
Abstract
PURPOSE:
Aware of the higher birth prevalence of spina bifida (SB) among Hispanics/Latinos, we aimed to appraise the literature as it relates to cultural context through a review of quality of life (QOL) studies conducted among individuals with SB in order to improve care among immigrant families.
METHODS:
A systematic review was conducted consistent with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines. The inclusion criteria were: (1) children and adolescents (5–21 years of age) with SB and/or myelomeningocele; (2) quantitative studies; (3) health-related QOL outcome measured by validated instrument determinants; and (4) US-based studies. Articles meeting inclusion criteria were assessed using the focused conceptual framework informing the study (i.e., social determinants of health).
RESULTS:
Eighteen studies met inclusion criteria, with eight different QOL instruments represented. The majority of studies used generic assessments of QOL (72%), two reported the use of both a generic and a SB-specific QOL measure (11%), and three (17%) documented QOL utilizing a SB-specific validated instrument. Only seven (39%) of the studies stated that they included Hispanics/Latinos and only six (33%) reported including Spanish-speaking individuals.
CONCLUSIONS:
QOL in individuals with SB is mediated by a wide-range of interrelated factors. In order to better serve this vulnerable population as they transition across the lifespan, multilingual condition-specific QOL measures need to be further developed and implemented among Hispanic/Latino individuals with SB, especially those who are recent immigrants.
Keywords
Introduction
Neural tube defects (NTDs), frequently understood as anencephaly and spina bifida (SB), have a birth prevalence of nearly six per 10,000 live births in the United States (US) [1]. Cases arise from a combination of genetic and environmental factors that are poorly understood [2, 3]. Prevalence rates of SB are also considerably influenced by the mother’s race/ethnicity [4]; Hispanics/Latinos consistently have a higher birth prevalence of SB compared with the other racial/ethnic groups in the US [1]. The most common form of open SB is myelomeningocele (MMC), which has long been associated with numerous cognitive, mobility, urologic, and orthopedic comorbidities [5, 6]. Adding to this disease burden, a number of potentially preventable complications have been described such as skin injury, infections, renal stones, and renal failure [7].
In recent years, the life expectancy of affected individuals has increased [8], and the assessment of SB-related disease burden on their quality of life (QOL) has become progressively important in patient-centered care as they transition across the life course [9]. QOL has commonly been defined as “an individual’s perception of their position in life in the context of the culture and value systems in which they live, and in relation to their goals, expectations, and concerns” [10]. The ecological framework, which recognizes that many socioeconomic influences (e.g., social gradients, stress, and social exclusion) impact and often help explain some of the divergent health outcomes found among communities, has termed these factors social determinants of health (SDH) [11, 12]. This holistic approach, which elucidates multiple variables (e.g., stress and demographic variables) as contributors to the overall QOL, is not foreign to the study of QOL among individuals with SB [13].
At the same time, the US Department of Health and Human Services’ Healthy People 2020 initiative underscored the importance of addressing the SDH by advocating for the creation of “social and physical environments that promote good health for all.” Under this charter, social and physical determinants include: language, culture, access to health care services and schools, as well as limited exposure to deleterious social norms, physical barriers, and hazards [14]. Thus, the SDH framework encompasses four categories of interrelating factors: 1) socioeconomic circumstances, 2) psychosocial factors, 3) political, economic, and cultural drivers, and 4) neighborhood environment [15, 16]. The Centers for Disease Control and Prevention (CDC) points to SDH as the “conditions in the environments in which people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and QOL outcomes and risks” [14]. The CDC has stated that when attempting to mitigate racial/ethnic health disparities, it should be remembered that SDH effectively contribute to longevity and QOL [17]. Moreover, the CDC goes on to state that healthcare delivery can be hindered if providers are not cognizant of the cultural context (e.g., language and culture); linguistic obstacles form a specific challenge of effectively working across cultures. Therefore, it is imperative that healthcare providers deliver support to those with language barriers to ensure care is received by all members of a community [17].
