involved in pediatric developmental care, practicing in various hospitals, clinics and nursing homes in a suburban city on west coast of Southern India. The study involved cross-sectional exploratory sequential mixed method design which included a quantitative questionnaire survey on health professionals (
RESULTS:
The study results indicate that health professionals involved in pediatric developmental care in Indian health care settings have fair knowledge and a favorable attitude towards the use of developmental surveillance and screening. Furthermore, the facilitators and barriers of implementation have been reported. The strategies outlined by interview respondents to improve adherence to implementation have been discussed.
CONCLUSIONS:
The practice of developmental surveillance and screening is limited despite favorable knowledge and attitude among health professionals in pediatric developmental care and is dependent on health care organizational setup.
Keywords
Introduction
The developmental trajectory of an infant across motor, cognitive, language, social, and emotional domains is typical and interdependent. Developmental milestones provide references for typical patterns of development across domains; an absence of key milestones along the developmental trajectory raises a developmental red flag [1]. Children with developmental disabilities invariably have delays in acquisition of milestones in one or more domains. Globally, the prevalence of developmental disabilities in children is estimated at 8.1% [7.7–9.1] with India reporting the highest prevalence of years lived with disabilities (YLDs) for all developmental disabilities except attention deficit hyperactivity disorder [2]. YLDs in India have not improved since 1990 [2]. Secondary prevention of developmental disabilities should be targeted by early identification and confirmation of red flags through surveillance and screening programs [3].
Developmental surveillance relates to the process of identifying the children at risk of developmental delay, whereas the developmental screening relates to the administration of a standardized screening tool in specific domains or areas of concern to discriminate atypical development and confirm such risk of developmental delay [4]. The American Academy of Pediatrics (AAP) recommends that all infants and young children be screened for early identification of developmental delays in order to initiate appropriate early intervention services [5]. The AAP also provides