
Abstract
PURPOSE:
To investigate foot and ankle somatosensory function in children with cerebral palsy (CP).
METHODS:
Ten children with spastic diplegia (age 15
RESULTS:
Children with CP demonstrated significantly higher light touch pressure and two-point discrimination thresholds compared to their TD peers. Individuals with CP perceived the vibration stimulus for a longer period compared to the TD participants. Finally, the CP group demonstrated significant impairments in joint position sense but not in kinesthesia of the ankle joints.
CONCLUSIONS:
These findings suggest that children with CP have foot and ankle tactile and proprioceptive deficits. Assessment of lower extremity somatosensory function should be included in clinical practice as it can guide clinicians in designing more effective treatment protocols to improve functional performance in CP.
Keywords
Introduction
Cerebral Palsy (CP) is the most common pediatric neurological condition that results in physical disability, and is caused by a static lesion in the developing fetal or infant brain [1]. The most prevalent type of brain injury in CP is periventricular leukomalacia, a condition associated with corticospinal pathway injury that is believed to be the primary cause of motor deficits in this population [2]. Traditional rehabilitation approaches in CP are generally motor-centric, focusing on techniques to ameliorate musculoskeletal and motor impairments. Less attention has been paid to deficits in sensory systems that could negatively influence the feedback and feedforward control mechanisms, which potentially shape motor behavior. The American Academy of Pediatrics has reported that there is no universally accepted framework for the diagnosis of sensory processing impairments in those with developmental disorders, resulting in treatment plans of limited effectiveness [3]. Further, clinicians lack confidence in their ability to accurately identify sensory deficits in children with neurological disorders due to the absence of reliable sensory assessments tools, although they acknowledge the importance of these assessments [4].
Sensory deficits have been attributed primarily to injury of the underdeveloped brain and secondarily as a result of motor impairments [5]. Specifically, reduced physical activity may limit opportunities for learning and perceptual development experience in CP [1, 5]. In addition, studies have identified somatosensory impairments in light touch pressure [6, 7], two-point discrimination [6], stereognosis [6], vibration [7], and proprioception [7, 8]. Some of the aforementioned studies have reported tactile deficits [6, 9] that have been associated with impaired manual performance [6] and precision grip tasks [9] in the affected hand of individuals with hemiplegia. This suggests an essential link between somatosensory information and motor performance in upper extremities.
In light of the above discussion, little research has examined lower extremity (LE) somatosensation in CP [7, 8]. McLaughlin et al. [7] demonstrated that LE pain sensation, position sense, and direction of scratch are diminished in a group with spastic CP. Yet, each of the tested sensory modalities were only documented with a “pass or fail” score and therefore lack important information regarding the deficit magnitude [7]. Additionally, Wingert et al. [8] reported transverse plane hip proprioception deficits in CP that were related to increased postural sway and decreased gait speed [10]. Less is known about ankle proprioception as well as plantar cutaneous feedback deficits, although distal LE impairments are more prevalent and severe than proximal impairments in spastic CP [11].
In the present study, we investigated the magnitude of foot and ankle tactile and proprioceptive deficits in children with spastic diplegia and compared their results to typically developing (TD) age-matched peers. We hypothesized that somatosensory ability would be diminished in the CP group compared to the TD one. Quantifying the nature and extent of somatosensory impairments in CP could potentially assist in developing a comprehensive LE sensory tests battery that will lead to improved identification of body function impairments, and thus guide therapeutic management in CP.
Methods
Participants
A convenience sample of ambulatory individuals with spastic diplegic CP aged 8–18 years old and age-matched healthy subjects participated in this case-controlled study. Participants with CP were primarily recruited at Shriners Hospitals for Children (SHC) in Philadelphia. Other means of contact to recruit both children with CP and healthy controls included recruitment letters and fliers. Individuals with CP were classified as levels I–III on the Gross Motor Functional Classification Scale (GMFCS), did not use any orthotic device on a regular basis, and were able to stand without assistance for at least 2 minutes. The exclusion criteria for this group comprised receipt of botulinum toxin injections in the last 6 months, a LE score of 4 on the modified Ashworth Scale, and previous selective dorsal root rhizotomy. Participants also had to report: no LE surgery or trauma in the year prior to participation, no prior history of LE joint instability, no uncorrected visual impairments, and no hearing or vestibular deficits. Parents or legal guardians and subjects 18 years of age signed informed consents. Participants under 18 years of age signed informed assent documents prior to participation. The study was approved by the Western Institution Review Board (IRB) and the IRB of Temple University and the University of Delaware.
