
Abstract
PURPOSE:
To describe the incidence and risk factors of communication, swallowing, and orofacial myofunctional disorders in a cohort of children and adolescents with cancer and benign neoplasms.
METHODS:
A prospective cohort study conducted with children aged
RESULTS:
One hundred and sixty individuals were evaluated. At the time of hospital admission, 68 individuals (42.5%) presented with some type of SLP disorder. After one year of follow-up, 22.8% of the patients had developed new impairments. The occurrence of new speech-language disorders had a statistically significant association with the tumor site. In the risk analysis for the development of speech-language disorders with respect to the primary tumor site, compared to other sites, the central nervous system (CNS) tumor group was 8.29 times more likely to present some new alterations, while the head and neck (HN) tumor group had a 10.36-fold higher risk.
CONCLUSION:
An incidence of 22.8% for communication, swallowing, and orofacial myofunctional disorders was observed. The development of these disorders was greater in individuals with tumors in the CNS and in the HN region.
Keywords
Introduction
Pediatric tumors correspond to a group of many diseases that present uncontrolled proliferation of abnormal cells and which can occur anywhere in the body [1]. Children and adolescents with cancer and benign neoplasms are at a greater risk of the development of communication, swallowing, and orofacial myofunctional disorders associated with the presence of tumors and, consequently, with their treatment [2, 3]. Those undergoing cancer treatment may present with hearing loss associated with exposure to ototoxic therapeutic agents such as platinum compounds and cranial irradiation. Auditory impairments can impact the development of speech, language, and communication, as well as social interaction, learning, and quality of life of these individuals [4, 5, 6].
Solid tumors in the central nervous system (CNS) are the most frequently found lesions in the pediatric age range, accounting for 8–15% of childhood and juvenile neoplasms [1, 7]. Individuals with CNS tumors may present with functional impairments associated with the involvement of certain structures by the lesion. Several studies have addressed the occurrence of speech, language, and swallowing impairments in children with neurological tumors [8, 9, 10, 11]. Dysphagia and dysarthria are common disorders in children with tumors localized in the posterior fossa because the neurological structures of this region play an important role in the accuracy and efficiency of the movements involved in speech and deglutition [8, 9, 13, 14]. Malignant and benign tumors in the head and neck (HN) region are also associated with the development of some functional disorders, namely dysphonia, dysphagia, temporomandibular joint disorder, dysacusis, and facial paralysis. In general, the disorder corresponds to the impairment caused by the presence of the tumor, and it may be aggravated by the treatment indicated for the disease [15, 16, 17].
Pediatric oncology patients often require speech-language pathology (SLP) intervention aimed at managing impairments in hearing, swallowing, voice, speech, language, and orofacial motricity. In the specific scientific literature, studies addressing the incidence of SLP disorders in heterogeneous groups of children with cancer and benign neoplasms are scarce, with a predominance of surveys involving groups of children with some specific cancer diagnosis, mainly neurological tumors [10, 12, 13, 14, 18]. In this context, the purpose of this study was to describe the incidence and risk factors of communication, swallowing, and orofacial myofunctional disorders in a cohort of children and adolescents with cancer and benign neoplasms.
Methods
This is a prospective cohort study conducted with children aged
Of the 213 patients recruited at the time of hospital admission, 53 individuals were excluded from the survey. The inclusion criterion was admission in the Pediatric Oncology Department of the Instituto Nacional de Câncer (INCA) and the exclusion criteria involved the patients who were not diagnosed with neoplasms or who did not maintain follow-up at the institution. Figure 1 depicts the flowchart of the research. The study sample was composed of 160 children and adolescents with solid tumors and benign neoplasms. During the study, monitoring was interrupted in 26 individuals due to death and in two patients who did not complete the assessment process (17.5%), but the data from the latter were used until the moment they participated.
