
Abstract
PURPOSE:
To describe clinical data, rehabilitation services, and outcomes of children with handedness switching as their presenting symptom before low-grade glioma (LGG) diagnosis.
METHODS:
A retrospective chart review was performed for five patients (four female and four white) with LGG and confirmed handedness switching before LGG diagnosis.
RESULTS:
All children were less than 8 years at diagnosis, and two patients were less than 3 years. All children were initially right-handed and experienced loss of motor function, ranging from weakness to paresis, in their dominant hand. The median time from switching handedness to diagnosis was 1 month (range: 0.75–60 months). Rehabilitation was offered for three patients, and motor function deficits in the initial dominant hand were resolved in two of the total cohort. At long-term follow-up, hand dominance returned to the initial hand in three patients.
CONCLUSIONS:
Handedness switching should be acknowledged as a potential sign of LGG in children, and early long-term rehabilitation services should be offered for these children.
Introduction
Neural plasticity (NP) can be defined as the brain’s ability to be molded or programmed by experience, capacity to learn and remember, and ability to reorganize and recover after injury [1]. The term plasticity was first used by William James in 1890 to describe the changes in neural paths that establish habits [2]. In 1906, Ernesto Lugaro suggested that chemotropic activities promote new synaptic functions [3]. The Kennard Principle, which links age to plasticity, states that young age imparts a plasticity privilege, resulting in fewer problems and better recovery after brain injury in children than in adolescents or adults [4]. NP can result in adaptive or maladaptive outcomes, depending on the equilibrium between plasticity and homeostasis [2]. Therefore, understanding this phenomenon and the factors influencing it may help to predict functional outcomes and determine the best treatment or rehabilitation modalities for children with various neurologic conditions characterized by impaired or lost function.
Although young age and developmental immaturity are associated with greater NP, disorders that affect the signaling of synaptic membranes in children, such as neurofibromatosis type-1 (NF1), tuberous sclerosis, and fragile X syndrome, exhibit impaired plasticity. Consequently, these disorders are used to identify the pathways involved in plasticity [5]. The corpus callosum plays a crucial role in interhemispheric interactions and maintains independent processing, as well as communication between both hemispheres [6]. It is hypothesized that factors affecting NP exert their influence through motor interhemispheric interactions [4, 7]. Several studies have also shown that noninvasive brain stimulation alters interhemispheric interactions by decreasing the excitability of the stimulated motor cortex, thus leading to reduced interhemispheric inhibition from the stimulated motor cortex over the nonstimulated motor cortex [8, 9].
Low-grade gliomas (LGGs) are slow-growing tumors associated with excellent outcomes but may remain undiagnosed for many years. If LGG tumors are incompletely resected, multiple recurrences requiring several treatment modalities may occur. The chronicity of LGG tumorigenesis, coupled with insidiously developing neurologic dysfunction, may potentially invoke NP [10]. In a previous study of delayed diagnosis of brain tumors in children, five children were noted to have experienced handedness switching before LGG was diagnosed [10]. A similar phenomenon has also been observed in adults [11, 12]. To create awareness of handedness switching in children as a presenting symptom of LGG, these five pediatric cases are described in detail, including clinical data and treatment modalities. In addition, the optimal treatment modalities and rehabilitation services needed to improve the quality of life of patients with LGG, who are expected to survive for a long time, are discussed [10, 13].
It should be noted that while in adults evaluating handedness can be performed easily by using questionnaires and noting which hand is used to perform certain skills, this process in young children is especially complicated as such questionnaires are difficult to apply [14]. In addition, the development of adult-like handedness is not well established until the age of 6 [14, 15].
Patients and methods
Retrospective chart reviews of five patients with LGG and confirmed handedness switching before LGG diagnosis were performed. This study was approved by the Institutional Review Board of St. Jude Children’s Research Hospital, which waived the requirement for informed consent. For each patient, we obtained date of birth, sex, age, race, existing symptoms, duration of symptoms, presence of NF1, initial imaging, extent of resection, treatment modalities (chemotherapy regimens and/or radiation therapy), history of relapse, and clinical status at last encounter. We also collected rehabilitation data for each patient. The brain imaging studies were reviewed by an expert neuroradiologist. Pathology findings for all cases were confirmed at St. Jude Children’s Research Hospital, and LGG diagnoses were extracted from the pathology reports. Date of diagnosis was defined as the date of the first imaging after initial presentation. Duration of symptoms was determined as previously described [10]. Handedness was determined based on parents’ reports.
Results
Patient characteristics
All tumors were histopathologically identified as pilocytic astrocytomas. Four patients were female, four were white, and one was African American. All children were less than 8 years at diagnosis, and two patients were less than 3 years. The median age was 51 months (range: 23–93 months), and the median time from switching handedness to diagnosis was 1 month (range: 0.75–60 months). None of the patients were noted to have a predisposing genetic condition or congenital neurologic disorder. Tumors were in the right cerebellar hemisphere in two patients (with involvement of the corpus callosum in one patient), in the left thalamopeduncular area in two patients, and in the left deep cerebral hemisphere involving the left optic pathway and thalamus in one patient (Figs 1 and 2). Recurrences occurred in three patients. One patient experienced a relapse within 3 months of diagnosis, and the second within 2 years. The third child suffered a first relapse within 4 years and three additional recurrences during the course of the disease. None of the patients had metastatic disease, and all relapses were local.