Procedure
Each participant underwent a comprehensive somatosensory clinical test battery to assess tactile and proprioceptive function. For light touch pressure, two-point discrimination, vibration sensation, and joint position sense assessments, each subject laid down comfortably on an exam table. Kinesthesia was tested in the seated position. Additionally, to be able to test for joint position and kinesthesia, all the participants were able to move their ankle joint from neutral to 30–40 degrees of plantarflexion. All assessments were administered in random order by the same examiner using standardized instructions. Specifically, for each participant a different random order for each test was generated. For each test, the assessor explained the procedure and then the participants performed a practice trial with visual feedback before the test was administered. Actual tests were performed without visual feedback, and took approximately one hour to complete.
Measures
Light touch pressure was assessed on the plantar surface of each foot by using the 6-item Monofilaments kit (Baseline
Two-point discrimination was assessed on the plantar side of the foot by using an aesthesiometer (Baseline
Vibration sensation was evaluated by using a 128 Hz tuning fork (Martin Tuttlingen, Germany) over the first metatarsal head and medial malleolus bilaterally. The assessor struck the tuning fork on a rubber padded surface located next to the participant’s feet to elicit a strong movement in the prongs. Then, the tuning fork was positioned perpendicular to the skin on the predefined bony prominences. The duration of the vibration stimulus was recorded by a chronometer, starting from the activation time of the tuning fork until the participant reported that he/she could not feel it. The average time(s) of the three trials for each site was used for the analysis.
Joint position sense was assessed with the participant lying prone on the exam table with their knee flexed in 90 degrees and the ankle joint in neutral position. A digital goniometer (Medigauge, Westford, MA) was used to measure the ankle angle displacement during testing. Initially, the tested foot was passively moved by a physical therapist to a specific joint angle (i.e., target joint angle: 20 deg of plantarflexion), held in this position for 3 seconds, and then returned to the neutral position. Next, the subject was instructed to actively reproduce the position as accurately as possible. The procedure was repeated 3 times per side (left and right). The magnitude of error between the performance and target joint angle was recorded at the nearest degree for each trial. The average of 3 trials was computed for analysis.
Kinesthesia was evaluated while the participant was seated with the ankle joint in neutral postion. The tested foot was grasped on its lateral and medial edges and the ankle joint was then passively plantarflexed or dorsiflexed in a random order. Participants were asked to instantly report the direction of the displacement. Performance accuracy was determined as the number of correct responses out of 10 trials (5 in each direction) and was converted to a percent value.
Statistical analysis