Increasingly, investigational interventions are actively pursued in an effort to treat the issues associated with SB [18, 19]. As innovative procedures are subsequently applied, their impact on QOL should be studied utilizing validated instruments. In the US, in an effort to ensure that women and minorities are included in representative numbers in studies supported by the National Institutes of Health (NIH), Congress passed the NIH Revitalization Act of 1993 [20]. The directive of this act – and the ensuing redefining of sampling regulations – safeguards adequate representation of ethnic and racial minorities in research studies [21]. Concurrently, since the year 2000 there has been a 49% increase in global immigration amongst low and high-income nations [22]. In the US, 25% of children live in immigrant families [23], and of the estimated 55 million Hispanics/Latinos, nearly three of every four speaks Spanish at home while remaining the fastest-growing demographic group [24, 25]. In this setting, previous systematic reviews of health-related QOL (HRQOL) assessments have called for the exploration of social environments and HRQOL [26]. We sought to examine if appropriately validated instruments, which take into account cultural context, are available and the extent of their use to assess QOL in this historically underserved US population. Therefore, the purpose of our study was to appraise the literature as it relates to language through a review of QOL studies conducted among individuals with SB in order to improve care among immigrant families.
PRISMA flow diagram [27]. For more information, visit 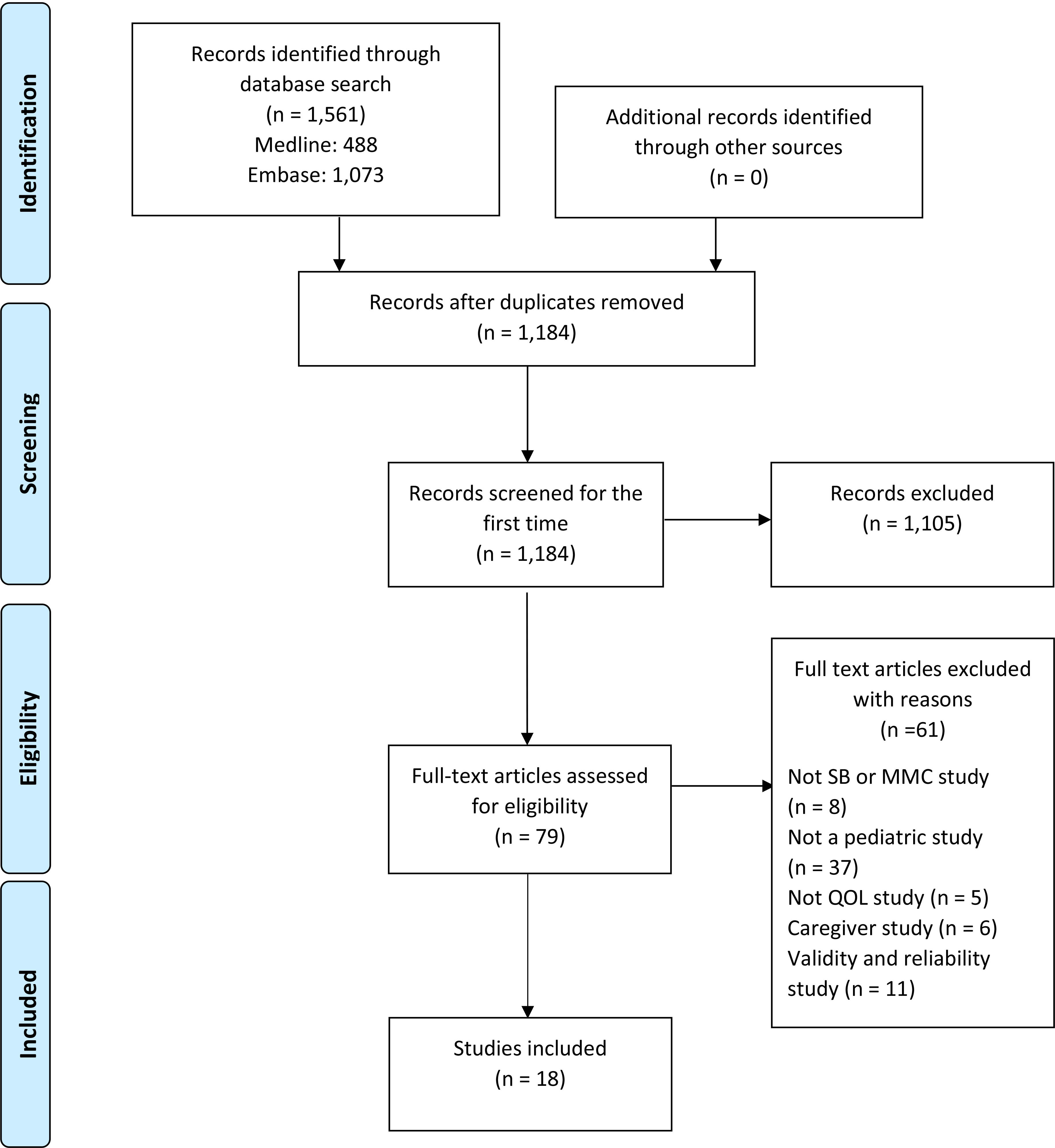
A systematic review was conducted consistent with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines [27]. Using the MEDLINE (PubMed) and EMBASE databases, we performed a search of all articles published from 2000 to September 14, 2018, using the following terms: ‘spina bifida’, ‘meningomyelocele’, ‘spinal dysraph-ism’ AND ‘quality of life’, ‘adaptation/physiological’, ‘activities/social’, ‘activities/physical’, ‘activities of daily living’, ‘well-being’, ‘personal satisfaction’, ‘social adjustment’ in diverse combinations following MeSH search strategies described by McKibbon et al. [28]. A secondary search included examining the reference lists of all included articles; we also used Google Scholar to complete our inquiry of recently published studies. The results were restricted toEnglish- and Spanish-language publications. The inclusion criteria were: (1) participants: children and adolescents (5–21 years of age) with SB and/or MMC; (2) quantitative studies; (3) outcome: HRQOL clearly measured by validated instrument determinants; and (4) US-based