
Abstract
PURPOSE:
To understand the relationship of walking speed to self-reported pain, fatigue, and physical function in adults with CP.
METHODS:
Design: Cross-sectional study.
Setting: Accredited clinical motion analysis laboratory in a regional children’s hospital.
Participants: 72 ambulatory patients
Main Outcome Measures: PROMIS-57 pain interference/intensity, physical function, and fatigue measures and walking speed.
RESULTS:
Physical function was significantly lower than able-bodied normal values by 1–2 standard deviations (40.3
CONCLUSIONS:
Self-reported physical function correlates with objectively measured walking speed in young adults with CP while patient-reported pain and fatigue did not, contrary to what would be predicted by the literature.
Introduction
Cerebral palsy (CP) is a non-progressive condition that arises from a neonatal/perinatal insult to the brain, resulting in poor neuromuscular control. While the injury to the central nervous system does not change, the secondary effects on the body do evolve. Adults with CP are at risk for accelerated degenerative musculoskeletal changes with aging due to abnormal biomechanics. Poorly aligned joints generate improper forces, leading to areas of excessive load [1]. This creates shear stress in atypical areas, resulting in mechanical cartilage degradation and the possibility of early osteoarthritis [1, 2]. Altered biomechanics leave individuals susceptible to overuse injuries and contribute to significant pain in ambulatory adults with CP [3, 4]. Based on our 20-year experience measuring gait biomechanics and overall gait performance in individuals with CP, we feel that there is reason to be concerned that decreased walking performance may directly contribute to health decline as individuals with CP transition into adulthood. This theory is supported by work by Opheim et al., which showed that ambulatory adults with CP who reported deterioration in walking also reported increased pain intensity and frequency, pain interference with ADLs, physical fatigue, and reduced balance [5].
There are numerous survey-based studies in which a disproportionate prevalence of pain is reported by individuals with CP relative to the normal population, with 18% to 51% reporting daily (i.e., chronic) pain [4, 6]. The high level of daily chronic pain is not surprising considering the biomechanical disadvantages. Indeed, adults with CP identify muscle and joint pain as a key factor to decreased weight bearing status and walking endurance with advancing age [4, 7]. This may explain why adults with CP report that their ability to walk both indoors and outdoors diminishes as they age [8]. Unfortunately, a decline in ambulation may inhibit people with CP from participating in their social communities and, in theory, worsen their cardiovascular health [9]. In addition to increased pain, individuals with CP report higher amounts of fatigue than the general population [10, 11]. Excessive fatigue has, in turn, been reported to contribute to decreased functional ambulation in adults with CP [12]. The high prevalence of pain and fatigue, and their adverse impacts on ambulation, have potential implications concerning general health and quality of life.
An individual’s experience of pain or fatigue is difficult to quantify. However, these are essential variables to consider in the treatment of adults with CP. One way to evaluate pain and fatigue is through use of Patient-Reported Outcomes (PROs). PROs are becoming an integral part of medical research as a representation of a patient’s disease experience, functional status, and health-related quality-of-life [13]. There are numerous PROs measures available. However, until recently a standardized format for PROs was lacking. A relatively new tool from the NIH, known as the Patient Reported Outcomes Measurement Information System (PROMIS), has indices that assess multiple domains including physical function, fatigue, and pain interference over the seven days prior to administration [14, 15, 16]. The PROMIS is a unique tool, as it provides a standardized method for quantification of patient reported data which may facilitate comparison of outcomes with future studies [17].
Since pain, fatigue, and physical function are subjective, it is informative to combine PROs with a quantifiable measure of function that is independent of patient or evaluator disease perception or bias. One way to accomplish this is by using an individual’s gait speed as an indicator of overall health status. While this seems like a simple measure, there is a large body of literature that correlates gait speed with overall function, health status, and ability to participate in social activities [18]. Particularly in the geriatric population, walking speed is a known predictive marker of overall health status and ambulation capability (e.g., household ambulator versus community ambulator) [18]. Although there is little known about its relevance in CP, one might reasonably suggest that it may be a marker for health as well. Indeed, health issues that influence motor function and the musculoskeletal system appear to manifest prematurely in adults with CP. It is also important to recognize that many health problems that affect older individuals are present in adults with CP such as metabolic syndrome, cardiovascular disease, obesity, and frailty [19, 20]. Recent work from our group shows that the prevalence of cardiovascular disease risk factors in the adult CP population seems to be triggered by decreased walking ability [19]. In addition, gait speed is important for the ability to function in community environments, such as the capacity to get across a busy intersection. Surprisingly, despite the ease of this measure and an abundance of literature identifying the importance of gait speed as an indicator of health status in other populations, there are no previous studies investigating gait speed as a predictive measure of physical function or health status in the cerebral palsy population [21].