an algorithm for developmental surveillance and screening to support pediatric health care professionals [5]. Developmental surveillance should be provided when there is a developmental concern and at all well-child visits at 9, 18, and 24–30 months [6, 7, 8, 9]. The Indian Academy of Pediatrics (IAP) in its consensus statements on evaluation and management of autism spectrum disorder (ASD) [10] and attention deficit hyperactivity disorder (ADHD) [11] recommends developmental screening for ASD at 18 and 24 months, and for ADHD at 4–18 years. A review article has provided an algorithmic schedule of developmental screening based on the degree of risk for developmental delays in Indian practice settings [12].
Flow of participants.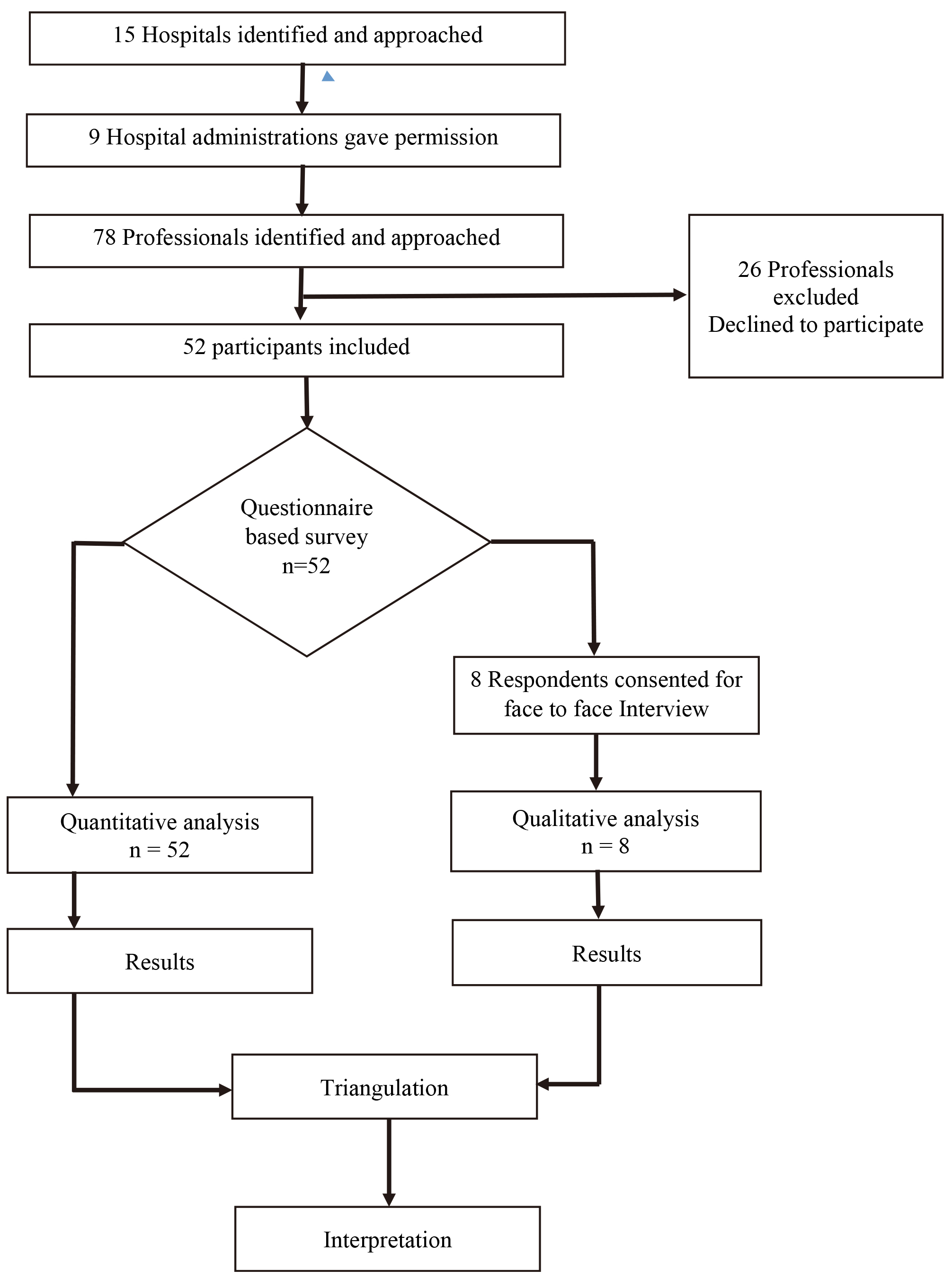
The countries of Asia-Pacific region have developed the Incheon Strategy towards achieving ten overarching disability inclusive developmental goals with 27 targets and 62 indicators to “make the right real” for persons with disabilities [13]. To further the mandate of Incheon Strategy core indicator 5.1 on number of children with disabilities receiving early childhood intervention, under National Health Mission, the Government of India launched Rashtriya Bal Swasthya Karyakram (RBSK) in 2013, an initiative offering comprehensive child health screening and early intervention services. The scope of developmental surveillance and screening is not clearly stated in the initiative [14]. The Research Priority Setting (RPS), a collaborative initiative of Indian Council of Medical Research and International Clinical Epidemiology Network (ICMR-INCLEN), has identified implementation of integrated and comprehensive new-born and child health care packages that provide continuum of care and improving quality of life as one of the strategic research priority [15].
Despite the recommendations for ongoing developmental surveillance and screening, several studies have reported challenges and barriers in the implementation of such programs [16, 17, 18, 19]. The current practices of developmental surveillance and screening in Indian context is not known. The present study used an exploratory sequential mixed-methods design to assess the knowledge, attitude and practices on developmental surveillance and screening. In addition, it examined the various factors which would serve either as facilitators and barriers in the implementation of developmental surveillance and screening programs in Indian health care settings.
