
Abstract
PURPOSE:
Spina Bifida (SB) is a congenital defect of the neural tube resulting in motor and sensory defects and frequently includes insensate skin on the buttocks and feet which are innervated by sacral nerves. For those living in hot climates such as the Southwestern United States, environmental surfaces reach temperatures throughout June-September that cause thermal burns. The objective of this novel case series was to evaluate the circumstances associated with environmental buttocks burns in children with SB who attend the District Medical Group Children’s Rehabilitative Services Myelomeningocele (MM) Planning clinic in Phoenix, AZ.
METHODS:
Nine children and adolescents with SB and a history of environmental buttocks burns were identified through participation in the National Spina Bifida Patient Registry at District Medical Group Children’s Rehabilitative Services Myelomeningocele Planning Clinic. Parents and patients were interviewed about the burn circumstances, charts were reviewed, and information was gathered from the NSBPR including level of function and ambulation status.
RESULTS:
Most of the patients were found to be of emerging independent ages (average age 10 years) and were not with their parents at the time of the burn. All had myelomeningocele (MM), almost all were community ambulators, and all had mid lumbar, low lumbar or sacral level function. There were no non-ambulators. In addition, the majority were wearing incontinence products.
CONCLUSIONS:
Children and adolescents with MM who are community ambulators, of an emerging independent age, and live in hot climates are at risk of environmental buttocks burns. Enhanced education in environmental thermal burn prevention is important. This education should be particularly focused on the child as they spend more time in settings without their parents. In addition, this enhanced education should extend to those who support the child or teen such as teachers, coaches, family and friends.
Keywords
Introduction
In the Southwestern United States and particularly in Maricopa County, Arizona, the average high temperatures are above 38
Although it makes sense that insensate skin can increase risk of burns, a literature search revealed relatively few supporting citations. Previous literature that is available suggests that thermal burns including scald, flame, contact with hot surface, and flash burns [4] are the most common types of burns in children. In addition, burns in teenagers with spinal cord injury (SCI) tend to be cooking related while those with SB tend to be scald injuries [5]. Another study of children with SB and other neurological impairments found that a majority with burns were secondary to scalding injuries while bathing [6]. In addition, it has been noted that burns in children and teenagers with SCI and SB, even on smaller surface areas, were more likely to need surgery [5]. Of all wounds in individuals with SB, wheelchair ambulators developed a disproportionate share of the wounds, and 60% of patients with chronic wounds were primarily wheelchair ambulators; however, these were mostly pressure sores and not burn related [11].
In this novel case series, the authors describe the circumstances associated with environmental buttocks burns in 9 children and adolescents who attend the Myelomeningocele Planning Clinic at District Medical Group Children’s Rehabilitative Services, a multispecialty interdisciplinary clinic, in Phoenix, AZ, and are consented participants in the CDC National Spina Bifida Patient Registry (NSBPR). The clinic cares for children, adolescents and young adults with the full spectrum of SB diagnoses as well as other neural tube defects. The authors hypothesize that presence of a parent well educated about SB would decrease likelihood of burn, and presence of incontinence product may decrease likelihood or severity of burn.