Flowchart of the research.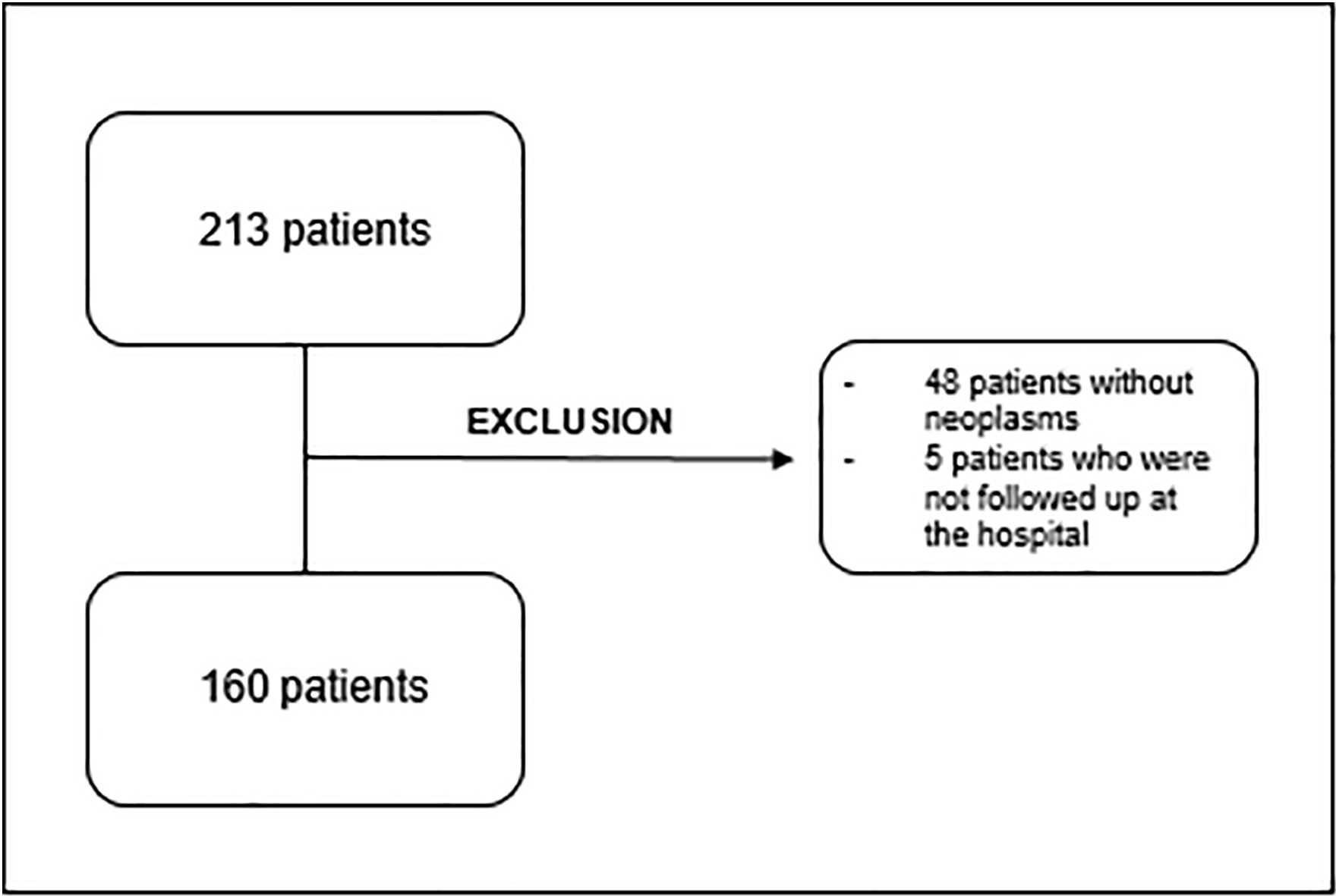
Study participants were evaluated at three different times: (T1) at hospital admission; (T2) six months after admission; and (T3) one year after admission. For data collection, an instrument prepared by the researchers was used for registration of sociodemographic and clinical information, anamnesis data, and findings of clinical speech-language pathology (SLP) assessment, which included aspects of the oral sensorimotor system, swallowing, speech, language, voice, and hearing. The evaluation instrument was developed based on some standardized assessments with the intention of reaching all aspects that were the focus of the study. The evaluations were conducted exclusively by the main researcher. In addition to the information obtained in the clinical assessment, data on the disease and treatments performed were obtained from the medical records of the patients.
Speech-language skills were evaluated through naming and spontaneous speech tasks registered by an audio recorder. Language assessment considered the following linguistic levels: phonological, morphosyntactic, semantic-lexical, and semantic-pragmatic.