All data were analyzed by using SPSS (version 23; SPSS Inc., Chicago, IL). Data normality was examined by visual inspection of Q-Q plots and by conducting the Shapiro-Wilk test. Demographic data (age, height, weight, body mass index) were normally distributed and analyzed with two-tailed independent samples
Demographic characteristics of children with cerebral palsy and their typically developing peers. Means and standard deviations (in parentheses) are presented in the table
Demographic characteristics of children with cerebral palsy and their typically developing peers. Means and standard deviations (in parentheses) are presented in the table
Somatosensory assessment scores (median and interquartile range [IQR]) in children with cerebral palsy (CP group) and children with typical development (TD group). Ankle joint position sense error data were normally distributed and presented as means with
Box plots of the light touch pressure thresholds at the first metatarsal head, fifth metatarsal head, and heel application sites for children with CP and TD children. The white dots within the boxes correspond to the group’s median, the boxes indicate the first and third quartile, and the whiskers the 95% confidence intervals around the median. In the TD group (grey box-plots), the 95% confidence intervals are within the interquartile range; therefore, no whiskers are shown. Asterisks correspond to significant differences between the groups (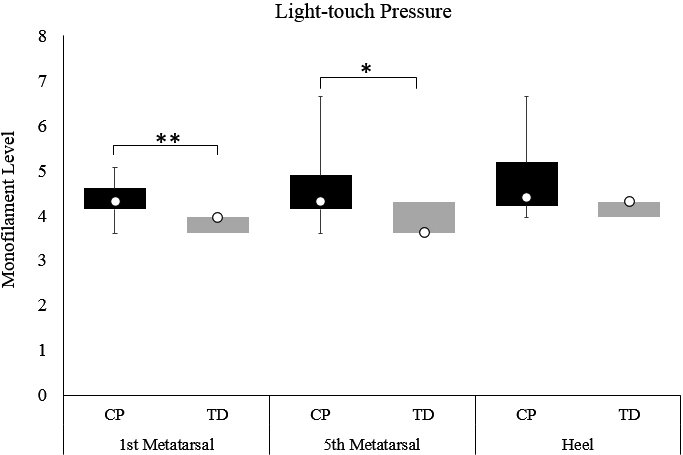
Box plots of the two-point discrimination thresholds at the forefoot and heel application sites for children with CP and TD children. The white dots within the boxes correspond to the group’s median, the boxes indicate the first and third quartile, and the whiskers the 95% confidence interval of the median. In the TD group (grey box-plots), the 95% confidence intervals are within the interquartile range; therefore, no whiskers are shown. Asterisks correspond to significant differences between the groups (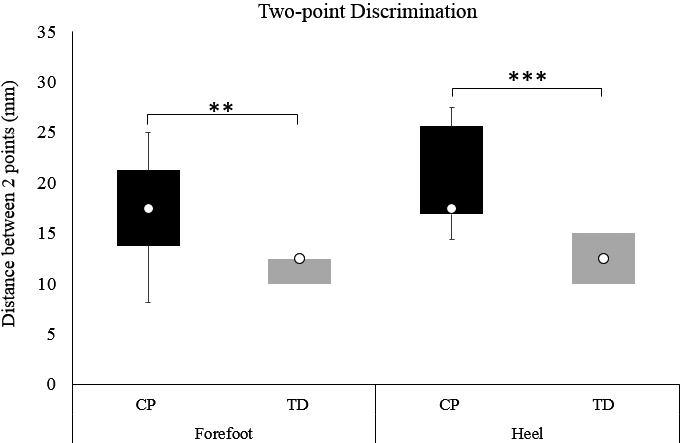
Box plots of the vibration scores at first metatarsal and medial malleolus for children with CP and TD children. The white dots within the boxes correspond to the group’s median, the boxes indicate the first and third quartile, and the whiskers the 95% confidence intervals around the median. In the TD group (grey box-plots), the 95% confidence intervals are within the interquartile range; therefore, no whiskers are shown. Asterisk correspond to significant differences between the groups (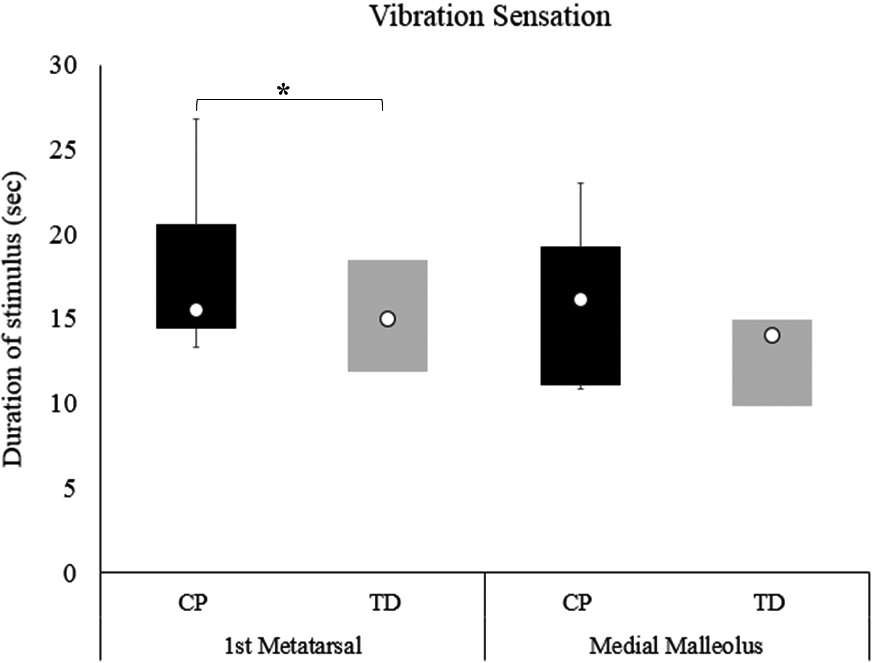
Means (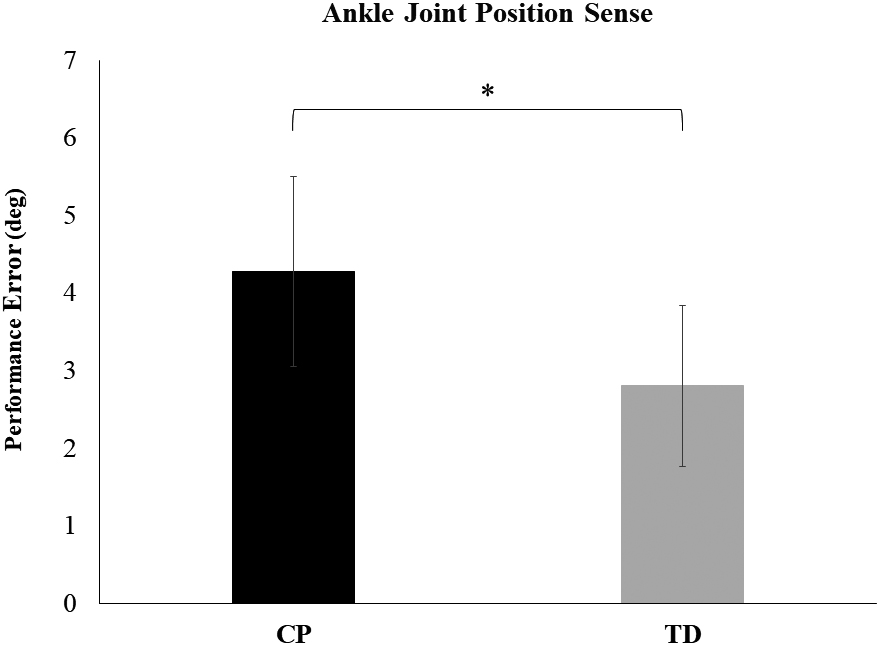
Participants’ demographic characteristics are presented in Table 1. Age, sex, height, weight, and body mass index were not significantly different between the two groups (
Compared to the TD group, the group with CP demonstrated statistically significant worse scores in all the somatosensory assessments except kinesthesia, thus suggesting sensory impairments. Particularly, light touch pressure thresholds were significantly higher for individuals with CP at the first and fifth metatarsal head of the feet than for TD participants (first metatarsal: U
A Mann-Whitney test indicated that the distance between the two perceived points for the two-point discrimination was greater for children with CP (Median