studies. Validation studies, case reports, conference abstracts, editorials, review articles, and animal studies were excluded. Studies that included fewer than six individuals with SB as a subset of a population also were excluded. The titles and abstracts were independently screened by two authors. After full-text articles were retrieved for eligibility, incongruences were presented to the third author, and consensus was reached through discussion. Articles meeting inclusion criteria were assessed and mapped to the focused conceptual framework informing the study (i.e., SDH). Demographic information on each study’s primary catchment county (or state when applicable) was obtained from the US Census [29]. Methods of the analysis and inclusion criteria were specified in advance and documented in a review protocol which is available upon request.
Summary of quality of life studies in children and adolescents with spina bifida, with annotations regarding the inclusion of cultural context
Summary of quality of life studies in children and adolescents with spina bifida, with annotations regarding the inclusion of cultural context
In accordance with PRISMA guidelines, 1,184 articles were identified, of which eighteen US-based studies met the inclusion criteria for the systematic review (Fig. 1).
Generic vs. SB-specific QOL instruments
In these 18 studies, eight different QOL instruments were used (Table 1). The generic (non-condition specific) Pediatric Quality of Life Inventory (PedsQL 4.0) emerged as the instrument most commonly used (
Social determinant of health: Language as cultural context
Of the 18 articles, a subset of 12 (67%) articles reported demographic information related to race/ethnic-ity. Within the 12 articles that reported this demographic information, only seven articles included Hispanics/Latinos. Of these seven, a single study reported 68.2% of its participants as being Hispanics/Lati-nos [35]; however, the remaining studies reported a smaller proportion of Hispanics/Latinos (range
The majority of the QOL studies excluded or did not mention including Spanish-speaking individuals. Of the six (33%) studies that reported inclusion of Spanish-speaking individuals, all used a Spanish version of the generic PedsQL 4.0, and two collaborating studies used an additional SB-HRQOL instrument that the authors reported to have translated at their institutions to complement the generic measure [42, 44]. Also, along with these studies, a third reported having a bilingual research assistant [42] to aid with the consent and administration of the surveys to Spanish-speaking parents. No other type of assistance for Spanish-speaking families was described in the remaining publications.
