
Abstract
PURPOSE:
Regardless of age or disease stage, children with neuromuscular disorders (NMD) are at risk of developing dysphagia and/or dysarthria. It is important to screen these children regularly in order to detect and treat problems as soon as possible. To date, there are no standardized tools for screening for dysphagia and dysarthria in children with NMD (pNMD). Thus, children are not always referred for assessment by a speech language therapist (SLT). A new screening instrument for dysphagia and dysarthria has been developed, the Screeninglist Physician of the Diagnostic list for Dysphagia and Dysarthria in pediatric NMD (DDD-pNMD). The diagnostic accuracy was estimated in this study.
METHODS:
Sensitivity and specificity were assessed in 131 children aged 2.0–18.0 years by comparing the outcome of the Screeninglist Physician with the diagnosis of dysphagia and/or dysarthria established by an SLT.
RESULTS:
The sensitivity of the Screeninglist Physician was 88% and its specificity was 63%. The AUC was 0.83. The prevalence of dysphagia and/or dysarthria was 53%.
CONCLUSION
: The Screeninglist Physician of the DDD-pNMD is the first valid screening tool for physicians to identify children with NMD with possible dysphagia and/or dysarthria, thereby enabling timely referral to an SLT.
Introduction
Neuromuscular disorders (NMDs) are a broad group of hereditary or acquired muscle disorders of variable severity. There are about 600 different muscle diseases which are often classified based on their anatomical origin: in the ventral horn of the spinal cord, the peripheral nerves, the neuromuscular junction, or the muscle fibers. There are congenital, stationary and slowly or rapidly progressive forms of NMDs [1]. Modern diagnostic procedures and improved medical management and rehabilitation therapy have increased the life expectancy of children with NMD [2]. However, swallowing and speech difficulties remain common problems in these individuals [3].
Normal swallowing includes oral, pharyngeal and esophageal phases [4]. Problems in one or more of these phases are called dysphagia, which may occur in all pediatric NMD (pNMD) [3] and are usually caused by weakness of the orofacial, pharyngeal, and thoracic muscles [5]. Its presence and severity largely depend on the muscle disease concerned [3, 6]. Children with NMD can have problems with chewing and need to swallow frequently in order to achieve complete emptying of the oral cavity and pharyngeal area, often resulting in long mealtimes [2, 5, 9]. These problems are caused by a decreased bite force and weakness of the masticatory muscles. Limited jaw opening affects chewing and oral hygiene [7], and many children retain food in the pharynx after swallowing [8]. The consequences of dysphagia can be substantial: failure to thrive, malnutrition, choking, recurrent respiratory infections, and aspiration pneumonia [10, 11, 12].
Children with NMD may also experience speech problems. In speech, many orofacial and thoracic muscles are involved, all contributing to strength, speed, range, steadiness, tone, or accuracy of movements necessary for intelligible and natural speech. Motor speech disorders called dysarthria are caused by disease of the peripheral and/or central nervous system which can affect various aspects of speech such as respiration, phonation, articulation, nasal resonance, and/or prosody [13, 14]. The type of dysarthria depends on the location of the injury in the nervous system [15]. Common features of dysarthria in pNMD include weak articulation, hypernasality, weak phonation, flattened prosody, and reduced speech volume [16, 17, 18, 19, 20].
Dysphagia often causes malnutrition, choking, or aspiration pneumonia [6, 21] and dysarthria influences intelligibility [22]; both hamper a child’s ability to participate. For this reason, it is important to monitor dysphagia and dysarthria throughout development. In the Netherlands, all children diagnosed with pNMD are regularly assessed by a multidisciplinary rehabilitation team under the direction of a rehabilitation physician or child neurologist. However, a speech language therapist (SLT) is not always part of this team in rehabilitation centers or hospitals. Therefore, possibly not all children are annually assessed by an SLT. Physicians are responsible for indicating whether referral to an SLT is necessary. For this reason, a validated, standardized tool for screening of dysphagia and dysarthria in pNMD that can be used by the physician was needed to create a better opportunity for referral [21, 23]. There is a wide range of problems due to muscle weakness that can occur in pNMD in which symptoms of dysphagia and dysarthria can be difficult to spot by physicians. Therefore, a Dutch working group of experienced SLTs involved in the care of children with NMD developed the Screeninglist Physician as part of a larger diagnostic instrument, the Diagnostic list of Dysphagia and Dysarthria in NMD (DDD-NMD) [24]. The intended use of the list was to screen for signs of dysphagia and dysarthria. If a child fails the screening, referral to an SLT for an extensive assessment should follow.
