
Abstract
Conventional knee-ankle-foot orthoses (KAFOs) are generally prescribed for children with lower limb muscle weakness and joint instabilities. The main function of KAFOs is to provide stability during gait by locking the knee in full extension. However, walking with the knee joint in a fully extended position requires excessive energy consumption, leading to early fatigue and inducing non-physiological gait patterns. A new generation of KAFOs was developed to allow free knee flexion during the swing phase and to lock the knee joint during the stance phase to provide the required stability. These are commonly labeled as stance-control knee-ankle-foot orthoses (SCKAFOs). Nevertheless, commercial SCKAFOs are not available for the pediatric population. Especially in early ages, children must frequently replace the orthosis due to their growth. Hence, the proposed design presents a solution for a SCKAFO with adjustable length adaptable to children’s dimensions ranging from two to six years old.
Introduction
Human gait is a complex process in which different body parts move in a coordinated way. Lower limbs are able to support the body weight during the stance phase of the human gait cycle, to rotate and coordinate joint movements, to allow forward progression of the body, to adjust limb length by flexing the knee during the swing phase, and to promote a smooth motion of the center of gravity in order to save energy [1]. Children generally develop physiological gait patterns at the age of three. Until this time, the child moves with the upper limbs distanced from the body in order to keep the body balanced [2]. Normal walking requires muscular strength, joint mobility, and movement coordination controlled by the central nervous system. Deficiency of any of these abilities can impair the stable gait [3].
Individuals with a significant weakness of the knee extensor musculature or articular deformity due to pathologies such as poliomyelitis, multiple sclerosis, incomplete spinal cord injury, or congenital defects usually require a KAFO [4]. Conventional KAFOs are lower limb devices composed of rigid bars that extend over the lower limb, enabling locking of the knee joint in full extension for walking, providing stability during both swing and stance phases and preventing the leg from collapsing during weight bearing. However, this available design for children does not allow any knee flexion during the swing phase. Children using a locked knee KAFO present a functionally long limb and clear the foot during swing phase by adopting compensatory movements such as ipsilateral circumduction, hip hiking, or contralateral vaulting [5, 1]. These can cause soft tissue and joint injuries of the hip and lower back [6]. Furthermore, some studies point out that walking with the knee locked in full extension causes a reduction of gait efficiency (24%) [7] and increased vertical displacement of the center of the mass (65%) [8]. In order to avoid these problems, a KAFO should provide complete restriction of knee flexion during the stance phase to promote the required stability, and unrestricted knee flexion during the swing phase to promote foot clearance. A KAFO containing the aforementioned characteristics is labeled as a SCKAFO.