In this report, we explore the relationship of PROMIS self-reported pain, fatigue, and physical function to walking speed in individuals with CP who participated in a prospective cross-sectional study. This study examined whether subjective experiences of pain and fatigue relate to objectively measured walking speed in adults with CP, as well as the relationship of these factors to overall self-reported physical function. We hypothesized that walking speed would be directly associated with self-reported function, pain interference and fatigue as assessed by the PROMIS-57. We also hypothesized that fatigue could be directly associated with walking speed, physical function, and pain, essentially acting as a confounder. As such, we chose to look at fatigue as a secondary outcome. Our group’s overall goal is to develop an evidence-based theoretical model to elucidate the mechanisms of health decline in CP as they relate to decreased walking performance. Understanding the role of self-perceived pain, fatigue, and physical function will help us better treat patients with CP from a whole-person perspective.
Methods
Setting and study design
This cross-sectional analysis was part of a larger longitudinal study analyzing changes in the walking ability and patterns of individuals with CP as they transition from the pediatric to the adult health care system. The study was conducted at an accredited clinical motion analysis laboratory in a regional children’s hospital from July 2014 to November 2017. The facility, composed of a specialized team of clinicians and researchers, has been serving the health needs of individuals with CP and providing Instrumented Gait Analysis (IGA) since 1999, and is nationally accredited by the Commission for Motion Laboratory Accreditation, Inc. (CMLA). The study was approved by an Institutional Review Board and all participants signed informed consent prior to participation.
A potential participant list was obtained from the laboratory patient registry and screened for inclusion criteria. Inclusion criteria consisted of adults aged 18 years of age or older, who were diagnosed with CP, who had a previous IGA at our institution during childhood and who were able to walk at the time of recruitment (i.e., GMFCS Level I–III). Enrolled participants completed cognitive testing, blood work, a full IGA, muscle strength testing, fatigue testing, and quality of life surveys, which were performed throughout three visits at the study site. The three study visits were completed within 4 weeks of each other. While only walking speed is discussed in this report, the data for each participant was extracted from a full IGA obtained as part of a larger study of health outcomes and gait changes in adults with CP. Please also refer to Table 1.
Main variable outcomes
Pain interference, physical function, and fatigue
PROMIS-57 has been developed as a set of measures to evaluate and monitor the mental, physical, and social health of children and adults across health conditions [14, 15, 16]. The PROMIS-57 Pain Interference (PROMIS-57 PI) measure reflects the self-reported or proxy-reported impact of pain (over the past 7 days) during engagement in social, physical, and recreational activities. Higher scores indicate more substantial pain interference. The PROMIS-57 Pain Intensity measure (embedded in the PROMIS-57 PI) reflects the self-reported or proxy-reported severity of pain (over the past 7 days) experienced in the PROMIS-57 PI. The scale is scored 0–10, in which 0 represents no pain and 10 is the worst pain imaginable. The PROMIS-57 Physical Function (PROMIS-57 PF) subscale reflects an individual’s self-reported or proxy-reported ability to accomplish daily activities, such as household chores and walking for 15 minutes. Higher scores indicate more physical activity. The PROMIS-57 Fatigue (PROMIS-57 F) subscale reflects the effect of an individual’s self-reported fatigue (over the past 7 days) on the ability to perform daily activities and function in his/her family and social roles. Higher scores indicate increased levels of fatigue. The PROMIS-57 PI, PROMIS-57 PF and PROMIS-57 F measures have been validated in multiple populations [22, 23, 24]. Scores from the PROMIS-57 can be converted to standardized T scores. PROMIS-57 norms for these scales are based on the general population with the average T score set at 50 with a standard deviation (SD) of 10. Much of the general population data was collected from the 2000 United States general census (please see
Walking speed
Each subject was tested at our clinical motion laboratory and followed a standardized clinical protocol that included a complete IGA consistent with the parent study, although in this report only walking speed was used in the analysis. One IGA-trained physical therapist performed all gait analyses in this cohort, responsible for placing retro-reflective markers and guiding the subject through the procedure. Fifteen tracking markers were placed on the pelvis and lower extremities in accordance with the Conventional Gait Model (CGM). A 13-camera Vicon motion capture system that included 10 Bertec force platforms were used to collect all 3D joint kinematics, kinetics and temporal-spatial parameters. Participants walked 5–8 times across the 10-meter calibrated walkway, with each “valid” pass identified as an individual walking trial. Passes were accepted as “valid” if the subjects walked without tripping and in a manner consistent with their typical pattern as determined by the observing physical therapist. Custom software in MATLAB identified a single representative walking trial for each subject, determined as the trial with the lowest composite residual across all 3D kinematics when compared to the average gait kinematics of all valid trials collected. The average walking speed of the representative trial, normalized to height (statures/min) was used in this analysis.