The phoneme production characteristics observed in the tasks of spontaneous speech and naming were recorded in a set of phoneme frames and the phonological processes were analyzed based on the criteria established in the ABFW – Child Language Test for Phonology, Vocabulary, Fluency and Pragmatics [19]. The morphosyntactic level involved phrase structure analysis in spontaneous speech.
The ABFW vocabulary test was applied to evaluate the semantic-lexical
level [19] of the study participants. The
semantic-pragmatic evaluation included the observation of skills such as verbal initiative,
speech production with communicative function, speech coherence, conversation topic
maintenance, literal verbal utterance comprehension, and figurative language comprehension
in participants aged
With respect to speech, the characteristics of articulation, velocity, intelligibility and prosody were evaluated. Regarding the oral sensorimotor system, posture, strength, and mobility of orofacial structures and sensitivity of the face and tongue were observed.
Swallowing of saliva and food was also assessed. The functional evaluation of swallowing using food involved liquid and solid consistencies. Efficacy of lip seal, oral motor control, oral transit time, mastication, and hyolaryngeal movement was observed, and the presence of extra oral food escape, oral cavity stasis, nasal leakage, multiple swallowing, coughing, throat clearing, wet voice, dyspnea, and cyanosis were identified. Cervical auscultation was used during the evaluation of swallowing. The assessment also included the application of the Functional Oral Intake Scale (FOIS) [21].
Voice assessment comprised identification of the findings on vocal quality, loudness (subjective perception of sound pressure), pitch (subjective perception of frequency), vocal resonance, and pneumophonic coordination. The GRBASI (grade, roughness, breathiness, asthenia, strain, and instability) perceptual vocal scale was used [22].
As for the auditory function, considering that the institution where the study was conducted did not have an audiology service, participants who had undergone pure-tone audiometry less than a year before the initial time (T1) and patients who underwent audiological control throughout the treatment follow-up times (T2 and T3) had their reports recorded in the assessment protocol. Frequency of dysacusis was estimated considering only this group of patients.
Definition of the outcomes was based on the detection of normality patterns in all the parameters assessed (absence of impairment), or the detection of presence of impairment in the functions of language and speech (language disorder, articulation and phonological disorders, stuttering, aphasia, apraxia and dysarthria), voice (dysphonia), swallowing (dysphagia), orofacial motricity (orofacial myofunctional disorder, facial paralysis, trismus, and tongue paralysis) and hearing (dysacusis).
Neoplams were categorized according to the third edition of the International Classification of Cancer in Childhood (ICCC-3), which divides tumors into 12 major groups: I – Leukemias, myeloproliferative disease, and myelodysplastic diseases; II – Lymphomas and reticuloendothelial neoplasms; III – Central Nervous System (CNS) and miscellaneous intracranial and intraspinal neoplasms; IV – Neuroblastoma and other peripheral nerve cell tumors; V – Retinoblastoma; VI – Renal tumors; VII – Hepatic tumors; VIII – Malignant bone tumors; IX – Soft tissue and other extraosseous sarcomas; X – Germ cell tumors, trophoblastic tumors, and neoplasms of gonads; XI – Other malignant epithelial neoplasms and malignant melanomas; XII – Other and unspecified malignant neoplasms [23]. This classification includes some tumors of uncertain biological behavior regarding malignancy (borderline tumors), considering the modifications contained in the International Classification of Diseases for Oncology (ICD-O) [24].
For data analysis, in the classification of patients in groups by tumor category, patients with malignant and borderline tumors described in ICCC-3 were separated into 4 groups: CNS tumors (ICCC-3 category III); osseous tumors (ICCC-3 category VIII); soft tissue tumors (ICCC-3 category IX); and other solid tumors, including neuroblastoma, retinoblastoma, renal tumors, liver tumors, tumors of germ cells and other epithelial malignancies (ICCC-3 categories IV, V, VI, VII, X, and XI, respectively). Regarding analysis of the variable “Treatment performed”, the individuals were subdivided into 4 groups: surgery; surgery and chemotherapy; surgery, chemotherapy, and radiotherapy; and other regimens (radiochemotherapy, exclusive radiotherapy, and exclusive chemotherapy). In the evaluation of punctual prevalence, the number of cases, new and existing, of SLP disorders was considered at the assessment times (T1, T2, and T3). In the estimation of the incidence of a disorder throughout the follow-up period, participants who had already presented with the disorder at the initial evaluation (T1) were excluded from this analysis.