Different concepts of SCKAFOs were developed over the last forty years [4], applying mechanical, electromechanical, or hydraulic systems to automatically lock/unlock the knee joint according to the gait phase. Mechanical SCKAFOs are usually engaged using the ankle motion or limb inclination [4]. An example is the UTX
QFD used to design the orthosis. The importance weights of the stakeholder requirements were defined based on the data of a questionnaire answered by health professionals that are directly in contact with orthoses users. The target requirements are highly important to define the orthosis requirements.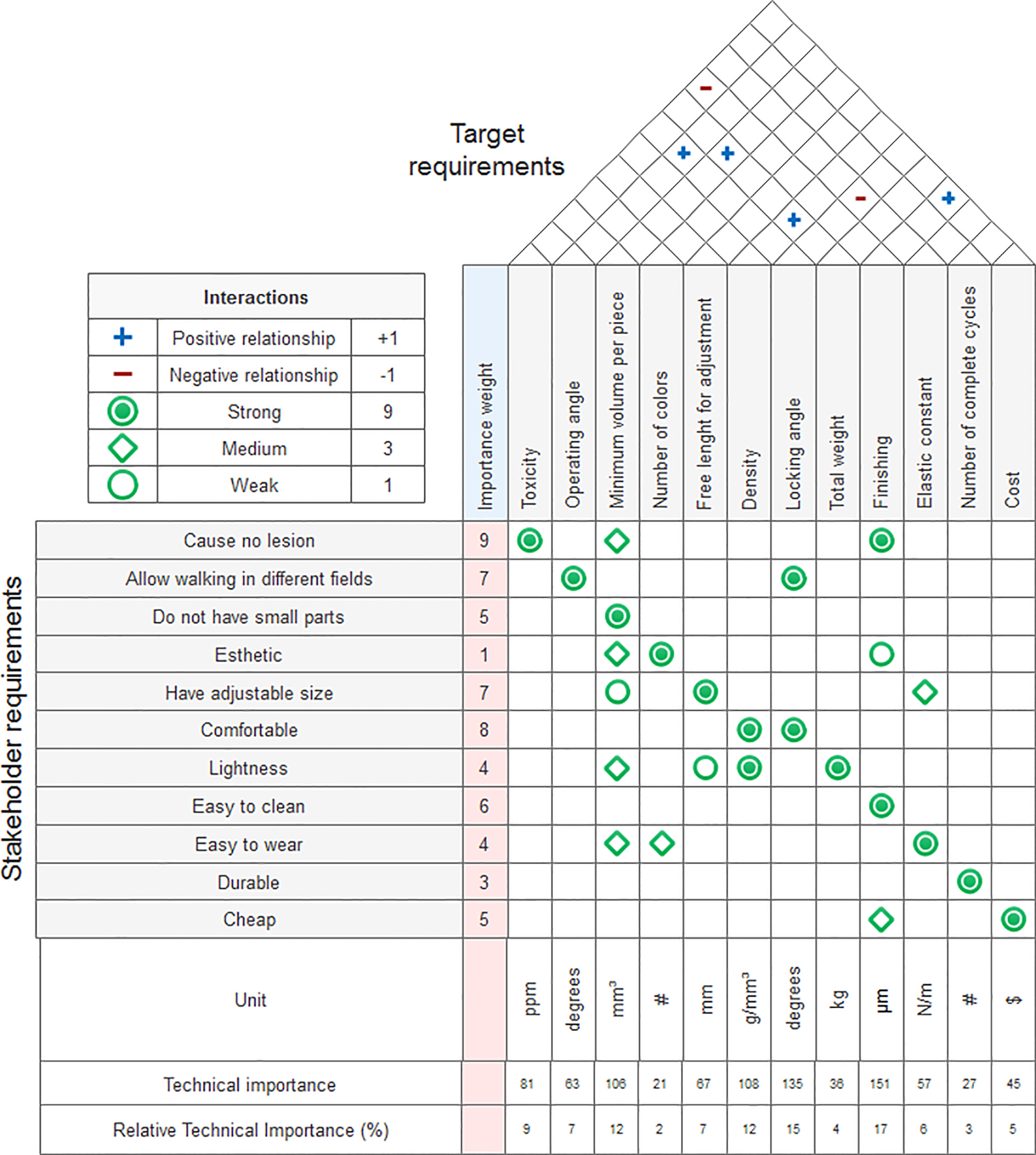
When children have some type of lower limb deficiency it is important to use prostheses or orthoses as soon as possible, as they facilitate the correction of required compensations for the swing phase of the non-articulated limb [9]. The earlier the transition to an articulated device, the easier will be to develop a physiological gait pattern that is more efficient, energetic, and safe [10]. Furthermore, the use of an articulated knee allows for the child’s maximal participation in activities associated with their psychomotor development and social interaction [11]. The design of orthotics for children is still an engineering challenge because most of the available SCKAFO solutions are not adapted to the pediatric population, although this is an important stage in motor skill acquisition. While conventional KAFOs are commercially available, they must be replaced as the child grows and uses different devices during the gait learning period. As such, the child’s development may be impaired by the adaptation period and sometimes by the unavailability of orthoses in nearby medical centers. Thus, the design of a SCKAFO for children adaptable to a relatively large range of ages is required.
In order to design the orthosis, the device requirements should be detailed. To accomplish this step, it was necessary to understand the problem, analyze the current market solutions, and discuss the possible solutions with health professionals. To define the dimensions of the device, the anthropometric data of lower limbs of children from two to six years old was analyzed. The patient’s weight was also essential information for dimensioning the orthosis’ mechanical elements. At the age of 6 years old, the average weight of children is 20 kg [12].
As previously discussed, some SCKAFO solutions make it difficult to walk on uneven or inclined surfaces, to transpose an obstacle, or to climb stairs. In addition, the SCKAFO must be robust, safe, and impact resistant, since children are usually less careful. At the same time, SCKAFOs for the pediatric population must be light to avoid muscular fatigue during gait [13, 14].