Demographic characteristics of participants
The study used a cross-sectional sequential exploratory mixed method involving a survey followed by face to face interviews of the pediatric health professionals. A questionnaire and an interview guide were prepared and validated specifically for this study. Both instruments were developed and validated using Delphi consensus by seven experts from various health professions in the field of pediatric care. The questionnaire and interview guide, developed in English, included questions under three broad domains i.e. knowledge, attitude and practice associated for the use of developmental surveillance and screening tools among various health professionals. This study was approved by Institution Ethics Committee and also registered with Clinical Trial Registry of India. The investigators recruited a convenience sample of 52 health professionals from a suburban city on west coast of Southern India. This included pediatricians, nurses, physiotherapists, occupational therapists, speech therapists, optometrists and clinical psychologists working in pediatric set-ups with minimum one year of experience. Professionals not comfortable with English as a mode of communication were excluded.
Procedure
Fifteen hospitals were identified and administrative permission was obtained from nine. The six other health care units which declined or have not responded to the request include Government primary health care centers and private nursing homes or clinics. The investigators then identified 78 prospective participants from nine hospitals and contacted each health care professional in person. An informed consent was taken prior to the administration of the questionnaire and 52 participants consented to participate (Fig. 1).
Survey
The investigators provided the participants with the questionnaire in person with detailed description of each component. Participants were given a period of one week to complete the questionnaire followed by three reminders, each at the end of first, second and third week. In case of further delay in response, a final reminder was given at the end of the fourth week after which the participant was declared a non-respondent. There were no non-respondents.
Face-to-face interviews
The investigators targeted at least two respondents of the survey from each profession to participate in face-to-face interviews. However, the only eight respondents who consented included one pediatrician, one nurse practitioner, one speech therapist, two psychologists, and three physiotherapists. In absence of any other individual, the face-to-face interview was conducted using a semi-structured and validated interview guide comprising open-ended questions. This was at a time convenient for participants at their workplace. Each interview lasted for 8 to 10 minutes. No repeat interviews were carried out. Researcher audiotaped all the interviews with a voice recorder.
Data analysis
Quantitative data analysis was done using MS Excel 2013. Descriptive statistics were used to report demographics using mean and standard deviation. Frequencies and percentages of the responses were calculated. All interviews were transcribed verbatim, anonymized and analyzed by the researcher. Codes were derived using inductive content analysis and grouped under categories and then into themes which were discussed and agreed upon by consensus of all investigators. Data saturation was not reached as the number of consenting participants was less than targeted.
Results
Most of the study participants (92.3%) worked in a tertiary care hospital. Forty-eight percent of the participants were professionals from speech therapy, and forty-eight percent of the participants had a post-graduation or doctoral qualification (Table 1). Most participants gave correct responses to the questions related to the guidelines regarding developmental screening. However, the majority could not differentiate between developmental surveillance and developmental screening (Table 2).
Knowledge, attitude and practice on developmental surveillance and screening
Knowledge, attitude and practice on developmental surveillance and screening
Participants considered an ideal screening tool to be comprehensive, language specific, cost effective, quick to administer and with good psychometrics. Some of their responses follow:
“it should include all the aspects of development motor, sensory, cognitive;” “it should cover the language differences;” “quick enough;” “a tool which is freely available, widely accepted by all the health care providers, will be a valuable tool;” “It should also be statistically appropriate, content validity and all.”
Participants were aware of the developmental screening guidelines specific to their own specialty, such as those from Indian Speech and Hearing Association, American Speech-Language-Hearing Association, American Academy of Pediatrics and Indian Association of Pediatrics. The participants responded saying that:
“The ones that is given by the specific association, like pediatric one, American guidelines are commonly used;” “Specific professionals have their own guidelines within their scope of practice, for instance for speech and hearing, ASHA guidelines are there or Indian speech and hearing guidelines are there.”
However, most were unaware of the guidelines related to developmental surveillance in general. The responses of the participants include:
“Surveillance I am not sure;” “Screening they say that regularly you need to do;” “If any parent is having any concern or if antenatal they had any problem, if they have any family history of developmental delay. Those times you may have to do (screening).”
