
Abstract
PURPOSE:
We explored the test-retest reliability of pelvic rotation measured using a smartphone and established criterion-related validity by analyzing simple linear regression between pelvic rotation data obtained using the smartphone and those measured by a palpation meter.
METHODS:
We recruited 12 children with cerebral palsy (CP) (7 boys and 5 girls) and measured pelvic rotation using a smartphone application and a palpation meter in the sitting, standing, and one-leg standing positions. Test-retest reliability was evaluated by calculating intraclass correlation coefficients (ICCs); simple linear regression was analyzed to explore the relationships between smartphone and palpation meter data.
RESULTS:
In terms of the test-retest reliability of pelvic rotation measured by the smartphone, the ICCs ranged from 0.85 to 0.95. A positive linear correlation was found between smartphone and palpation meter data.
CONCLUSIONS:
We confirmed that measurement of pelvic rotation using a smartphone was reliable when children with CP were in the sitting, standing, and one-leg standing positions. In addition, pelvic rotation measured using the smartphone correlated significantly with that measured using a palpation meter.
Introduction
Pelvic rotation is closely associated with both trunk motion and lumbar spine curvature [1]. When the pelvis is rotated anteriorly, lordosis of the lumbar vertebrae increases in the sagittal plane; when the pelvis is rotated posteriorly, lumbar kyphosis increases [2]. Pelvic asymmetry is associated with changes in trunk posture, scoliosis [3], increased lumbar spine stress [4], and leg length differences [5]. In children with cerebral palsy (CP), the pelvis is excessively tilted posteriorly when sitting and excessively tilted anteriorly when standing [6]. Additionally, physical activities such as sitting and standing are limited by excessive pelvic rotation [6, 7]. Therefore, it is important to measure pelvic rotation in children with CP.
Pelvic rotation is frequently assessed in the sitting, standing, and one-leg
standing positions in ambulatory children with CP since these postures are all adapted when
performing daily activities [8, 9, 10]. A palpation meter
is frequently used to obtain pelvic rotation data which are reliable when recorded in
healthy adults [9]. Krawiec et al. [11] investigated the reliability of a palpation meter
on 24 male and 20 female collegiate athletes. Test-retest reliability was reported as
The minimal detectable change (MDC) is the smallest difference detectable above
the measurement error [12]. Azevedo et al. [9] studied the MDC of measuring pelvic rotation using
a palpation meter. The MDC of pelvic rotation ranged from 1.5
Methods
Children
We recruited 12 children with CP (7 boys and 5 girls, mean age, 9.0
Examiners
A single examiner with 7 years of experience in pediatric physical therapy performed all measurements. To reduce measurement error, the examiner was trained in pelvic rotation assessment in the sagittal plane by a senior researcher with 20 years of experience in pediatric physical therapy.
Apparatus
The palpation meter featured an angle-level inclinometer with a magnetic
base and two caliper arms (Acuangle; Isomed, Portland, OR, USA). The device was 93 mm long
Pelvic rotation data
Pelvic rotation data
SDs: standard deviations.
The flow chart for pelvic rotation measurements.
All children participated on two occasions (test occasion, T1; retest
occasion, T2), which were two weeks apart. Pelvic rotation in the sagittal plane derived
using both the palpation meter and the smartphone was obtained with participants in each
of three positions (sitting, standing, and one-leg standing). For examining pelvic
rotation, the children were asked to sit on a therapeutic table with thigh support,
without back and feet support, and also were to assume a comfortable or preferred sitting
position according to Bigongiari’s protocols [13]. When standing, the children were asked to stand with their feet aligned at
shoulder width and to look at a red dot attached to a wall 2 m distant, to reduce trunk
sway. In the one-leg standing position, the children were asked to stand with the dominant
leg on the floor and to maintain the opposite hip at 45
Statistical analysis
PASW software (ver. 20; Norusis/SPSS Inc., Chicago, IL, USA) was used for
all statistical analyses. Statistical significance was defined by a two-tailed
The test-retest reliability, standard error of measurement (SEM), and minimal
detectable change (MDC) of pelvic rotation
The test-retest reliability, standard error of measurement (SEM), and minimal detectable change (MDC) of pelvic rotation
The means and standard deviations (SDs) of pelvic rotation measured by the
smartphone and palpation meter in the sitting, standing, and one-leg standing positions are
shown in Table 1. The test-retest reliabilities
(ICCs) of smartphone-measured pelvic rotation were 0.95 (
Linear regression analysis between smartphone and palpation meter data in sitting
position.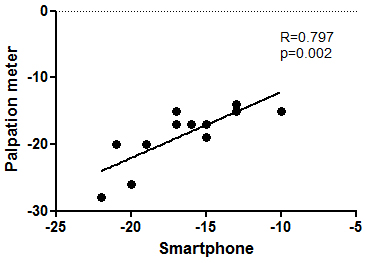
Linear regression analysis between smartphone and palpation meter data in standing
position.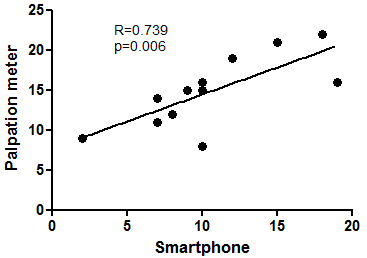
Linear regression analysis between smartphone and palpation meter data in one-leg
standing position.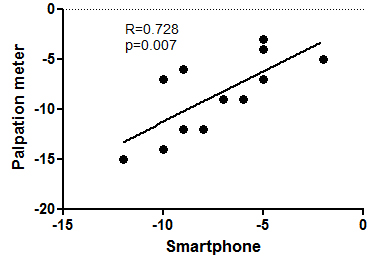
Pelvic rotation measured using the smartphone was
Test-retest reliabilities were excellent in the sitting, standing, and one-leg
standing positions (ICCs
The MDC is affected by measurement reliability and responsiveness [15, 16]; the
MDC is the minimal change that can be detected by the measuring instrument beyond
measurement error [17, 18]. The analyses show that the MDC was 2.01, 2.11, and 2.99 in the
sitting, standing, and one-leg standing positions; therefore, when the change in pelvic
rotation between two measurements reach these parameters, the clinicians might interpret the
changes as reliable beyond measurement error. A strong linear relationship was evident
between pelvic rotation measured using both a palpation meter and the smartphone. Generally,
it is considered that a correlation coefficient
Our study had certain limitations. First, we calculated only short-term MDC. Future studies should calculate minimal clinically important differences over the long term. Second, because the main purpose of this study is to compare pelvic rotation data obtained using a smartphone and those measured by a palpation meter, we could only measure test-retest reliability. Future studies will need to estimate inter-rater reliability for smartphone-based pelvic rotation in consideration of the risk rater errors. Finally, we measured pelvic rotation only in children with CP. Future studies should include typically developing children.
Conclusion
We confirmed that measurement of pelvic rotation using a smartphone is reliable in children with CP in the sitting, standing, and one-leg standing positions. Additionally, pelvic rotation values measured using the smartphone correlated significantly with those assessed using a palpation meter. Thus, the smartphone afforded excellent criterion-related validity. Measurement of pelvic rotation using a smartphone is easy, fast, and cost-effective in clinical settings [19]. Our findings contribute preliminary evidence of pelvic rotation evaluations using a smartphone in rehabilitation protocols for children with CP.
Footnotes
Acknowledgments
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (No. 2019R1G1A1100698).
Conflict of interest
The author has no conflict of interest to report.