Social determinant of health: Health care services
QOL instruments were also used to examine the influence of accessed surgical services and/or extant mental health on QOL among children and adolescents with SB. Three studies described exploring the influence of surgical procedures such as: the antegrade continence enema procedure (ACE) [45], urinary and fecal incontinence reconstruction surgery [37], reconstructive urological surgery such as augmentation with or without a Mitrofanoff procedure and ACE, and bladder neck reconstruction on QOL [30]. Generic QOL instruments (PedsQL 4.0 and GCBI) were used for two of these three studies. Along with the FICQOL [45], these SB-specific and generic instruments demonstrated changes in QOL following surgery, with post-surgical improvements in HRQOL noted in all three studies. Additionally, since mental health has been reported as a mediator of QOL among children and adolescents [47], two studies incorporated an assessment of mental health (i.e., depression and anxiety) using either the Beck Depression Inventory (BDI) or a subdomain of the FICQOL survey. Flanagan et al. [34] observed that children and adolescents with SB tended to report lower QOL and increased depressive symptoms in comparison to peers with spinal cord injury (SCI) as measured by the BDI. Additionally, Ok et al. [45] reported an overall improvement of QOL and decreased depressive symptoms after the ACE procedure was performed, using the FICQOL.
Lastly, two studies reported on cognitive function outcomes with regard to QOL. In a study by Wasserman and Holmbeck [41], cognitive ability was assessed using the Wechsler Abbreviated Scale of Intelligence (WASI) and subtests from the Wide Range Achievement Tests 3 (WRAT3), the Cognitive Assessment System (CAS), the Delis Kaplan Executive Function System (D-KEFS), the Test of Everyday Attention for Children (TEA-Ch), the Diagnostic Analysis of Nonverbal Accuracy 2 (DANVA2), and the Comprehensive Assessment of Spoken Language (CASL). The results from this study revealed qualitatively different cognitive profiles among children with SB, which ultimately related to physical QOL. Driscoll et al. [42] assessed cognitive ability using the WASI but did not observe a significant relation to self-reported or proxy-report HRQOL scores measured on the generic PedsQL 4.0. This study reported on parenting stress as consistently being the most strongly associated with parent proxy-report of youth HRQOL.
Discussion
Our findings document that individuals living with SB face many factors that negatively impact their reported QOL; these challenges, as well as the QOL instruments used to assess them, are wide-ranging. Along with physical domains, a number of additional factors were associated with lower HRQOL scores; the investigation and understanding of these factors as a basis to develop interventions designed to improve QOL emerged as an important pursuit. Consistent with previous reviews of HRQOL in patients with SB [26, 48], our findings demonstrated that most studies were cross-sectional in nature and described varying degrees of HRQOL divergence on parent and self-reported scores related to emotional, social, and school domains (Table 1). Moreover, a generic measure of QOL was utilized by the majority of studies (
Thus, current research reasoning has evolved into calling for suitable QOL psychometric instruments that are condition-specific and clinically validated assessment tools that also value individuals’ perceptions of their HRQOL rather than unduly focusing on physical function [48, 49]. The SB-specific QOL instruments are more appropriate for individuals with SB because they offer insight into the person’s perspective on QOL. Instruments that increasingly incorporate the individual’s perception ask relevant questions related to self-esteem, independence, relationships, and bladder/bowel function, which are essential contributors to overall QOL [9]; in part, SB-specific QOL measures aim to quantify QOL through questions regarding embarrassment, lifestyle, and coping behaviors related to self-catheterization as well as incontinence. Conversely, generic QOL instruments fail to address concerns related to common SB symptoms and focus more on questions such as ambulation. Nonetheless, in our review, the generic PedsQL 4.0 questionnaire was found to be the most pervasive instrument used to measure QOL in individuals with SB. By contrast, only a minority of studies documented solely utilizing a SB-specific instrument for assessment [13, 45, 46].