Statistical methods
Descriptive statistics (means, SDs, and percentages) were used to summarize continuous variables and categorical variables respectively. Raw fatigue, physical function, and pain interference scores were mapped to a t-score using tables in the PROMIS-57 manual [25]. These t-scores have a mean of 50 and a SD of 10 for the general population. The t-scores were correlated with normalized walking speed using simple and multiple linear regression analysis. A backward selection method was used to determine the final model. Pain intensity scale was treated as a continuous variable. Sensitivity analysis, which dichotomized the pain intensity score, produced consistent results similar to those with continuous intensity. Spearman correlations were reported for pain intensity with others variables. Pearson correlations were reported for other outcomes. SAS 9.4 (SAS institute Inc.) was used for all of the analyses. A
T-scores for PROMIS-57 physical function, pain interference and fatigue.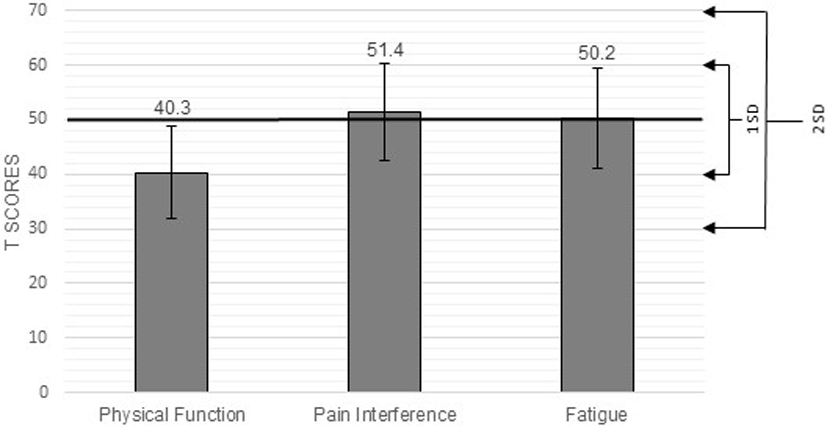
Correlation between walking speed and T-score of the PROMIS-57 fatigue, physical function, pain interference and pain intensity sub-domains. Figure 2A is the linear regression between walking speed and physical function sub-domain. Figure 2B is the linear regression between walking speed and pain interference sub-domain. Figure 2C is the linear regression between walking speed and fatigue sub-domain. Figure 2D is the linear regression between walking speed and pain intensity sub-domain.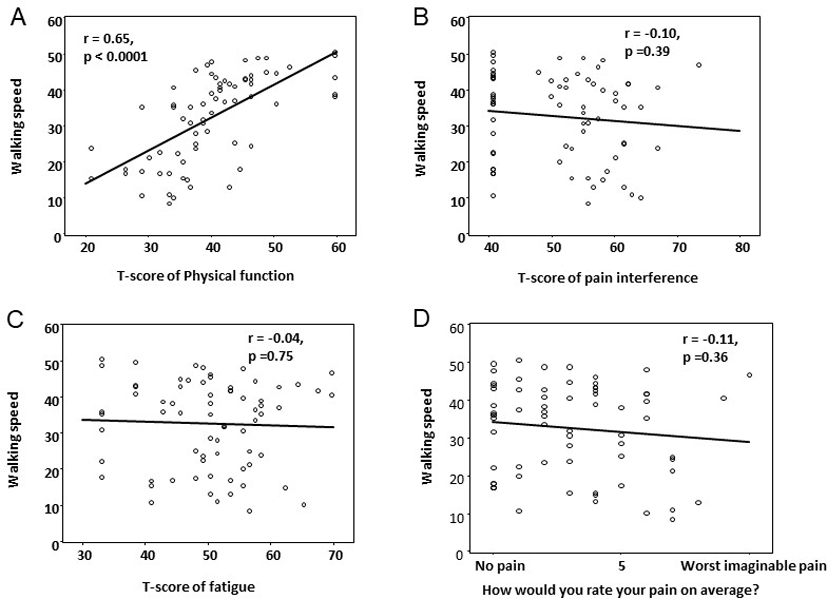
Correlation between T-score of the PROMIS-57 fatigue sub-domain and the PROMIS pain interference, PROMIS pain intensity, PROMIS physical function, and walking speed. Figure 3A is the linear regression between PROMIS-57 fatigue sub-domain and physical function sub-domain. Figure 3B is the linear regression between PROMIS-57 fatigue sub-domain and pain interference sub-domain. Figure 3C is the linear regression between PROMIS-57 fatigue sub-domain and pain intensity sub-domain. Figure 3D is the linear regression between PROMIS-57 fatigue sub-domain and walking speed.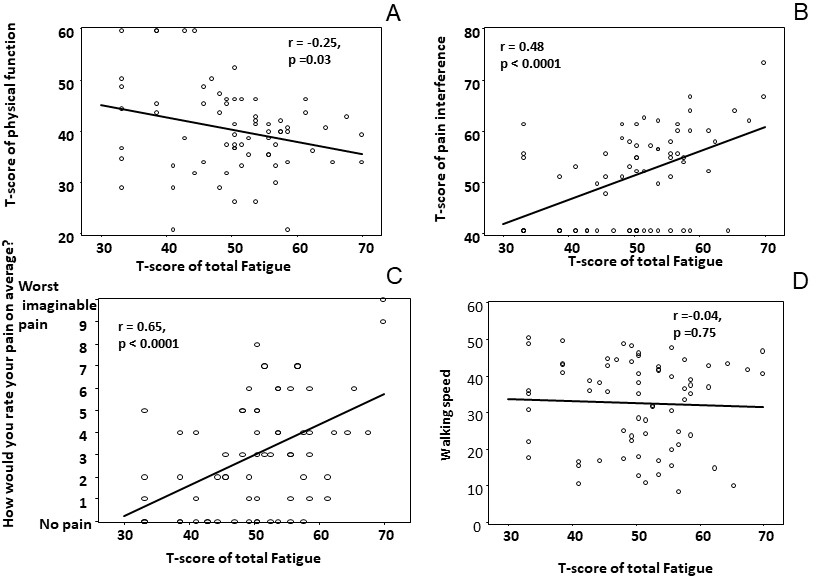
A total of 72 patients participated in this study. However, two participants were excluded from this analysis due to lack of completion of the physical function and pain interference sub-scores. Specifically, one had a missing physical function score and another had a missing pain interference score. Table 1 shows the summary statistics for the demographics and diagnoses of the 70 participants. Roughly 65% of our participants could complete the PROMIS independently, while roughly 35% of the responses were provided by a proxy. The average walking speed measured in statures per minute was 32.5
When looking at the individual variables (Fig. 1), physical function was significantly lower than normal values by 1–2 standard deviations (40.3
Discussion
