
Abstract
BACKGROUND:
Although considered an advanced area of practice, there has been insufficient standardization in clinical training and preparedness for occupational therapists (OTs), physical therapists (PTs), and speech-language pathologists (SLPs) practicing in the neonatal intensive care unit (NICU). The first step in developing a neonatal therapy certification process was to conduct a practice analysis.
PURPOSE:
To describe: 1) the collection of OTs, PTs, and SLPs working in NICUs, 2) educational and professional preparation to practice in the NICU, and 3) interest in neonatal therapy national certification.
METHODS:
An online survey of 468 neonatal therapists was completed in 2015–2016.
RESULTS:
There were 208 (47%) participants who were OTs, 140 (32%) PTs, and 94 (21%) SLPs. Among respondents, 187 (50%) neonatal therapists had a clinical doctorate, and 143 (40%) therapists practiced for
CONCLUSIONS:
Advanced training and skills of neonatal therapists are vital to ensure safe, effective and evidence-based practice. Insufficient standardization in training and variable adherence to education and training guidelines provided credibility for the creation of a neonatal therapy national certification process, which has now been implemented.
Keywords
Introduction
Although general knowledge related to a therapy discipline is validated at entry into each field, the American Occupational Therapy Association (AOTA), the American Physical Therapy Association (APTA), and the American Speech-Language-Hearing Association (ASHA) all recognize neonatal therapy as an advanced area of practice, requiring additional highly specialized training and skills [1, 2, 3, 4]. Despite established practice guidelines by the governing bodies [1, 2, 3, 4], there is insufficient standardization in clinical training and preparedness for therapy professionals practicing in the neonatal intensive care unit (NICU). Post-professional certification standards can ensure that therapists working with medically fragile infants in the NICU have met minimum benchmarks for safe, effective and evidence-based practice [5].
In 2014 the National Association of Neonatal Therapists (NANT) established an independent group, the Neonatal Therapy National Certification Board (NTNCB), to oversee the creation of a certification process for occupational therapists (OTs), physical therapists (PTs), and speech-language pathologists (SLPs) who practice in the NICU [6]. A neonatal therapy certification process, with the use of a portfolio review and credentialing examination, can ensure that therapists who practice in the NICU have the requisite experience and knowledge outlined as best practice by national governing bodies.
In order to ensure that practitioners have met certain standards for neonatal therapy certification, the methods of assessment must represent the current scope of neonatal therapy practice [7]. In 2013, Sturdivant published survey results of 226 neonatal therapists in and outside of the United States, working in hospitals with different sized NICUs (
To our knowledge, at the time, there had not been a comprehensive study of neonatal therapy practice that included what daily tasks are conducted by neonatal therapists and what level of training and preparation they had in order to work in the NICU. Conducting a practice analysis of OTs, PTs, and SLPs who work in the NICU was an important step toward the development of neonatal therapy certification. This study aimed to identify: 1) the number of neonatal therapists, 2) the practice settings and breadth of services provided by neonatal therapists, 3) the level of clinical training and preparedness for therapists working in the advanced practice setting of the NICU and how neonatal therapists are gaining this preparation, and 4) if there is a need for a certification process for neonatal therapists.
This research was the first step in defining the current scope of neonatal therapy practice, in order to lay the foundation for the development of a comprehensive and valid certification process, which has now been implemented.