The role that cultural context, as a SDH, plays in the outcomes related to chronic health conditions has long been identified [16, 50, 51, 52]. In particular, language plays a key role as a factor associated with outcomes among Hispanics/Latinos [53, 54]. Given the fundamental nature of language, we focused on it as a primary SDH. Health disparities research suggests that among some specific racial/ethnic groups, inferior health status may be explained partly by divergent SDH (e.g., social gradients, social exclusion, and changes in the health care system) [55]. It is also acknowledged that in order to properly address gaps in providing care for patients with SB, a national research strategy must be multi-centered, longitudinal, and inclusive of ethnic and socioeconomic diversity [56]. Promisingly, investigators have also begun to recognize existing disparities through the use of the National Spina Bifida Patient Registry (NSBPR) – a partnership between the CDC and SB clinics throughout the US. Schechter et al. [57], established that non-Hispanic blacks were less likely than the other groups to have documented bladder/bowel continence, as also were Hispanics/Latinos less likely than non-Hispanics. The authors went on to state that after controlling for SB-related intrinsic characteristics, significant variations in outcomes associated with age, gender, race/ethnicity, and insurance status remained. They demonstrated that non-Hispanic blacks, Hispanics/Latinos, and those without private insurance had less favorable outcomes. A second NSBPR study recognized that the likelihood of having bladder continence was significantly higher among non-Hispanic whites and those with private insurance [58]. A third NSBPR study demonstrated that non-Hispanic white race/ethnicity and private insurance were associated with an increased likelihood of receiving surgical services to treat neurogenic bowel (e.g., ACE procedure) [59].
In the face of these health disparities, the timely and proper study of QOL among the Hispanic/Latino population, which has the highest SB prevalence [1], is clear. Furthermore, it has long been recognized that measuring outcome indicators based on the differing cultural aspects of well-being – indicators such as QOL – is crucial [15]. In a previous study beyond health measures alone, Chowanadisai et al. [60] found that well-being assessment, such as satisfaction with health care, is significantly lower among Hispanics/Latinos with SB, even after controlling for socioeconomic status. Since the multidimensional conceptual understanding of an individual’s own QOL is thought to be profoundly impacted by the intrinsic cultural context [52, 63], health professionals are called upon to consider the impact of culture, ethnicity, and immigration status on QOL [61] in an increasingly ethnically diverse society. Additionally, even after adjustment for family income and parental education, language and culture are known to contribute to the disparities in health outcomes found among Hispanics/Latinos [64]. However, even though it has been demonstrated that culturally sensitive interventions improve QOL and outcomes among Hispanic/Latino children with chronic health conditions [65] and it has been further postulated that such an approach may benefit children with SB [60], efforts towards this goal are nascent in SB care [66].
Whereas researchers utilized supplementary assessment measures to investigate additional dimensions (e.g., stress, anxiety, depression, cognitive function) that theoretically could impact QOL [36, 41, 42, 45], in our US-based review where an estimated 55 million Hispanics/Latinos live, we found no study that probed cultural aspects (e.g., language, acculturation, immigration, etc.) as potential modifiers on QOL. In fact, within the largest minority group and the fastest growing US population segment [25], among whom nearly 75% of individuals speak Spanish at home [25], there is a dearth of research on HRQOL among those living with SB. Of the 18 QOL studies identified, only six (33%) reported including Spanish-speaking individuals. In these studies, a generic QOL measure was used, at times supplemented with an ad hoc translation of a condition-specific tool. Although some initial steps were taken to address culturally-appropriate care [42, 43, 44], further work is needed. Despite Congress’ previous efforts to safeguard adequate representation of ethnic and racial minorities in federally funded research, our review failed to identify an adequate culturally validated Spanish-language, SB-specific QOL instrument; this goal is especially relevant to parents and to new immigrants providing self-report. As we grow in our understanding of immigration as a SDH and its effects on health and well-being [67], this gap also becomes self-evident.
Of note, the literature reviewed showed no consistent expression to describe people whose ancestry could be traced to the Spanish-speaking regions of Latin America, including the Caribbean, Mexico, Central America, and South America. Moreover, in some instances, even the term “Spanish origin” was used [36]. Such terminology “places narrow and undue emphasis on the European influence of Spanish colonialism” [68]; thus, the root term Latino would have been preferable.