In this group of young adults with CP, self-reported physical function directly correlated with walking speed. Indeed, 42% of walking speed variance was accounted for by perceived physical function. This may be associated with the fact that the PROMIS PF questions relate directly to activities that generally are accomplished through independent ambulation, such as the performance of household chores, navigating stairs, and shopping. An association between walking speed and the ability to perform activities that require mobility has been well established in community-dwelling older healthy adults but has not, to our knowledge, been specifically reported for adults with CP [13, 21].
The literature suggests that fatigue and pain are prevalent in, and adversely impact the function of, individuals with CP. However, pain interference and fatigue in our study population were not significantly different when compared to normal values on the PROMIS-57. Based upon a body of literature that suggests a high prevalence of pain and fatigue in adults with CP, this was an unexpected finding and may reflect selection bias toward higher functioning individuals in our study group [4, 5, 6, 7, 10, 11, 12]. On the other hand, the PROMIS-57 norms were obtained from a broad age range (i.e., 18–64 years old), while the average age of our subjects was 24.6
Self-reported fatigue and pain interference did not predict walking speed in this younger cohort of adults with CP [5, 26, 27, 28]. This may be an artifact of study design, since the PROMIS-57 is structured to elicit information about the 7 day period preceding the survey. The IGAs were conducted during a study visit independent of the PROMIS-57 administration and the study visits were separated by 3 weeks on average. It is conceivable that participants had less pain and fatigue on the days that walking speed was measured. Furthermore, 14.3% of the participants reported use of non-steroidal anti-inflammatory medication. While we do not know what medications the participants took on the study visit days, it is possible that analgesic use increased in preparation for the IGAs or perhaps participants rested in a prophylactic manner prior to the studies. Interestingly, those who reported a higher pain intensity also reported using significantly more non-steroidal anti-inflammatory medication. This might explain the reason that we did not, to our surprise, see a strong correlation between pain interference and gait speed. Additionally, it is possible that the participants interpreted the wording of the PROMIS F and PROMIS PI measures idiosyncratically. The wording of the PROMIS F subscale is particularly abstract. Conversely, the PROMIS PF questions are much more concrete and possibly leave less room for interpretation. Prior work with the PROMIS Pediatric Measures suggested that individuals aged 8–21 with CP may have interpreted the questions differently than the PROMIS Pediatric reference group [29].