The aim of this study was to estimate the diagnostic accuracy of the Screeninglist Physician of the DDD-NMD compared with a clinical reference standard (SLT assessment and diagnosis) in children aged 2–18 years with an NMD. For this purpose, sensitivity, specificity, predictive values, area under the ROC-curve and the cut-off point were measured.
Method
A cross-sectional prospective study was carried out involving 131 children (aged 2.0–18.0 years) with an NMD who visited the pediatric multidisciplinary outpatient clinic of the Muscle Center of the Radboud University Medical Centre in Nijmegen or Rehabilitation Centre Klimmendaal in Arnhem (both in The Netherlands) between May 2015 and October 2016. SLT’s are a standard part of the multidisciplinary pNMD-teams of both centers. All consecutively admitted patients were eligible for inclusion if: (i) they had been diagnosed with an NMD; and (ii) were between 2;0 and 18;0 years of age.
Screeninglist Physician of the DDD-pNMD
The Screeninglist Physician is a short and quick screening, consisting of nine broad yes/no-questions (to be answered by parents/caregivers or by the young adult patient) (see Fig. 1): seven questions on feeding and swallowing and two questions on speech and communication. The broadly formulated questions are related to frequently reported complaints in pNMD [3].
Questions of the Screeninglist Physician (DDD-pNMD) (translated from Dutch).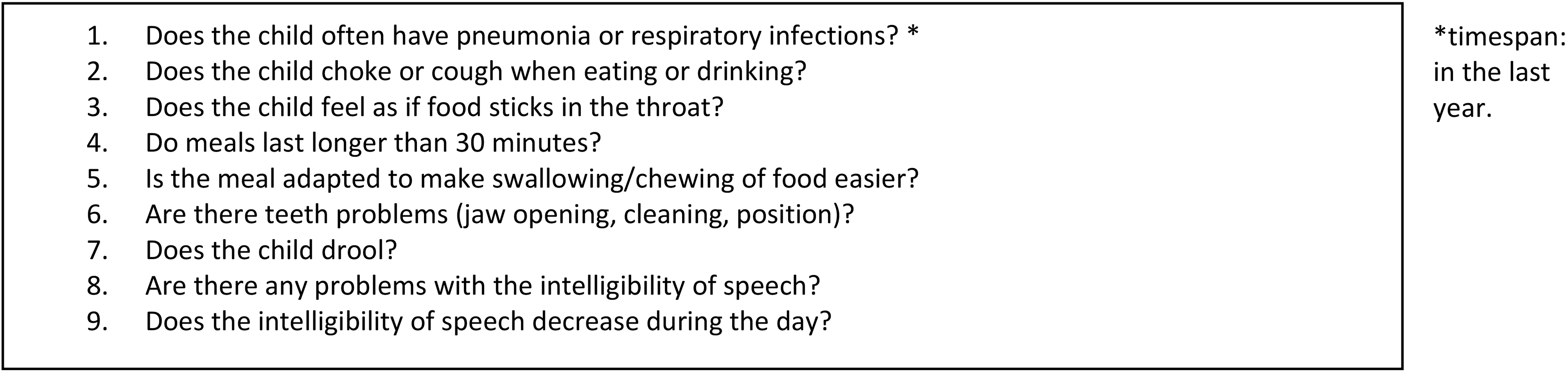
The physician administered the Screeninglist Physician together with caregivers or with young adults when visiting the outpatient clinic. The test positive cut-off was set at
All children, regardless of the outcome on the Screeninglist Physician, were seen by the SLT for a full assessment. The SLT’s were blinded for the outcome of the Screeninglist Physician. Diagnosis of dysphagia and/or dysarthria by the SLT was used as reference standard. This diagnosis was based on the SLT’s clinical evaluation, following national and international guidelines [25, 26]. To structure the clinical evaluation, the standardized diagnostic part of the DDD-pNMD was completed by an SLT for all children as best practice in the absence of other validated diagnostic tools [21]. The diagnostic part of the DDD-pNMD consists of an extensive speech language assessment covering case history and items of the themes: posture, oral and facial anatomy, oral structure and oral motor skills, saliva control, eating, drinking, chewing, swallowing, intelligibility of speech, and communication. All separate items within these themes are scored on a 4-point Likert scale based on the Radboud Dysarthria Assessment, ranging from 0 to 3 corresponding with no, mild, clear or severe abnormality [27]. A qualitative judgement has to be given in case the score was
Demographics and clinical characteristics of the participants (
131)
Demographics and clinical characteristics of the participants (
Data were collected from the Screeninglist Physician (positive/negative) and from the conclusion of the SLT assessment (dysarthria: yes/no, dysphagia: yes/no). In total, four physicians and four SLTs (Radboud University Medical Center and Rehabilitation Centre Klimmendaal) were involved in the study. All had more than 5 years clinical experience of NMD in children.