Most of the participants had a favorable attitude towards screening and early identification of developmental delays, and the majority (76.9%) believed that children without risk should also be followed up with developmental surveillance and screening. Fifty percent of participants agreed that developmental surveillance alone is not sufficient for identification of children with developmental delay, and should be backed up with formal screening using a standardized tool. Ninety-six percent of participants agreed that parental input is vital (Table 2). Forty-one (79%) have been trained in administration of some developmental screening tools and thirty-five (67%) are currently using them in their setup (Fig. 2). Twenty-five (48.1%) reported using an assessment based screening tool (Table 2).
Barriers and facilitators to the use of developmental screening tools
Training and use of developmental screening tools among participants.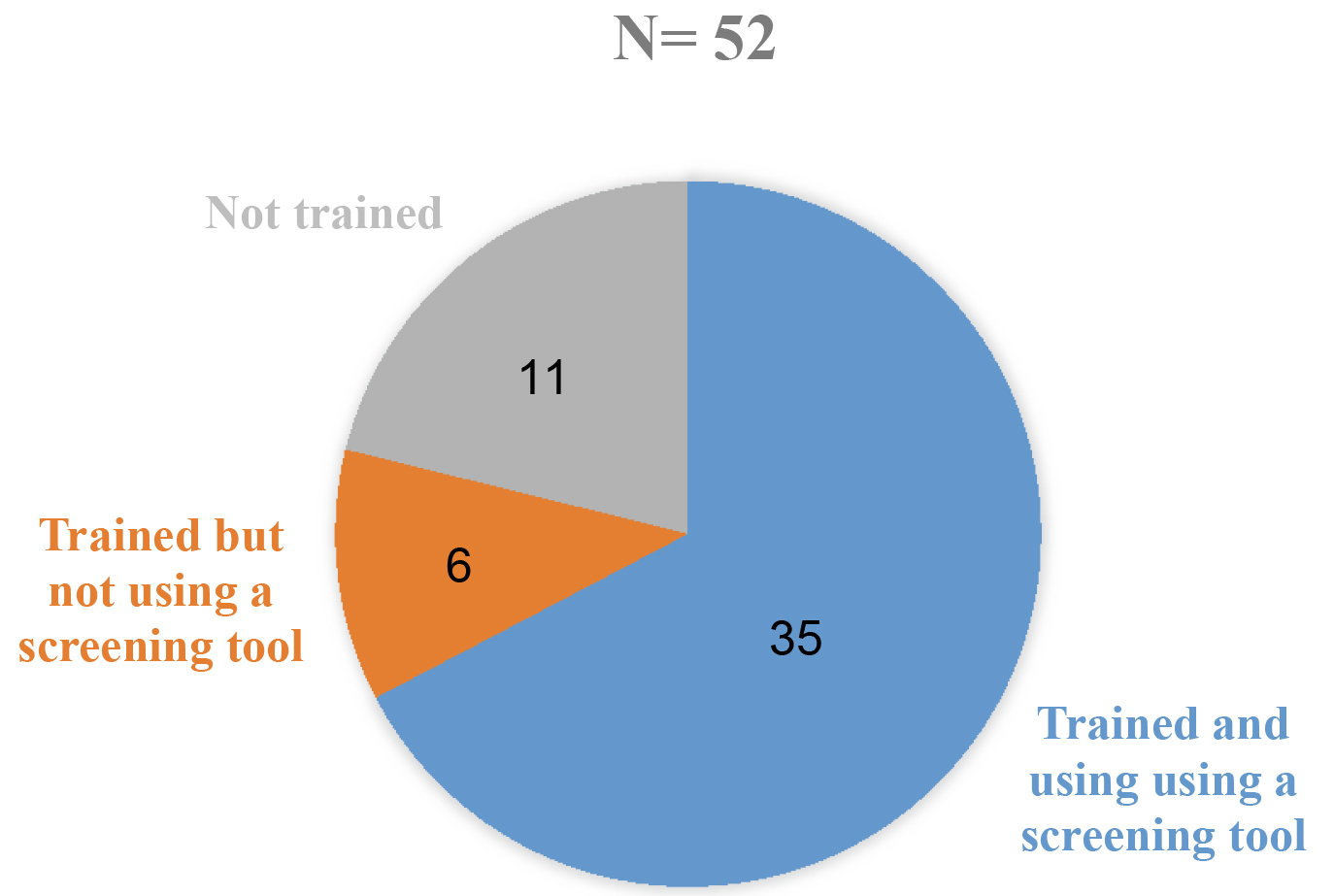
The most common facilitators reported were expertise (55.8%), scope of practice (53.8%), and specialist referrals (50%) (Table 3). Participants believed that parental awareness and input simplifies the screening process, sometimes even facilitating early identification and intervention.