Methods
Study population
The study was approved by two Institutional Review Boards, at Washington University and Sage Colleges, and voluntary consent was obtained with participants’ initiation of the survey. There were 468 OTs, PTs, and SLPs who previously had practiced or were practicing on a full-time, part-time, or consultative basis in a Level II, III, or IV NICU who participated in the survey. Invitations to participate in the web-based survey, hosted on SurveyMonkey
Distribution of surveyed NICU therapists in the United States.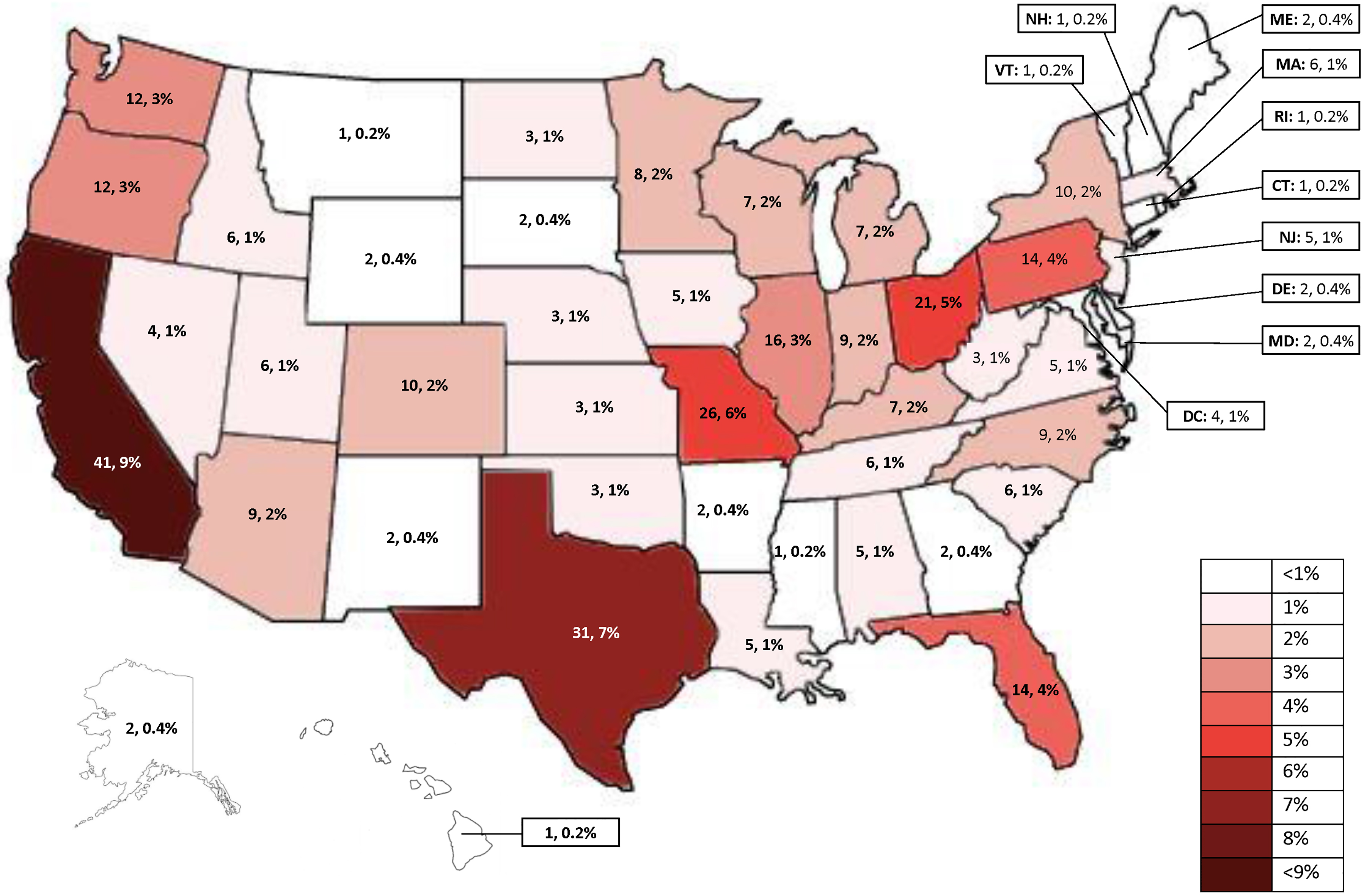
The 104-question mixed methods survey, which included open and closed-ended questions, was designed by the authors for this study. Some questions were adapted, with permission, from the survey previously conducted [8]. The current survey was pilot tested with 12 members of the NTNCB, and revisions were made based on participants’ feedback. Respondents were not required to answer all survey questions, and all questions that were answered were included in the analyses, even when there were missing answers to other questions. This resulted in the number of respondents for each question varying. The survey was open from October 2015 through January 2016. The broad scope of the 104 questions presented in the survey provided extensive data that were beyond the aims of this study. The full set of questions were coded to determine relevance to the research questions, and those not relevant to this study were removed from further evaluation.
Data analysis
Descriptive statistics were used to analyze survey responses. SPSS (IBM Statistics 24, Armonk, NY, USA) was used to calculate frequencies and proportions for discrete variables, as well as means and ranges of continuous and categorical variables. The ratio of NICU beds per full time equivalent (FTE) therapist was obtained by taking the response about the total number of NICU beds and dividing it by the number of full-time NICU therapists on staff.
Results
Four hundred and sixty-eight neonatal therapists participated in the survey. Respondents were not required to answer each question, so the number of respondents for each question varied. The neonatal therapists who participated in the survey represented 266 hospitals across all 50 states in the United States, in addition to 10 countries outside the United States. Figure 1 provides the specific distribution of therapists who responded to the survey in the United States.