Credit: Mediscan/alamy stock photo, used with permission.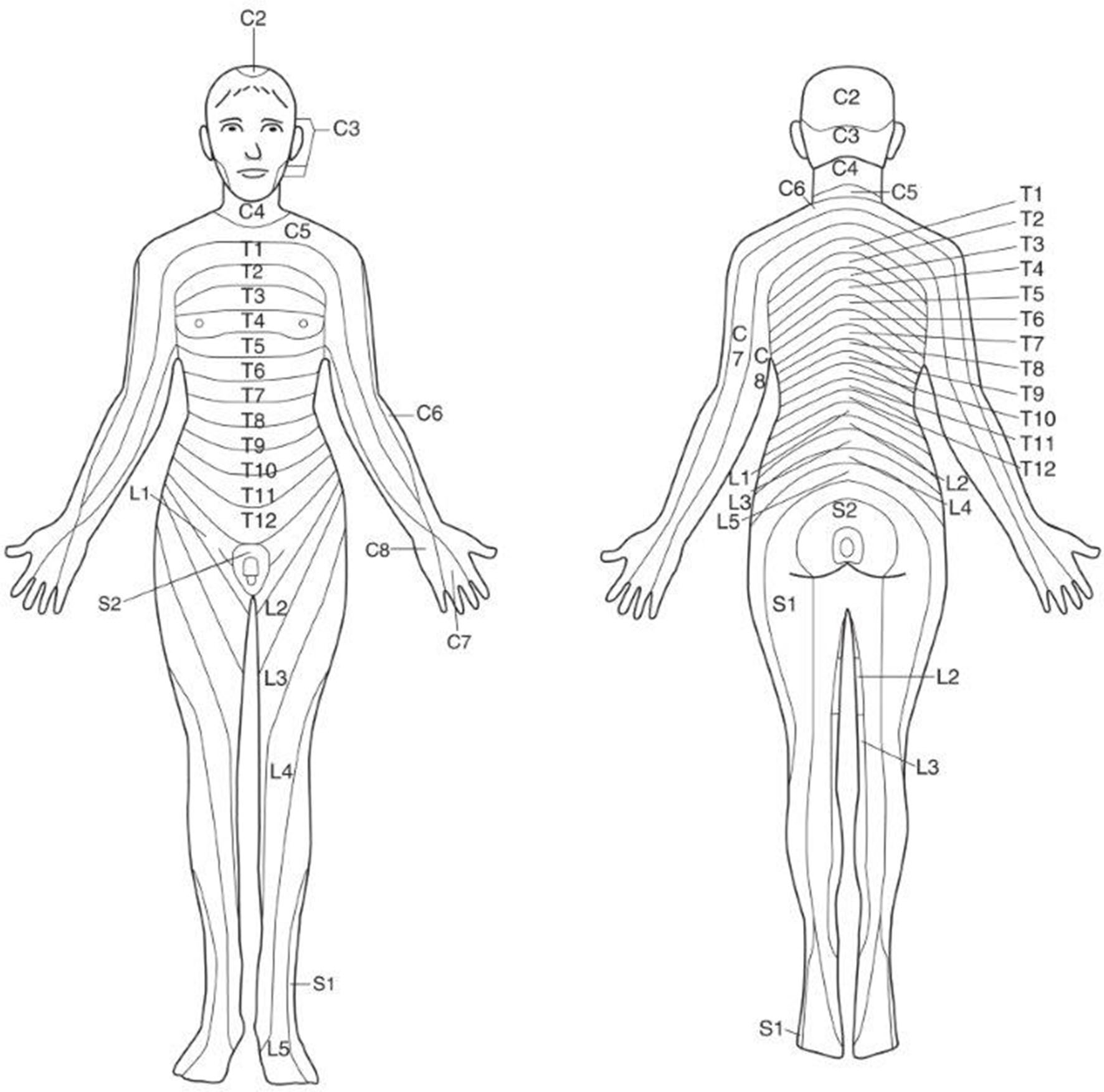
Patients with environmental buttocks burns were identified in this Medicaid only clinic (newborn to 25 y) through enrollment in the CDC National Spina Bifida Patient Registry (NSBPR) and identification of a burn in the posterior pelvis (coccyx, sacrum, ischium) in the previous year or historically. The study was approved by IntegReview Institutional Review Board. The registry annual form includes a question on presence of skin breakdown, the location and the primary cause. The clinic initially enrolled in the NSBPR in 2017, and at the time of data collection for this series the clinic patient enrollment in the NSBPR was 174. The authors elected to identify this area as the buttocks for general ease of description and relationship to sitting. A research coordinator contacted the parent/guardian by phone or in person at the clinic and asked: 1) what year the burn occurred, 2) what age the patient was at time of burn, 3) what month of year burn occurred, 4) was patient wearing an incontinence pad at time of burn, 5) what clothing patient was wearing at time of burn, 6) what surface caused the burn, 7) was a parent present at time of burn, 8) what was the size and severity of the burn if known, 9) was patient hospitalized for the burn, 10) what treatment was provided including surgery. Medical records were reviewed if available. Type of SB, level of function, presence of ventriculoperitoneal shunt (VP), and ambulatory status were derived from the annual questionnaire of the NSBPR. Functional level is determined by strength testing and categorized as thoracic (flaccid lower extremities), high lumbar (hip flexion present), mid lumbar (knee extension present), low lumbar (foot dorsiflexion present) and sacral (foot plantar flexion present). Ambulation status is described as non-ambulator (uses wheelchair exclusively for ambulation), therapeutic ambulator (walks only for a therapy session), household ambulator (walks only indoors and with assistive device and requires little or no assistance in transferring) or community ambulator (walks indoors and outdoors for most activities).