“They [parents] are looking out, ‘my child is not speaking by age of one and half year’. They compare with other kids and come in early for identification. And that becomes a facilitator.”
Tertiary care set up, research orientation, interdisciplinary cooperation, and communication were also important facilitators that were identified.
“Because we have a set-up of speech therapy, occupational therapy, so we do get cross reference from these units.”
The most common barriers cited by participants were time availability (69.2%) followed by training cost for certification (59.6%), cost of procurement of tool (57.7%), and staff adequacy (48.1%) (Table 3). However, participants expressed that delayed referral, dependency on referral, lack of comprehensive tools, irregular follow-ups, private practice, lack of facility, and unreliable informants were also hindering timely and periodic screening. Participants also believed that screening within the critical period of development had a better prospect of improving the developmental outcome. However, in most of the cases, children were not referred to them on time.
“Many times what happens is that they (pediatrician) say ‘let’s wait’. That school of thought is there ‘let’s wait, it will happen over a period of time’. So many a times even if they are identified early, it’s not tapped for providing treatment. So that’s one main barrier.” “The children with neuromotor delay detected at 8 months to children detected at 2 months, there is a considerable difference in their neuromotor abilities.”
One participant cited lack of interprofessional communication as a barrier: “Communication between various allied health professionals and pediatricians is limited.”
Some factors such as interdisciplinary cooperation and communication, parental awareness, and professional awareness were identified as both barriers and facilitators by the respondents.
“Their support and their awareness regarding developmental screening is very important; there is not a single scale which gives me comprehensive picture; if we suspect that a patient is having developmental delay, we usually send him to institution (tertiary care set up) for further investigation and management. We don’t have the facility to manage patients with developmental delay; many times, the parents overrate the ability of the child.” “Most of the time the parents would be coming to us after a reference from the pediatrician or developmental neurologist. So, unless and until they (pediatrician or developmental neurologist) have an interest in developmental screening, it is very difficult to do screening.” “One is the knowledge at the level of pediatrician to do a developmental screen, especially when it is from the communication domain, many times what happens is that they say ‘let’s wait’. So, even if they are identified early, it’s not tapped for providing treatment. So that’s one main barrier. Next, awareness itself is poor, not only among the parents but also at the level of professionals.”
Themes related to overcoming barriers were weekend clinics, screening during immunization, and the need for interdisciplinary collaboration, child-centered practice, and curriculum. One participant suggested that, considering a large number of working parents, organizing a weekend clinic would benefit them: “Most of the parents are working. So, sometimes they call and ask us – are you open on Sundays.” Another participant suggested that children with probable developmental delay could be followed up during immunization appointments: “We usually tell them to come for immunization clinic, come for the follow up”. One participant emphasized the need for interdisciplinary collaboration: “Cooperation among the different departments is also important because we have a setup of speech, occupational therapy, so we do get cross reference from these units. So harmony among these departments is necessary.” One participant responded that the practice of developmental surveillance and screening should address parental concerns and focus on child development: “Final goal of the entire team should be to help the parents and the child”. The health professions’ curriculum should include developmental surveillance and screening: “Undergraduate level and post graduate level program should also ensure that therapist is also trained”.