Descriptive statistical analyses of the quantitative and qualitative variables were performed by mean/standard deviation and absolute/relative frequencies, respectively. The Chi-squared test was applied for evaluation of the percentage differences between the outcomes and the independent variables considering a significance level of 5%. Univariate logistic regression was conducted to assess the risk of development of SLP disorders and their relation to site of the lesion by means of odds ratio (OR) and its respective 95% confidence interval. All statistical analyses were performed using the SPSS 23.0 software.
One hundred and sixty children and adolescents (73 males and 87 females) aged
2–17 years old (mean 9.24; SD
Sociodemographic characteristics
Sociodemographic characteristics
With respect to the clinical characteristics, 143 participants (89.4%) were diagnosed with malignant tumors or borderline tumors and 17 individuals (10.6%) presented with benign neoplasms (Table 2).
Clinical characteristics and treatments performed
Prevalence of speech-language disorders
The solid tumors most frequently observed in the group of children and adolescents analyzed were central nervous system (CNS) (ICCC category III) and osseous (ICCC category VIII) lesions, affecting 41 (29.5%) and 26 (18.3%) patients, respectively. As for site of the lesion, 43 patients presented with CNS tumors, 23 had lesions in the head and neck (HN) region and 94 presented with tumors in other sites (Table 2). The treatment regimen that included the largest number of individuals was the combination of surgery and chemotherapy, with 44 patients. Of the patients who underwent chemotherapy, 42.7% received cisplatin, an antineoplastic agent of high ototoxic potential [4].
Incidence of speech-language disorders in the follow-up
*The number of patients considered for analysis of the incidence of each disorder excludes those who already had the disorder in T1. **Only patients who underwent auditory evaluation over a year.
Table 3 shows the frequencies of the speech-language pathology (SLP) disorders investigated at the three assessment times. At hospital admission (T1), 68 individuals (42.5%) presented with some type of SLP disorder (data not shown in the tables). Orofacial myofunctional disorder, dysphonia, and language disorder were the most commonly found SLP impairments. Dysphagia, dysarthria, and facial paralysis, which are
Association of speech-language disorders and sociodemographic and clinical variables
disorders not usually found in healthy children and adolescents, were also observed in this group of individuals.
Participants who presented with a specific impairment at the initial assessment of the study were excluded from the analysis of incidence of that disorder throughout the follow-up period. Incidence of impairment over one year of monitoring was 22.8% (21 patients in the group of 92 individuals who had no disorders at baseline). Some individuals developed two or three new concomitant disorders and 59 new disorders were detected. New cases of articulation disorder, dysacusis, dysarthria, dysphagia, dysphonia, orofacial myofunctional disorder, facial paralysis, and tongue paralysis were observed (Table 4).
Table 5 shows the association between SLP disorders and the sociodemographic and clinical variables analyzed. No statistically significant correlation was found between the occurrence of articulation disorder, dysphonia, orofacial myofunctional disorder, and the sociodemographic and clinical variables investigated.
All new cases of dysarthria were observed in patients with malignant CNS tumors
(
Occurrence of facial and tongue paralyses was associated with site of the lesion and ICCC-3 category. Patients with these disorders presented with tumors localized in the CNS or in the HN region and belonged to ICCC-3 categories III and IX. One patient with facial paralysis had a benign neoplasm not categorized in the ICCC-3.
Of the 32 patients who underwent auditory monitoring for one year, five
individuals with CNS tumors developed dysacusis: three with lesions in the HN region and
five with tumors in other sites (
Regarding the treatments performed, incidence of dysphagia and dysarthria was
associated with the “Other Regimens” group (
A statistically significant association was found between the occurrence of new
SLP disorders and the site of the lesion (
To the best of our knowledge, this is the first study describing the incidence and risk factors of communication, swallowing, and orofacial myofunctional disorders in a heterogeneous group of children and adolescents with cancer and benign neoplasms by means of prospective analysis with follow-up of individuals for one year. In the literature, most of the studies addressing the frequency of speech-language pathology (SLP) disorders include groups of patients with some specific cancer diagnosis, mainly neurological tumors [10, 13], which hinders the comparison of our results with those of other similar surveys.