Aesthetics are also extremely relevant to this application. An orthosis with a good surface finishing, attractive appearance, and low volume is essential because children should feel attracted to wearing it without concerns [6]. Other relevant points are the comfort of the orthosis, connection to the patient, and the ease of adjustment or removal of the orthosis daily.
The relevant requirements to develop the orthosis were made through an analysis of the solutions available in the market, of the scientific research in the area, and by a questionnaire designed for health professionals who are in daily contact with users of lower limb orthoses. In this questionnaire, they were asked to order the main needs of a child’s orthosis for lower limbs. The information from twelve subjects was translated into engineering requirements through a design methodology for planning and quality control called Quality Function Deployment (QFD). QFD is useful for systematically customer-oriented product development and process planning. Customer needs were precisely adapted into product characteristics and design requirements [15]. Figure 1 presents the QFD with weights (obtained from the questionnaire) demonstrating the conversion of user requirements into technical characteristics, with the dependence relationship between them.
Analyzing the values of technical importance collected from the QFD, it is possible to verify relevant information needed to design the orthosis. The highest percentage values obtained among the technical characteristics were the ability to resist knee flexion at any operating angle in the stance phase and to allow free motion in the swing phase. Furthermore, designing the surface finishing was also an important feature in order to guarantee the hygiene and safety of the user. In addition, the designed device should have lightweight parts in order to maintain the user’s comfort.