Results
Eight of the patients were 8–16 years old with an overall average age of 10. All nine had myelomeningocele, and five had VP shunts. The burns occurred one to two years prior to interview or medical record review in 6 of the 9 patients and four to six years prior in the remaining three. All occurred in June, July or August. Seven of the nine were female. Six of the nine had mid lumbar level function, two low lumbar level function and one sacral level function as defined by the NSBPR. All but two were community ambulators, and the other two were household and therapeutic ambulators. None were nonambulators. Seven of the nine were known to be wearing an incontinence pad. The clothing worn when the burn occurred varied among the patients in the series. The surface sat on varied including side walk, trampoline, river rock, cement, sand, metal bench and planter cement wall. A parent was present for only two of the buttocks burn injuries, and the 3 year old in the series was being supervised by a nonparental adult. Two of the nine required hospitalization and surgery, and three required wound clinic care. The other four healed with non-wound clinic outpatient treatment. More specific information about treatment was not collected, but all had second or third degree burns that resulted in scarring. None of the patients in this series had recurrent burns.
Discussion
This novel series highlights a regional risk for children/teens with SB who are ambulatory with insensate buttocks skin during June, July, August and September; and to our knowledge, no such study exists on relative risk of environmental burns in SB patients between different geographical areas. The burn risk appears to be higher without guidance by a parent/guardian who is well educated about SB to remind/warn the child/teen of the risk. The age range of 8–16 years is typically when children are becoming more independent and perform activities alone or with other supervising adults who may not know the issues and risks related to SB. Transition to more independent care is a gradual process occurring throughout the lifespan and is especially important in the teen years as adolescents take more responsibility for their own health care [12].
Myelomeningocele is more commonly associated with hydrocephalus and need for VP shunt than other forms of SB. Although the majority of children with myelomeningocele have IQs within the normal range, many have executive function disorder hypothesized to be associated with the presence of hydrocephalus and/or VP shunt [7]. In this series we did not include cognitive ability of each patient in our analysis. In other research, it has been shown that for children with SB and other handicapping conditions, 80% of all burn injuries could be prevented with supervision and protection [9].
Summary of spina bifida patient characteristics with environmental buttocks burns. Information retrieved from the NSBPR or from interview/medical record
Summary of spina bifida patient characteristics with environmental buttocks burns. Information retrieved from the NSBPR or from interview/medical record
*Myelomeningocele.
Of particular note is that none of the children were non-ambulators and only one was a therapeutic ambulator who was specifically working toward household and community ambulation at the time of the burn. This therapeutic ambulator is likely an outlier in the series. Furthermore, none had high lumbar or thoracic level function status. This suggests that those walking as community or household ambulators are more at risk for an environmental buttocks burn than the nonambulators (primary wheelchair ambulators) who are less likely to transfer out of their chair to an outdoor surface. We did not specify which patients used assistive devices such as forearm crutches or walkers at the time of their burn in this series.
Interestingly, the environmental surfaces sat on and the extent and treatment of the burns varied. Some sat low to the ground while others sat on a bench or leaned against a surface causing the burn. Two required inpatient care and surgery.
With the exception of one patient, all wore some type of incontinence product (other than a simple pad) presumably providing some protection and possibly mitigating the severity of the burn. However, pull-ups and diapers or briefs do not provide any protection to the posterior upper thigh area or ischium innervated by sacral nerves.
Skin innervation of the buttocks area and posterior upper thighs are entirely by sacral nerves which are the most likely to be nonfunctioning in patients with SB or other distal spine abnormalities. (diagram) The “Did You Look?” campaign, developed by the National Spina Bifida Association (
The study has a number of potential limitations. It is understood that the dependence on parental recall about burn details in some of the cases raises concern about accuracy, however, most of the series patients had burns in the previous two years and six of the nine had severe enough burns to require hospitalization and surgery or wound clinic care likely improving recall. We cannot exclude the possibility that there are other regional patients whose burns may have been minor and not reported. In addition, given the ages of the children at time of burn and subsequent time of enrollment in our study, the authors do not expect the ambulatory status to be substantially different than at the time of the burn.