Where appropriate, the standards for reporting diagnostic accuracy studies (STARD) were followed. STARD is an internationally acknowleged guideline developed to help improve the transparency and completeness of the reporting of diagnostic accuracy studies [28]. This study was approved by the Committee on Research Involving Human Subjects of Arnhem and Nijmegen (no 2015–1690). Informed consent was obtained from the parents and children, or only from the parents for children younger than 12 years.
Cross tabulation of the indextest results (Screeninglist Physician) by the results of the reference standard (SLT assessment)
a
Descriptive statistics were used to document the general characteristics of the children. Diagnostic test accuracy was defined by sensitivity, specificity, and predictive values with 95% confidence intervals (CIs). Sensitivity, specificity and positive predictable value have been calculated for 3 age groups. A receiver operating characteristic curve (ROC) was used to calculate the area under the ROC. We used the theoretical a priori cut-off score of
Results
In total, 137 Dutch children with NMD participated in the study. After the exclusion of non-eligible children, the data of 131 children were analyzed (Table 1, Fig. 2). The SLT assessment was performed within 1 week of the Screeninglist Physician test.
Flow diagram: flow of participants.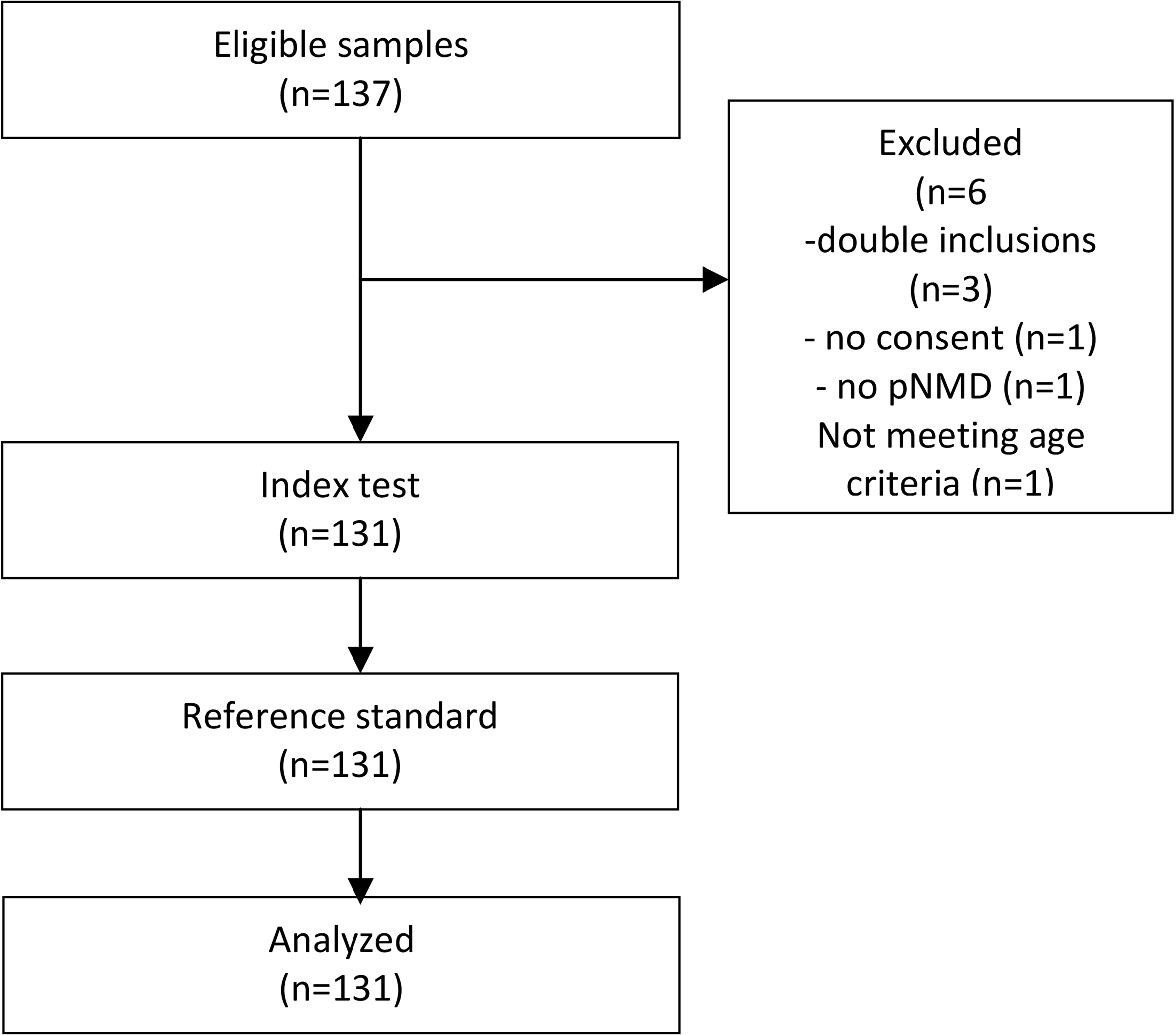
With a theoretical cut-off score of
Crosstabulation of dysphagia and dysarthria diagnosis by the SLT
Sensitivity, specificity and the percentage unnecessarily referred children (1-PPV) in the total group and 3 age groups
Receiver operating characteristic (ROC) curve and area under curve (AUC) for the Screeninglist Physician versus diagnosis by a speech language therapist (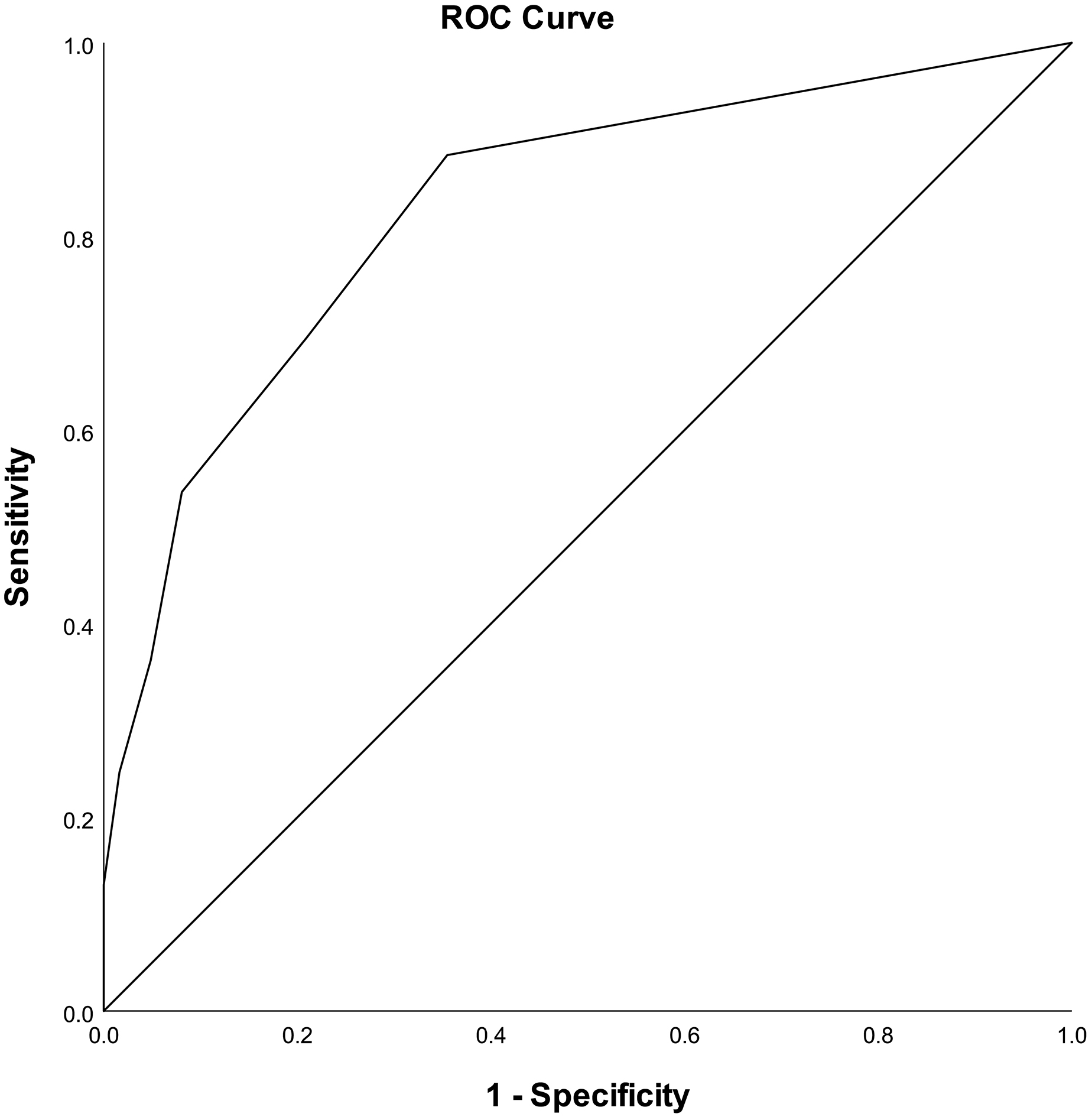
The Screeninglist Physician of the DDD-pNMD is a short and simple screeninglist for dysphagia and dysarthria and was developed by a group of experienced SLTs in the field of pNMD.