Individuals with CP perceived the vibration stimulus for a longer time period compared to TD participants. However, this difference was statistically significant only for the first metatarsal site (U
An independent samples
Discussion
The objective of this study was to explore the magnitude of foot and ankle somatosensory deficits in children with CP compared to TD controls. Our findings indicated diminished tactile and proprioceptive ability in the CP group. Specifically, plantar light touch pressure and two-point discrimination, vibration at the first metatarsal site, and ankle joint position sense were significantly impaired in children with spastic diplegia. Appropriate somatosensory feedback is a critical component of refined motor performance in light of evidence that somatosensory deficits are related to poor balance and motor function in CP [13]. Overall, sensory assessment in CP may help define individual-specific deficits and lead to more effective clinical treatment approaches.
This study is the first to demonstrate that children with spastic diplegia have higher plantar cutaneous thresholds, suggesting foot tactile impairments relative to their age-matched TD peers. Similarly, increased foot tactile sensation thresholds have been reported in individuals with peripheral nervous system disorders like diabetic neuropathy [14], Charcot-Marie-Tooth type 2 [14], and multiple sclerosis [12] which have been linked to impaired balance. Our results showed diminished light touch sensation in the forefoot and decreased two-point discrimination in both the forefoot and heel of the foot. These two plantar foot areas are crucial during upright stance [15]. Particularly, the forefoot site contributes to the forward propulsion during the push-off phase of gait, while the heel provides important neural input regarding the initiation of the stance phase of gait. Decreased cutaneous information in these areas is associated with increased postural sway during unperturbed stance [16] and altered kinematics and muscle activation patterns during gait [17]. We speculate, therefore, that poor postural control performance in children with CP can be attributed partially to their foot tactile deficits.
Another interesting finding is that all participants with CP were able to perceive the vibration stimulus. Previous research suggested that children with CP were unable to correctly identify the vibration stimulus in their LEs [7]. In this study, the duration of the perceived vibration stimulus was longer in the CP group compared to controls. Higher vibration perception thresholds have been reported in knee osteoarthritis [18] and diabetic polyneuropathy [19], suggesting sensory impairments in the LEs with increased risk of falls and fall-related injuries. Conversely, children with an idiopathic toe walking gait showed increased sensitivity in vibration perception at the hallux due to sensory processing deficits that potentially resulted in the toe walking pattern [20]. Hence, vibration should be explored further in CP in order to provide a clearer understanding of vibratory function and how its deficit affects motor performance.