Children and adolescents with MM who are community ambulators, of an emerging independent age, and live in hot climates are at risk of environmental buttocks burns. Incontinence products may mitigate the severity of the burn but will not prevent a burn. The authors conclude that enhanced education in the Southwestern United States, and other similar climates, to prevent environmental buttocks burns is critical and needs to be focused on the patient (in addition to the parents and caregivers) as he/she reaches the ages of increased independence. Because of the executive dysfunction so common in individuals with myelomeningocele, it is also important to reach out to those who support the children and teens for enhanced preventative education including teachers, coaches, family and friends. Although this education is important for all the clinic patients, the risk should be stressed for those who are household or community ambulators. In addition, it can be surmised that incontinence products may mitigate the severity of burns, but this cannot be conclusively determined. For lifestyle and social reasons, the authors would not routinely recommend use of pull-ups or briefs simply for burn protection.
Footnotes
Acknowledgments
The authors thank Mary Dexter, RN, BSN, and Deborah Anderson, RN, BSN, CPNP as participating investigators. The authors thank District Medical Group for its support in research and data collection. The Institutional Review Board supporting this research is with IntegReview. The authors thank Susan Shelly, BSN, MLS, Library Services at HonorHealth John C. Lincoln Medical Center for support in literature search. The authors thank the many individuals with SB and their family members who participated in this research, without whom the NSBPR would not be possible. The NSBPR has also been successful because of the contributions of the Centers for Disease Control and Prevention, the Spina Bifida Association, and all members of the NSBPR Coordinating Committee. Members of this Committee during the collection of the data reported are listed in alphabetical order and were Richard Adams, Texas Scottish Rite Hospital for Children, Dallas; Pat Beierwaltes, Children’s Hospital of Michigan, Detroit; Timothy Brei, Riley Hospital for Children, Indianapolis; Robin Bowman, Ann and Robert H. Lurie Children’s Hospital of Chicago, Chicago; Heidi Castillo, Cincinnati Children’s Hospital Medical Center, Cincinnati and Texas Children’s Hospital, Houston; James Chinarian, Children’s Hospital of Michigan, Detroit; Mark Dias, Hershey Medical Center, Hershey; Brad Dicianno, University of Pittsburgh Medical Center, Pittsburgh; Nienke Dosa, Upstate Golisano Children’s Hospital, Syracuse; Carlos Estrada, Boston Children’s Hospital, Boston; Kurt Freeman, Oregon Health and Science University, Portland; Greg Heuer, Children’s Hospital of Philadelphia, Philadelphia; David Joseph, Children’s Hospital of Alabama, Birmingham; Sarah Korth, Kennedy Krieger Institute, Baltimore; Pamela Murphy, District Medical Group Children’s Rehabilitative Services, Phoenix; Jacob Neufeld, Children’s Hospital and Research Center at Oakland, Oakland, University of California at San Francisco Benioff Children’s Hospital, San Francisco, and St. Luke’s Boise Medical Center, Boise; Joseph O’Neil, Riley Hospital for Children, Indianapolis; Michael Partington, Gillette Children’s Specialty Healthcare, St. Paul; Paula Peterson, Primary Children’s Medical Center, Salt Lake City; Elaine Pico, Children’s Hospital and Research Center at Oakland, Oakland and University of California at San Francisco Benioff Children’s Hospital, San Francisco; Karen Ratliff-Schaub, Nationwide Children’s Hospital, Columbus; Kathleen Sawin, Children’s Hospital of Wisconsin, Milwaukee; Kathryn Smith, Children’s Hospital Los Angeles, Los Angeles; Katherine Steingass, Nationwide Children’s Hospital, Columbus; Stacy Tanaka, Monroe Carell Jr. Children’s Hospital at Vanderbilt, Vanderbilt; Jeffrey Thomson, Connecticut Children’s Medical Center, Hartford and Shriners Hospitals for Children Springfield, Springfield; David Vandersteen, Gillette Specialty Clinics, St. Paul; William Walker, Seattle Children’s Hospi- tal, Seattle; John Wiener, Duke University Medical Center, Durham; Pamela Wilson, Children’s Hospital Colorado, Denver; and Hadley Wood, Cleveland Clinic, Cleveland; Jason Woodward, Cincinnati Children’s Hospital Medical Center, Cincinnati
Conflict of interest
The authors have no conflict of interest to report.