A retrospective study conducted in Australia [3] revealed the prevalence and severity of deglutition/feed-ing and communication disorders in children diagnosed with cancer and non-malignant hematological diseases followed up at a Speech-Language Pathology and Audiology Service. In the group of 70 patients analyzed, the authors observed the following types and percentages of SLP disorders: 44.3%, swallowing; 34.3%, receptive language; 38.6%, expressive language; 31.4%, speech; and 5.7%, voice.
In the present study, 83 patients presented with some type of speech-language impairment at the time of hospital admission. In this initial assessment, some typical developmental SLP disorders possibly unrelated to disease onset were observed, i.e., orofacial myofunctional, phonological, and language disorders. However, other observed impairments such as dysphagia, dysarthria, and facial paralysis are not common in healthy individuals and were likely associated with disease onset in the group studied [10, 11]. After a year of follow-up, new SLP impairments were detected in 41 patients (25.62%).
All new cases of dysarthria were observed in individuals with CNS tumors. In the literature, there are several studies reporting the occurrence of dysarthria in patients with neurological lesions, especially those localized in the posterior fossa [8, 9, 12, 25]. The posterior fossa, which includes the cerebellum, brainstem, basal ganglia, and the cortico-cerebellar connections, is the most common site of CNS tumors in children [8]. Astrocytomas and medulloblastomas localized in the cerebellum region account for approximately one-third of pediatric neurological tumors [12]. Presence of motor speech disorders (ataxic dysarthria) associated with cerebellar lesions has long been documented as part of the posterior fossa syndrome, which occurs in approximately 25% of children after resection of tumors in this site [9, 11, 25, 26, 27]. In addition to speech disorders, swallowing impairments are also common in patients with posterior fossa tumors [8, 9, 14]. Dysphagia is a frequent sequela from CNS tumors, especially those localized in the brainstem region [13]. In this study, most individuals who developed dysphagia had CNS tumors. Incidence of dysphagia was observed in 18.9% of the patients with CNS tumors. Gonçalves et al. analyzed 190 individuals with neurological tumors and observed dysphagia in 17% of the cases [13]. Mei and Morgan detected occurrence of dysphagia in 33% of the patients investigated after surgery for posterior fossa tumor resection [8]. The study by Morgan et al. demonstrated a higher incidence, with 73% of the participants presenting with dysphagia following postoperative tumor site resection [11].
In this survey, four new cases of dysphagia were observed in patients with HN tumors, corresponding to 18.2% of the individuals with tumors in this region. Functional impairments in patients with tumors in the HN region are associated with the involvement of the structures of swallowing dynamics compromised by the tumor, determined by site of the lesion and its extent. In addition, dysphagia may occur as result of the treatments performed [15].
Pediatric patients with tumors in the HN region frequently present with swallowing impairment resulting from structural changes caused by surgery or associated with the side effects of radiotherapy and chemotherapy [3, 28]. Dysphagia, odynophagia, trismus, mucositis, xerostomia, and changes in taste and appetite are common in patients undergoing these types of treatment [15, 28, 29]. A study conducted by Sahai et al. with 41 patients with nasopharyngeal carcinoma treated with radiochemotherapy (RT/CT) demonstrated that 47% of them developed dysphagia as a consequence of the treatment effects [29]. In research conducted with children and adolescents with rhabdomyosarcoma, individuals with tumors in the HN region presented a higher risk of development of mastication and deglutition problems than those with lesions in other regions [16].
New cases of facial paralysis and tongue paralysis have also been detected in children and adolescents with tumors in the CNS and in the HN region. Facial paralysis can be observed in patients with rhabdomyosarcoma in the HN region [16, 34, 35]. Rhabdomyosarcoma is the most common type of soft tissue sarcoma in children, and the most frequent primary site for occurrence of this tumor in childhood is the HN region [36]. Durve et al. reported the incidence of 64% of facial paralysis in a sample with pediatric rhabdomyosarcoma of the ear and temporal bone [17].