We found that self-reported physical function correlated with walking speed which, in turn, we may reasonably extrapolate to predict overall health. In this light, it is concerning to note that the mean reported physical function is 40.3, which is more than one standard deviation below the general population norm, despite having a relatively healthy young adult CP population. The normal values in the PROMIS-57 are generated from adults 18–64 years old based on the 2000 US census data. Therefore, the mean age of the reference group of healthy adults is presumably older than our measured CP population. Hence, it is possible that our results would be even more dramatic if we used age matched normal values, as our group had a mean age of 24.6
Patient reported outcomes (PROs) have emerged as an important source of information regarding health-related issues that impact function and quality of life. Unlike traditional research outcomes (e.g., mortality and morbidity measures), PROs comprehensively capture a patient’s disease experience, functional status and health-related quality-of-life [14, 31]. The NIH has developed the PROMIS to provide researchers with a validated tool for investigating life domains (
Study limitations
There were several potential limitations to this study. The participants were recruited from a database of individuals with CP who had previously undergone IGA in our laboratory. This was done under the protocol from a larger observational study investigating the relationship between changes in gait characteristics and a variety of health outcomes for persons aging with CP. Given the potentially selective nature of our study population, we recommend caution in generalizing the results of our study. Another limitation is the issue of parent-proxy answers. From all surveys, self-reported PROs and parent proxy can differ tremendously. This study did not account for this issue, as the number of parent proxy was low (three cases).
Additionally, the PROMIS-57 has not been validated for young adults with CP. The mean age of the PROMIS-57 reference group is not provided in the supporting literature, and the data is not available to use an age matched normal group for comparison. This makes it difficult to tell the degree to which our group of young adults might deviate from age matched normal community dwelling young adults in terms of pain, fatigue, and physical function. Additionally, pain interference and fatigue (per PROMIS) were only rated for the previous 7 days. We do not know whether the self-reported pain interference is representative of a relatively stable state (i.e., chronic pain) or an acute monophasic occurrence that happened within the week of their participation in this study. Based upon prior literature, it would be expected that a portion (perhaps 1/5th) of participants might have been reporting about chronic pain [30]. Due to the design of the study and outcome measures, we do not know how much pain the participants had, the location of pain, the type of pain (e.g., musculoskeletal, neuropathic) or whether they took pain medications on the day of their gait analysis. We suspect but cannot verify that subjects reporting pain were referring to pain of musculoskeletal origin, as this is the most common source of pain in CP [26].
Conclusions
This paper is the first to look at patient reported outcomes in adults with CP with a focus on walking speed. Our goal was to understand how a patient’s disease experience as measured by the PROMIS-57 relates to objectively measured walking speed, which we are using as a proxy for overall health status. We have shown that the PROMIS-57 PF scores significantly correlate with walking speed, however, PROMIS-57 PI and F do not. The questions in the fatigue and pain interference questionnaires are rather vague and can result in variable interpretation, which may help to explain their lack of correlation with gait speed. On the other hand, the physical function questionnaire asks concrete questions that do not leave as much room for interpretation. While pain and fatigue clearly play a large role in quality of life, we were unable to find a direct association with walking speed in this cohort of healthy, relatively young adults with CP during this sample period. Our intention is to follow this cohort prospectively to further delineate the relationships between pain, fatigue, overall physical function and gait performance in adults with CP as they age with this pediatric onset condition.
Footnotes
Acknowledgments
The authors wish to acknowledge the important contributions of the CPAT co-investigator team (Amy Bodkin, Tim Boyd, Meghan Colip, Tatiana Oliveira, Tim Reistetter, David Robertson, and Pam Wilson), the CP team at Children’s Hospital Colorado led by Dr. Frank Chang, and the faculty/staff of CGMA. This research was supported by grants from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR #H133G130200, NIDILRR #90IF0055-01), in the Administration for Community Living (ACL) of the Department of Health and Human Services (HHS). Additional support was provided from the J. T. Tai and Company Foundation.
Conflict of interest
The authors have no conflicts of interest to report.