The children with CP displayed significantly larger error in reproducing the target ankle position compared to the TD participants, although the mean error difference between groups was only 1.7 degrees. Hip joint position sense errors of similar magnitude were significantly correlated with increased center of pressure and mass sway during quiet stance and decreased gait velocity in CP [10]. Interestingly, when kinesthesia was tested no differences were detected between the two groups. Previous studies have reported joint position sense deficits in the hip and knee joints [7, 8], whereas hip joint kinesthesia was not affected in CP [8]. One potential reason is that detecting the direction of movement, as required by the kinesthesia test, is a simpler task compared to the joint position test [8]. Another possible explanation is that despite grasping the foot on its medial and lateral edges during testing, sensory inputs from the pressure receptors in these areas may have contributed to the participants’ ability to detect the direction of movement. Further, the applied pressure, albeit minimal, is still higher than the pressure applied from monofilaments and the aesthesiometer during the testing for somatosensory deficits detection. Overall, the joint position sense test may be a better method to detect proprioceptive deficits in children with CP who have mild to moderate motor impairments in clinical settings.
Somatosensory feedback is crucial for balance control [15, 21, 22] and in view of our clinical findings, it appears that children with spastic diplegia exhibit diminished foot and ankle somatosensory function. The interplay of the tactile and proprioceptive somatosensory signals allows for a stable posture [15] and gait [17]; therefore, the observed deficits can potentially affect balance resulting in poor performance during functional activities, increased risk for falls, and higher levels of caregiver dependence [23]. These findings provide the impetus for future studies to further investigate the relationship between distal LE somatosensation and postural control in CP.
A limitation of this study is its small sample size. Yet, our data demonstrated statistically significant differences between the CP and TD groups in several of the somatosensory measures. As a next step, it is important to investigate if this statistically significant difference is also clinically important. Determining the minimal clinically important difference would provide insights on what children with CP perceive as meaningful and beneficial and, therefore, can guide the design of the therapeutic protocol by clinicians.
In this study, we utilized a simple battery of sensory tests that are traditionally used in the clinic to determine sensory function in individuals with neurological disorders. Although these clinical tests are easily administered and use low-cost instruments, their reliability has been previously questioned as there was a lack of control on how much force is applied to the instruments by the assessor during testing [24]. However, recent findings support that these tests are reliable and valid for use in the clinic [25, 26, 27]. More comprehensive and standardized assessments for LE somatosensation can complement these traditional clinical tests and provide us with a better understanding of how severe somatosensory deficits are in children with CP.
Another limitation pertains to how the joint position sense test was performed. Specifically, a goniometer was used to evaluate performance error, thus introducing variability in joint angle measurements. To improve the test’s accuracy, the same physical therapist performed three consecutive trials of the test and recorded the average performance error for each subject. Additionally, this test does not differentiate between proprioceptive and potential motor control deficits that are prevalent in CP. However, it is common to utilize both joint position sense and kinesthesia tests to demonstrate proprioceptive impairments in this population [8, 28]. In this study, although we did not assess motor control deficits, all participants were able to move their ankle joint independently from neutral position to at least 30 to 40 degrees of plantarflexion while the target ankle angle was set at 20 degrees. Therefore, participants were able to actively move the tested foot when instructed, indicating absent or minimal motor control impairments. Taken together with these limitations, our findings should be interpreted carefully.
Conclusions
Ambulatory children with spastic diplegia exhibited decreased foot tactile and ankle proprioceptive function compared to their age-matched TD peers. These findings confirm that somatosensory impairments are prominent in CP not only in upper extremities but also in the LEs, and may be associated with decreased postural control performance [10]. Using a simple and cost-effective battery of sensory tests in daily clinical practice may allow for the detection of LE somatosensory deficits. Identifying these impairments can assist clinicians in designing more effective rehabilitation protocols by combining motor learning strategies with sensory facilitation techniques. Additionally, this may have important practical implications due to the presence of existing evidence that these approaches can enhance somatosensation and improve postural control in CP [29].
Footnotes
Acknowledgments
This research project was conducted in partial fulfillment of the requirements for the Ph.D. dissertation of Anastasia Zarkou (Biomechanics and Movement Science Program, University of Delaware, Newark, DE). This study was supported by Shriners Hospital for Children (grant: 22173) to JJ (Primary Investigator) and partially supported by the Onassis Foundation to AZ.
Conflict of interest
The authors have no conflict of interest to report.