Axial nonenhanced T1-weighted (A) and T2-weighted (B) images of an optic-hypothalamic glioma involving the left thalamus. The lesion exerts compression on the pyramidal tracts at the level of the posterior limbs of the internal capsules.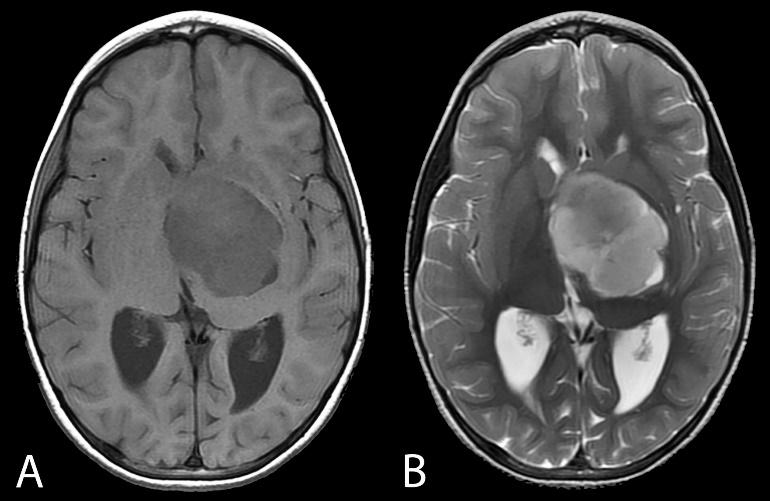
Axial nonenhanced T1-weighted (A) and T2-weighted (B) images of a voluminous, dominantly cystic right cerebellar tumor (juvenile pilocytic astrocytoma). The mass effect in the posterior fossa results in compression and deformity of the brainstem. 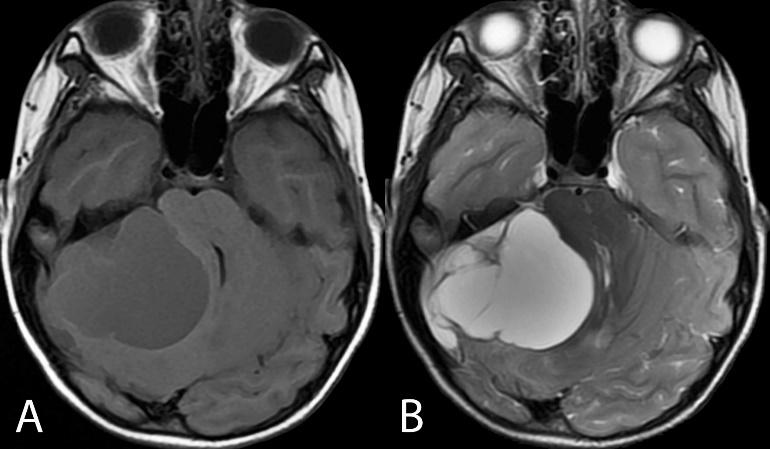
All children were initially right-handed and experienced loss of motor function, ranging from weakness to paresis, in their dominant hand (Table 1). Rehabilitation was offered for three patients. One patient experienced improved paresis to almost normal function but continued to prefer using the nondominant hand. At long-term follow-up, motor function deficits in the initial dominant hand were resolved in two patients (information was not available for an additional patient), and hand dominance returned to the initial hand in three patients.
Discussion
This report describes a small series of children with LGG who demonstrated handedness switching before diagnosis. Although, switching handedness is not usually described as a symptom of brain tumors in children, primary health care providers should consider the possibility of an indolent LGG in their differential diagnoses for children with an unexplained change in hand preference. Further evaluation by a neurologist and a diagnostic imaging workup should be sought in these cases. To our knowledge, only one study has addressed handedness switching as an atypical presentation in children with brain tumors, potentially causing delayed diagnoses [16]. In this study, Yokoi et al. described three cases of brain tumors, with only one case of LGG. Interestingly, in an educational article, Crawford described the early changing of handedness or even early presentation of handedness as a sign that may be missed in children with brain tumors [17].
Slow-growing lesions are highly associated with more efficient plasticity in animals and humans than are acute lesions [11]. LGGs, as slow-growing neoplasms, are also known to affect brain function reorganization, even in adult populations [12, 18, 19, 20]. In a study by Almairac et al. [19], structural magnetic resonance imaging revealed that 84 patients with insular LGG (47 in left insula and 37 in right insula) experienced increased gray matter volume in the contralateral insula. In another study by Traut et al. [18], functional plasticity in language was demonstrated with magnetoencephalography. This ability of the brain to reorganize crucial functions can be used to optimize resection extent for LGG tumors. Picart et al. [20] reported that well-demarcated cortical tumors exhibit a better extent of resection and functional recovery after a second surgery. Because most childhood LGG tumors are not diffuse, this may have important implications in surgical interventions for children with LGG.
Because young age is associated with greater plasticity [4, 7], pediatric LGG is a potentially ideal model for studying spontaneous NP in children. In addition, children with LGG are expected to survive for decades [10, 13, 21] but suffer many neurologic deficits over the course of their lives [21]. Therefore, it is important to consider rehabilitation services for these children as early and as long as possible to recover some of their functionality and improve their quality of life. Constraint-induced movement therapy in 10 children with brain tumors (four were pilocytic astrocytoma) was previously shown to be both feasible and beneficial [22]. In a study of 10 children with cerebral palsy, constraint-induced movement therapy was associated with structural remodeling in gray matter [23], suggesting that aggressive early and long-term rehabilitation therapy is justified for children with LGG and other chronic conditions.
Handedness and rehabilitation of pediatric patients with low-grade glioma
Handedness and rehabilitation of pediatric patients with low-grade glioma
Footnotes
Acknowledgments
This study was supported by grant funding from ALSAC and grant CA21765 from the National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors acknowledge Nisha Badders, PhD, for the scientific editing of the manuscript. This work was presented in part at the 17th International Symposium on Pediatric Neuro-Oncology (ISPNO) in 2016 as a poster presentation.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.