After establishing the user’s needs and obtaining the technical characteristics from the QFD, it was possible to seek solutions for the global problem (already separated into objective problems) by looking for appropriate operating principles that meet the associated functions and requirements.
Results
Virtual model
After obtaining the main design requirements for the orthosis, a virtual 3D model was created. Figure 2 illustrates the orthosis attached to the patient by four straps. Figure 3 shows the designed device with a length adjustment mechanism for the child’s growth from two to six years old. The designed device is made out of a metal structure that promotes support to the body during the gait. Such structure contains the following mechanisms: ankle joint with a pivoting cable to unlock the knee joint, knee joint with a mechanical ratchet that allows free extension but may limit flexion according to ankle dorsiflexion, and both superior and inferior support bars with length adjustment and attachment to the patient.
Illustration of the orthosis’ connection to the patient’s leg. Four straps are used to keep the orthosis connected to the leg.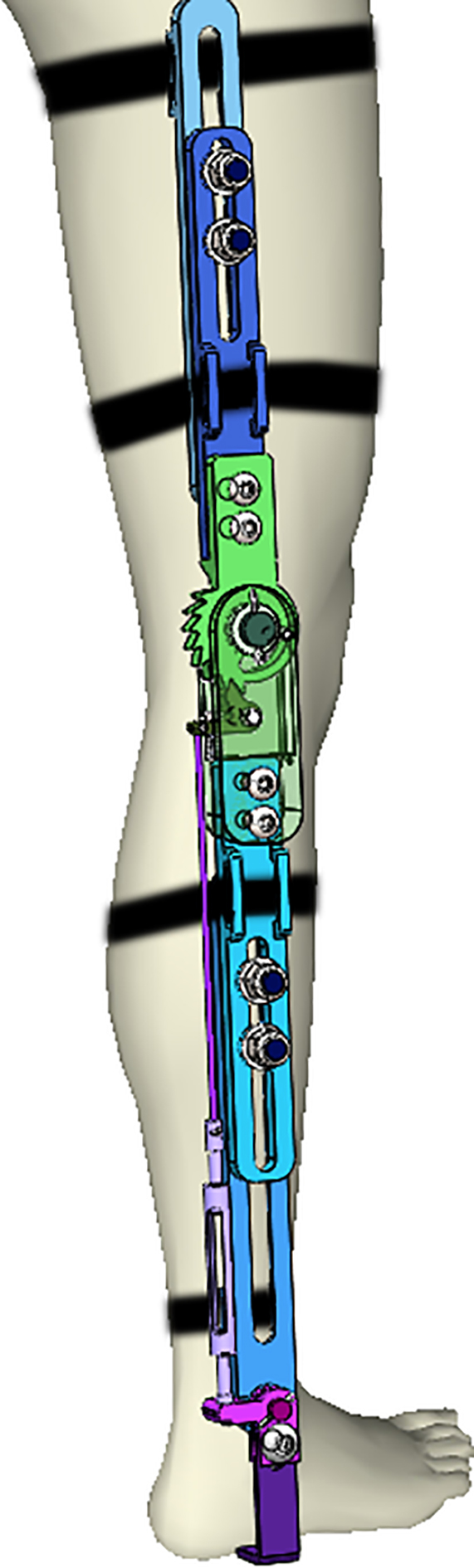
Designed orthosis and views of the articulation mechanism (a), the articulation lock mechanism (b), and the length adjustment mechanism (c).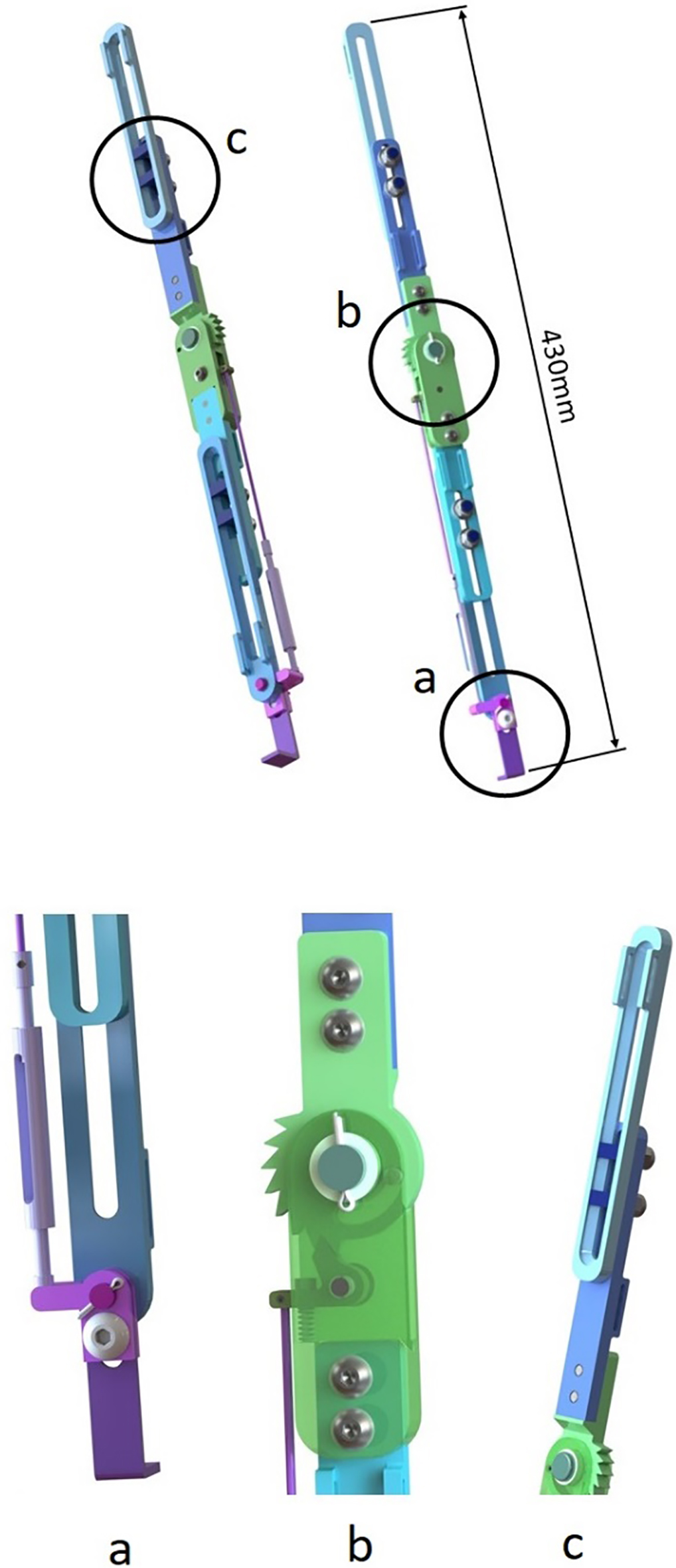
Figure 3c shows the length adjustment mechanism of the designed support bar that allows for increasing the bar’s length during the child’s growth. The screws are made out of stainless steel and their wedge shape ensures that the screws fit into the cavities in the aluminum support bars, making it easy to adjust the length without any specific tools while the orthosis is attached to the user.