These functional disorders may also occur in patients with tumors in the brainstem and cerebellopontine angle, possibly because of cranial nerve involvement [30, 31, 32, 33]. Morris et al. who investigated a group of patients with infratentorial ependymoma, reported facial paralysis as one of the most frequent neurological deficits, affecting 50% of the sample [10].
Dysacusis was observed in 13 (40.6%) of the patients who underwent auditory monitoring for one year and in 40% of those who received chemotherapy with administration of an ototoxic drug (cisplatin). Cisplatin is an antineoplastic agent widely used in the treatment of different neoplasms affecting children and adolescents, such as medulloblastoma, nasopharyngeal carcinoma, osteosarcoma, hepatoblastoma and germ cell tumors [4, 6, 37]. The reported incidence of cisplatin ototoxicity ranges from 26 to over 90%, and this variation is influenced by treatment and patient-related factors [4]. Knight, Kraemer and Neuwelt reported an incidence of 61% decreased auditory acuity in the children evaluated, secondary to ototoxicity [4]. In research conducted with a Brazilian population of children and adolescents with cancer, Da Silva et al. reported dysacusis prevalence of 42% according to the American Speech-Language-Hearing Association (ASHA) criteria, corroborating the findings of this study [5]. The fact that not all patients underwent auditory monitoring during the follow-up period hampered the investigation on the incidence of hearing loss, which is considered a limitation to the present study.
Incidence of dysphagia and dysarthria was higher in the “Other regimens” treatment group, which included patients who received exclusive radiotherapy and RT/CT. Most of the individuals who developed dysphagia and dysarthria in this group corresponded to patients with brainstem tumors who were treated exclusively with radiotherapy, which is the treatment of choice for diffuse brainstem tumors [30]. The prognosis of these patients is poor and speech and swallowing disorders can commonly occur as the disease progresses, considering that the brainstem structures play an important role in the performance of these functions [30, 32].
Regarding dysphonia, case distribution was similar among patients with tumors in different sites, and no statistical difference was found between them, which may be associated with the small number of cases. Although dysphonia is a disorder observed in populations of healthy children and adolescents often related to vocal abuse [38], individuals with tumors in the CNS and in the HN region are at risk of development of vocal disorders in cases of involvement of the vagus nerve [13, 15].
The occurrence of new SLP disorders demonstrated statistically significant association with the site of the lesion. Onset of new SLP disorders during follow-up was greater in the groups with CNS and HN tumors. Individuals with tumors in the CNS are 8.29 times more likely to have new SLP disorders compared with patients with tumors in other sites, whereas those with tumors in the HN region present a 10.36-fold risk. These results can be explained by the important role that the structures of these regions play in the control and execution of communication, swallowing, and orofacial motricity functions.
Modern treatments for CNS and HN tumors often include both surgery and RT/CT. Many patients have been cured using these multimodal approaches, but they are also exposed to increased risk of disease- and treatment-related morbidities [10, 16, 18, 34, 35], which include functional sequelae as described in this study. In research conducted with survivors of pediatric neurological tumors, Armstrong et al. reported an increased risk of the development of endocrine, neurological, and sensory impairments in this population [18]. Although children and adolescents with tumors in the CNS and HN region are at an increased risk of developing disease- and treatment-related SLP disorders, other groups of pediatric oncology patients may also require SLP evaluation and intervention.
A limitation to this study may be the fact that only the disorders that were present at the time of the three assessments performed during the study were detected, which may have prevented the detection of any impairment begun and improved in between assessments. The sample size of this heterogeneous group of individuals may also be considered a limitation of the study. Studies with larger sample sizes, more frequent assessments, and longer follow-up periods could reveal more information about this population and the correlation between sociodemographic data and clinical characteristics with the development of the functional disorders evaluated. Nevertheless, the present study stands out for pioneering the investigations conducted, and it presents the profile of a relevant number of children and adolescents with cancer and benign neoplasms under treatment assisted at a single cancer treatment referral center.
Conclusion
In this study, an incidence of 22.8% for communication, swallowing, and orofacial myofunctional disorders was observed in a sample of patients with malignant and benign pediatric tumors monitored at a cancer institute for one year after hospital admission. Development of these disorders was greater in individuals with lesions localized in the central nervous system and in the head and neck region.
Footnotes
Conflict of interest
The authors have no conflict of interest to report.