Successful implementation of developmental screening depends on the knowledge and attitudes of various health care professionals. As observed in this study, 78.8% of participants were trained in administration of a standardized developmental screening tool and 67.3% were currently utilizing a screening tool in their practice. The study participants had fair to good knowledge related to the use of developmental screening tools and guidelines. These tools could be associated with the fact that majority of participants were from a medical college-associated, tertiary care set up, with 48.1% of them having a post-graduation or doctoral qualification with an orientation towards academics and research. A previous study (Morelli et al., 2014) had reported that lack of knowledge regarding screening tools and the process of their administration, scoring, and interpretation was a barrier [17].
The results revealed a favorable attitude towards screening using standardized screening tools. The majority of participants believed that children, irrespective of risk of developmental issues, should also be followed up regularly with standardized developmental surveillance and screening tools. This resonates with the recommendations of the American Academy of Pediatrics. The study results are consistent with a study by Thomas et al. in 2012 that compared detection of delays by surveillance with formal screening and found that periodic formal screening is necessary in addition to systematic surveillance alone [20].
The most common barrier to developmental screening according to the study participants was lack of time availability as screening tools are not quick to administer and are time intensive. Thus, it may affect the practice of regular use of screening tools leading to the professionals relying mainly on developmental surveillance rather than periodic screening with a standardized screening tool [17]. A study by Glascoe et al. in 2015 advocates opportunistic screening beyond well child visits, the use of web-based parent-completed screening tools such as Ages and Stages Questionnaire (ASQ) and Parents’ Evaluation of Developmental Status (PEDS), telephonic follow-up, and the establishment of a repository of referral resources as well as collaborative partnerships. These various screening tools help to overcome the limitation of time availability [21, 22].
Ninety-six percent of participants agreed that parental input is important for early identification and intervention. This result is supported by several studies advocating parental concerns as predictors of early identification of developmental problems [23, 24, 25]. However, only 17.3% of the study participants utilized a parent reported developmental screening tool in their set-up. This finding can be attributed to professionals’ perception that parental input is biased with concerns either over- or under-estimating the capacities of the child. This belief that parents lack knowledge of normal child development directs professionals to rely more on profession-initiated screening tools [17].
The present study has taken into consideration the perspectives of various health care professionals in implementation of developmental surveillance and screening. It establishes the facilitators and barriers towards developmental surveillance and screening in Indian context. Also, it will help in evolving strategies to encourage implementation and adherence to the practice of developmental screening using standardized tools. The study participants emphasized the need for interprofessional collaboration to improve the referral process. Several other studies emphasize the roles of various health care professionals in optimizing developmental outcomes and quality care [26, 27]. School-based screening programs, parental education through mass media, integration of screening programs with well-baby clinics or weekend clinics, and the inclusion of mandatory training of professionals for administration of standardized screening tools in undergraduate and postgraduate courses are other strategies emphasized by the study participants. Such strategies were deliberated by other studies [28, 29, 30]. The outcomes of this study imply the need for a comprehensive developmental surveillance and screening program integrated with the national RBSK program in providing early intervention services for children at risk of developmental delay.
In addition, the present study has some limitations. Majority of the participants had affiliation to a tertiary care set-up with a drive towards academics and research. It was situated in a small town of Southern India receiving a large quantum of patient referrals. There was unequal distribution of participants of various professions involved in this study. Further, the government health care set ups were not involved. Thus, the findings of this study cannot be generalized to other Private and Government aided health care set ups where the practice contexts might be different. A larger knowledge, attitude and practice survey on developmental surveillance and screening practices among health professionals across India in various health care set-ups will provide more insights.
Conclusion
The study concludes that the pediatric health care professionals have fair knowledge on developmental surveillance and screening. They have a favorable attitude and practice of standardized developmental screening tools. However, in Indian context, practice is largely dependent on organizational set up and is hindered by certain barriers. The emergent themes can be utilized as facilitators to formulate better strategies to improve the practice of using standardized developmental surveillance and screening tools for early identification of developmental delay.
Footnotes
Acknowledgments
The investigators thank the administrators of healthcare settings for necessary permission and all respondents of the survey and the interview in providing their expert opinion.
Conflict of interest
The authors have no conflict of interest to report.