Figure 3a shows the lever attached to the ankle joint that allows adjusting the tension of the cable that unlocks the knee joint when the ankle dorsiflexes. This mechanism consists of a cable, a turnbuckle, the ankle joint, and the lever attached to a curved part that supports an insole connected to the user’s feet. During gait, when the user dorsiflexes the ankle, the lever rotates, pulling the cable connected to the knee joint and unlocking the articulation. The turnbuckle consists of a stainless steel body and two threaded tops. On one end, a screw thread moves in the clockwise direction and on the other end it moves in the opposite direction. The turnbuckle allows for the cable’s length adjustment while the child is growing.
The locking mechanism in the knee joint (see Fig. 3b) consists essentially of three different parts:
a ratchet attached to the superior support bar that rotates on the knee joint axis; a small lever connected to an articulating pin attached to the inferior support bar that is pulled by the cable in one end, with a tooth in the other end that unlocks the ratchet; a spring that pushes the lever to lock the ratchet rotation forcing the tooth to engage with the ratchet. The ratchet enables the free extension of the knee joint but locks the flexion in different angles (when any of its teeth are locked by the ankle joint in the extended position), allowing the user to access ramps and irregular surfaces.
After creating the virtual model of the orthosis, some design calculation to verify the mechanical strength of the device is required to ensure that patient safety is not compromised. For example, according to [11], the knee joint must withstand a flexion moment of up to 1.71 Nm/kg of body mass during stair climbing. In the case of a six year old child, this flexion moment is 34.2 N.m. This value was used to design the support bar width and to perform a Finite Element Simulation of the ratchet using CAE software. Other component dimensions were