Based on the available literature, this is the first screening that is evaluated for diagnostic accuracy for this patient population. Our findings show that the Screeninglist Physician, with an AUC of 0.83 (95% CI 0.76–0.90), has a very good diagnostic accuracy [29], indicating a very good ability to distinguish between children with or without signs of dysphagia and/or dysarthria, diagnosed by an SLT. The physicians found the list clear and easy to use.
The desired sensitivity and specificity characteristics of a screening instrument depend on the purpose of screening. For the Screeninglist Physician, we aimed to focus on a high sensitivity (
Due to the sensitive and the less specific nature of the screening, children might be referred unnecessarily. Comparing 3 age groups (
The items on the Screeninglist Physician are covering a broad spectrum of symptoms of dysphagia. The cut-off score of
Screening is important for multiple reasons. First, the prevalence of dysphagia and dysarthria is high in children with NMD. For example, in children with SMA II and III it is 44.4% [6], and in children with myotonic dystrophy it is 51.9% [5]. In our study population, the prevalence of dysphagia and dysarthria was 53%. Second, dysphagia can have severe, sometimes life-threatening consequences [21], such as malnutrition, choking, and aspiration pneumonia. Dysarthria might hamper the function and participation of affected children and therefore adversely affect their quality of life. The high prevalence, in combination with the variable onset and consequences of dysphagia and dysarthria, justifies periodic monitoring of these children which would be greatly facilitated by using a short and easy to use screening instrument such as the Screeninglist Physician.
Due to measurements of diagnostic accuracy being sensitive to the design of the study, the STARD checklist was followed to optimize the design and reporting. Nevertheless, there are some limitations that must be taken into consideration.
First is that we had to rely on a best practice reference assessment and diagnosis by experienced SLTs in the absence of a comprehensive proven, valid and reliable instrument for the diagnosis of dysphagia and dysarthria in pNMD [21, 23]. Instrumental assessment such as a videofluoroscopic swallowing study (VFSS) is considered as the gold standard for detection of pharyngeal dysphagia. However, chewing problems or prolonged mealtimes are commonly reported complaints of dysphagia in pNMD [3] causing failure on the Screeninglist Physician. Children showing chewing problems are not referred for instrumental assessment, because these oral phase problems are not captured by VFSS. Second, a VFSS gives a small window of swallowing ability in which the common factor like fatigue is not included. Children with pNMD often cannot maintain ‘best swallow’ during the entire mealtime [21]. To establish a diagnosis of dysphagia and dysarthria, a broader assessment is needed. This is the reason why the SLT assessment was chosen as the best available (best reference standard) method for establishing the presence or absence of dysphagia or dysarthria.
If there were concerns about safe swallowing, or the feeling of food sticking in the throat, children were always referred for instrumental assessment as part of the assessment and intervention plan.
Second, test-retest reliability was not measured because the bias caused by awareness of the parents and possible progression of the disease could influence the results.
Conclusion
The Screeninglist Physician of the DDD-pNMD is the first valid tool to screen children and young adults with NMD for possible dysphagia and/or dysarthria, thereby enabling timely referral to an SLT.
Footnotes
Conflict of interest
The authors have no conflict of interest to report.