The authors acknowledge several limitations common to systematic reviews. Inherent limitations exist due to the nature of synthesizing large datasets. To reduce some of these limitations, such as selection bias and inclusion of irrelevant validity/reliability results, a very stringent search criteria was implemented by two reviewers who assessed all studies in accordance with PRISMA guidelines. A second limitation of this review may be that as language and culture were not primary outcomes for many of the QOL studies, they may not have reported all relevant information due to journal limitations or the perception of this information as irrelevant. It is possible that studies that did not report any demographic information did in fact include Hispanics/Latinos or had few Hispanics/Latinos in the community. To address this limitation, we provided county census data [29] relevant to each study site to provide a crude contextual proxy of the percentage of Hispanics/Latinos in the primary catchment area where the research was conducted (Table 1). A third limitation arises from the heterogeneity of the populations (e.g., spinal cord injury) included in the reviewed studies. However, to ensure that we appropriately represented individuals with SB, we did not include any studies with relatively few participants with SB (i.e. studies with less than six participants with SB).
Since its inception [69], those evaluating QOL among individuals with SB have done a remarkable job in developing and moving forward this effort and its associated body of literature. However, these gains have not translated equally to all segments of the SB population. As a starting place, we would encourage the SB research community to include Hispanics/Latinos in QOL studies and conduct interviews and questionnaires in their primary language. After this step is taken, other means will be needed to further delve into additional SDH, health beliefs, and health literacy. Future QOL research should not only take preferred language into account, but it should also explore other dimensions keenly relevant to immigrants such as levels of family support, acculturation, adverse childhood experiences, and resilience.
To our knowledge, this is the first study to summarize the US-based QOL literature under a SDH conceptual framework and to identify gaps in the implementation of these efforts among the population most prevalently affected by SB [1]. Recently, in March 2017, the Spina Bifida Association brought together content experts to update the SB-healthcare guidelines [70]. As these guidelines – comprising 25 areas of care delivery – are implemented, fresh momentum towards the employment of HRQOL measures is likely to ensue. Therefore, nationally we now have renewed guidance and have the opportunity to care for all individuals and parents as whole-persons as they transition across the lifespan [13], not only addressing the medical condition but also holistically approaching them in their language and cultural context.
Conclusions
“Blue marble health” was introduced in 2013 as a policy framework to illustrate trends in the geographic distribution of neglected tropical diseases affecting at-risk populations that live not only in low-income countries but also in pockets of the populace in wealthier nations [71]. Since that time, it has been noted that this framework may also have a role in illustrating the SB paradigm in a high-income nation such as the US [72]. Globally, since 2000 there has been a 49% increase in immigration [22], thus linguistically-congruous study of QOL has enlarging relevance not only locally, but also abroad. In the US, in spite of Congress’s NIH Revitalization Act of 1993, calling for efforts to ensure that minority groups are included in representative numbers in research studies and that Hispanics/ Latinos have the highest reported prevalence of SB, few HRQOL studies have documented inclusion of this population. According to the most recent US Census forecasts on immigration and birth, this demographic group will increase from 17.4% to 28.6% of the total population in the approaching decades; hence, future research should include cultural context as a component in the study of the HRQOL construct and support the utilization of validated Spanish-language measures for its investigation.
Footnotes
Acknowledgments
The authors thank Dr. Monica Gramatges in the Department of Pediatrics, Hematology/Oncology section at Texas Children’s Hospital and Dr. Robert G. Voigt, Chief of the Meyer Center for Developmental Pediatrics, Texas Children’s Hospital for their support of this work. We also thank Dr. B. Lee Ligon of the Department of Pediatrics, Center for Research, Innovation and Scholarship, Baylor College of Medicine, for editorial assistance. Additionally, we are deeply grateful for the countless individuals and their family members who participated in the research reviewed, without whom progress in the field would not be possible.
Conflict of interest
The authors declare that they have no conflicts of interest.