also analyzed considering the worst loading case scenario, using conventional analytical models commonly used in mechanical design such as the example presented below. Namely, we analyzed the contact pressure and the number of bolts (and the corresponding necessary torque) to avoid the relative motion between the support bars (in the length adjustable system), the shear stress and contact pressure in all the articulating pins, the tensile load in the cable, the spring elastic constant, and the cross-section area of the parts. During calculation, it was ensured that each of the components had a safety factor higher than two. The components that presented a low factor of safety were resized and/or stronger materials were selected so that the safety of the user was guaranteed.
Force distribution in the frontal view in one leg during monopedalic support. a) shows the applicable forces at a noninjured knee while b) shows the reaction forces when the user is wearing the proposed SCKAFO. 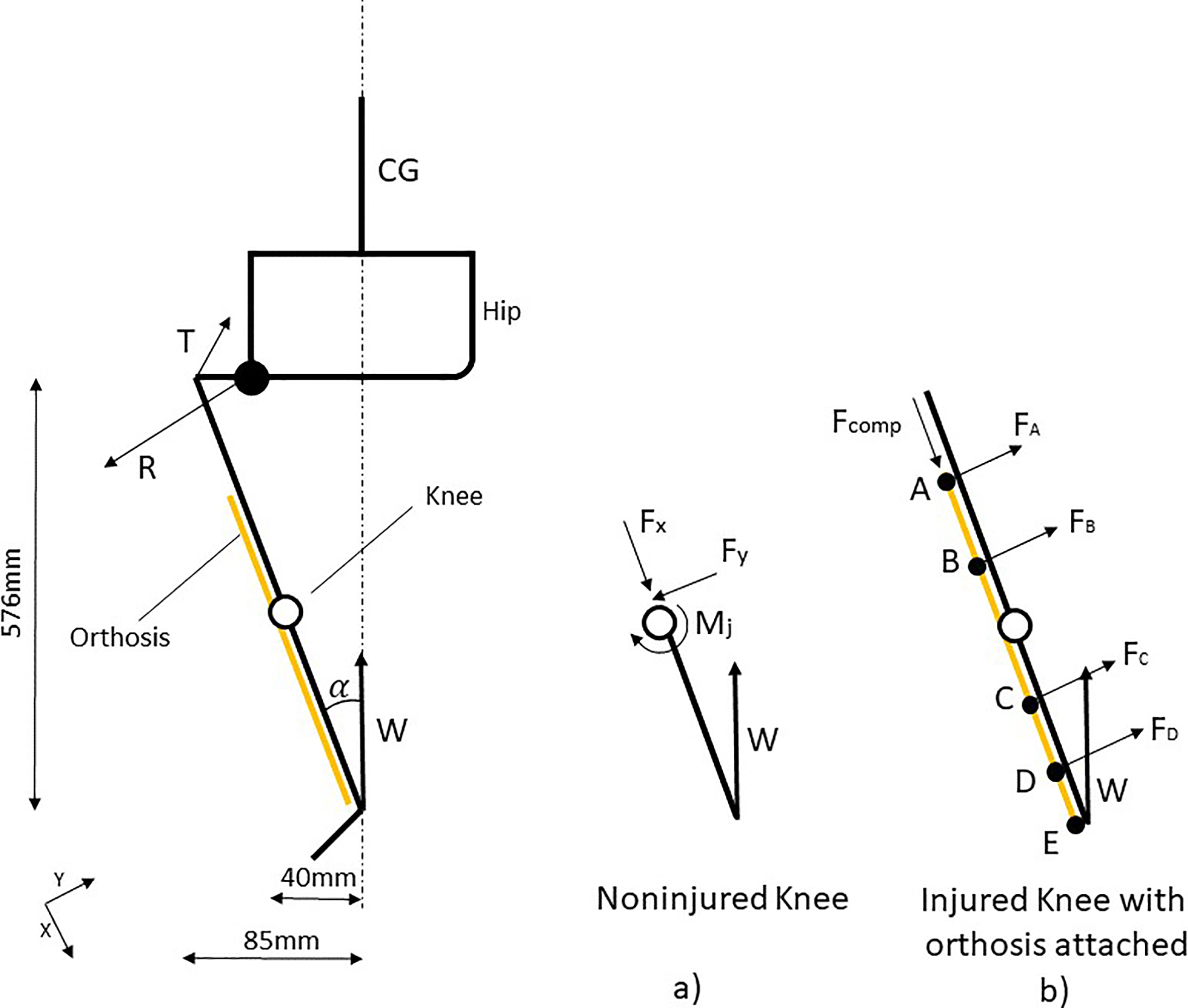
The following example describes the process to design the support “bars” thickness. Figure 4 shows the distribution of forces at a specific moment of the gait cycle (in the frontal plane with monopedalic support) in which the load is concentrated in the orthosis. Force
Equation (1) calculates the compression force described in Fig. 4b which is useful for dimensioning the device parts. A child at the age of six years old weighs about 20 kg.
The reaction forces on the four straps are caused by the component of the force
Thus, the orthosis has a constant compression force equivalent to the user’s weight. The bending moment diagram along the orthosis and perpendicular to the frontal plane is presented in Fig. 5a. The shear diagram along the orthosis is presented in Fig. 5b. Based on these applied forces and reactions, it was possible to perform the component stress analysis to verify the support bar thickness, pin diameter, and other parts’ dimensions.
a) Bending moment perpendicular to the frontal plane. The figure shows that the maximum bending moment occurs at the point where the first strap is connected, point D. b) Shear force in the frontal plane. The figure shows that the maximum shear force occurs between points D and E.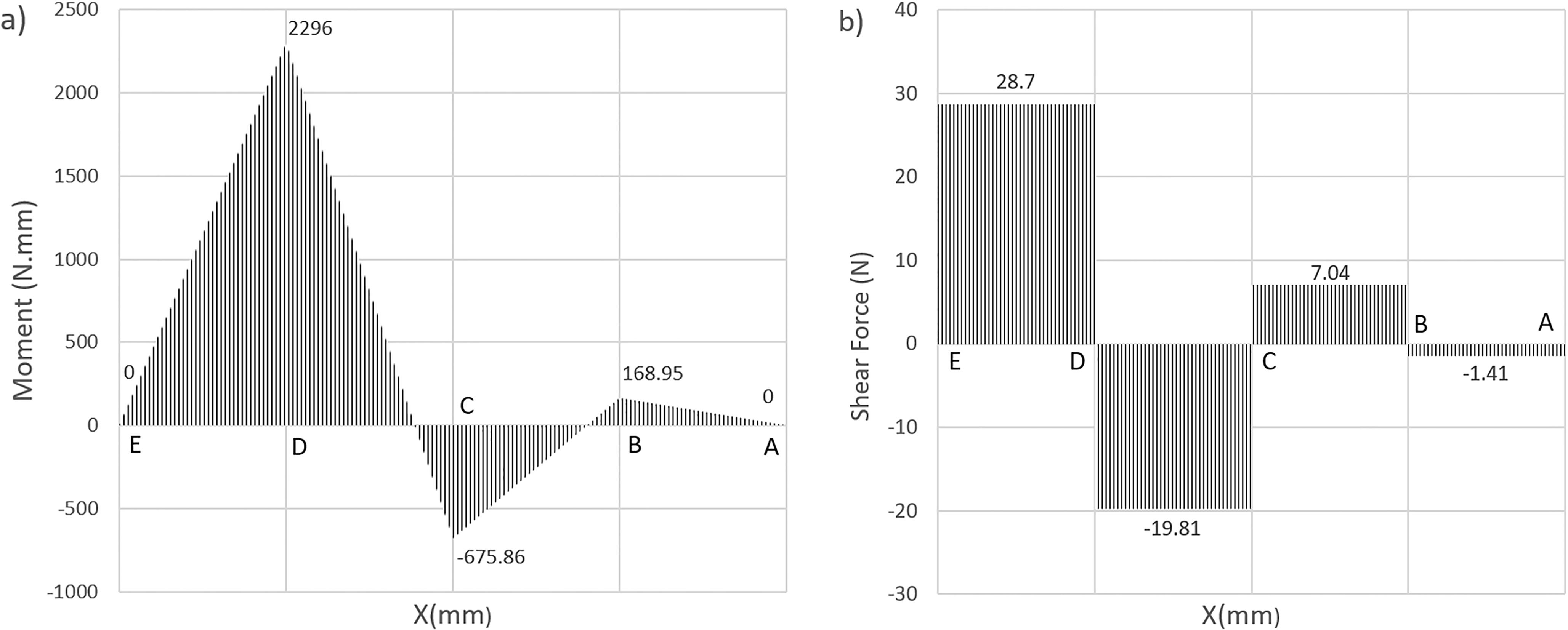
Manufactured SCKAFO after assembling all components. The prototype is functional and is ready to be tested on children between two and six years old. The whole device weighs less than 500 grams and costs less than 400 USD to be manufactured. 
Once all the design steps were completed, it was possible to manufacture a prototype to verify the operation of the mechanisms that compose the orthosis. After machining the metal parts, the orthosis was then assembled, as can be seen in Fig. 6. Then, the operation of the main mechanisms, the ankle joint activation system, the knee joint locking system, and length adjustment, was verified.
An important requirement observed in the questionnaires was the need to allow the user to adjust the orthosis length according to their growth. The proposed solution allows a simple and easy adjustment while the user is wearing the orthosis. It is also important to point out that the proposed orthosis meets the need for length adjustment according to growth, promoting an innovative characteristic to consumers in relation to other market solutions with a low-cost device due to the simplicity of the solution.
Among the several highlighted needs that were applied to the designed orthosis, the locking mechanism of the orthosis joint was the most important as it was designed aiming to guarantee the safety of the user during the gait.
Although a heel-tilting mechanism to activate the knee joint is a well-known solution, the possibility of adjusting the cable length with a turnbuckle is a solution not yet applied to the orthotics market. This mechanism also allows adjustment of the cable length according to the child’s growth. However, this solution is restricted to patients with no tibiotarsal joint limitations.
Conclusions
This work presented an alternative solution for a SCKAFO design that is adjustable in length to help children with lower limb dysfunction. Comparing the designed prototype with requirements obtained through the questionnaires, most of the requirements of the users were met. The QFD assisted the project development by ordering design priorities and translating the features raised through the questionnaire into engineering definitions.
This project has not yet completely fulfilled its development cycle. In fact, this is the first iteration. Hence, in future work, this prototype will be tested in clinical trials to validate all the designed features. Then it will be possible to perform kinematic and kinetic studies to compare the energy efficiency with the commercially available designs for the pediatric population.
Footnotes
Conflict of interest
No authors have any conflicts of interest to disclose.