Characteristics of NICU therapists participating in the survey
Characteristics of NICU therapists participating in the survey
Characteristics of the hospitals that survey respondents worked for
Of the therapists who completed the survey and answered the question about their discipline, 208 were OTs (47%), 140 were PTs (32%), 94 were SLPs (21%), and 26 did not identify their discipline. Table 1 contains characteristics of the neonatal therapists who took the survey, and Table 2 provides the characteristics of the hospitals where the therapists worked. Most notably, the largest proportion of therapists reported dedicating all of their time to the NICU rather than consulting, and they provided a variety of services such as parent and nursing education, engaging in discharge planning, and making referrals.
Clinical and educational preparation for practicing in NICU
Interest in neonatal therapy certification
Table 3 displays the clinical and educational preparation neonatal therapists received prior to practicing in the NICU, while Table 4 provides information on the level of interest in a neonatal therapy certification process. Respondents reported receiving NICU-related continuing education after receiving their therapy degree, and 299 (88%) believed it is highly important to have oversight/accountability for meeting standards while practicing in the NICU. There were 329 (98%) therapists interested (either highly interested, interested, or somewhat interested) in a neonatal therapy certification program.
The key findings of this study were: 1) there was a pool of at least 468 neonatal therapists, 2) neonatal therapists had a solid foundation of clinical practice, often rooted in pediatrics, and received education related to neonatal therapy in a variety of different ways after receiving their therapy degree, 3) most neonatal therapists indicated that oversight was highly important for therapists to practice in the NICU, and 4) most neonatal therapists indicated there was a need for and that they were very interested in a neonatal therapy certification program.
In 2016 there were at least 468 neonatal therapists currently practicing or who had previously practiced in the NICU despite there being no standardization of knowledge or skills available. AOTA, APTA, and ASHA all recognize neonatal therapy as an advanced practice area [1, 2, 3, 4], requiring advanced skills and training, however, no process to ensure a benchmark for advanced skills and training existed at the time. This highlighted the need for a process of neonatal therapy certification, which has since been implemented.
While most therapists entered the field with a Bachelor’s degree, one-half of neonatal therapists had achieved clinical doctorate degrees, and an additional 14% had achieved a PhD or similar terminal degree. Given that neonatal therapy is considered an area of advanced practice, therapists working or planning to work in the NICU require further education and training, outside traditional education and training programs, in order to provide the best care for this vulnerable population. Most therapists reported that they received only one lecture related to the NICU in their therapy program, which introduces the topic, but does not enable in-depth understanding of key concepts related to the NICU that allows practice in this specialty area. NICU-related continuing education coursework was an important part of preparation for advanced practice in the NICU. Therapists reported obtaining education on NICU practice by attending specialized courses or conferences, hospital in-services, and watching online webinars. On-the-job training and mentoring appeared to be another important element of becoming a neonatal therapist. Most of those who were surveyed had been practicing for
Neonatal therapy centers around the developmental needs of newborn infants who are receiving intensive care interventions. It is different from other areas of pediatric practice in that it requires the careful integration of knowledge about vulnerability, medical factors and interventions, mother-baby care and interaction, and the complex NICU environment in order to optimize outcomes during a critical period of development. The proportion of time spent in the NICU, compared to other areas of practice, and the types of therapeutic modalities used in NICU practice varied across settings. The largest proportion of neonatal therapists reported dedicating all their working hours to the NICU, but some only performed consultative services in the NICU. For those who provided only consultation in the NICU, their caseloads largely consisted of adults, which can make it challenging to have enough time to develop the specialized skills needed for independent practice in the NICU. This also requires therapists to demonstrate competence across two very different practice areas, which may impact quality of patient caregiving in one or both areas. Neonatal therapists reported a wide range of therapeutic modalities used in the NICU, and most described engaging parents in the NICU and educating them for care after discharge. Neonatal therapists work in different types of NICUs, within and outside of teaching hospitals and/or free-standing children’s hospitals. Most stated that there was at least one therapist in their NICU for every 1–20 beds. Most neonatal therapists also reported that 71–100% of infants in the NICU receive therapy services.
Due to the relatively large number of therapists currently in practice and entering practice in the NICU, and the advanced and complex nature of the NICU setting, it is important that there be a process of validation to ensure adequate education, training, and knowledge for working independently with high-risk infants in the NICU. Most therapists reported that oversight, as in validation of experience and knowledge, is highly important for ensuring safety and evidence-based therapy in the NICU setting. Many hospital systems may have clinical competencies to ensure those entering the NICU have achieved advanced skills. However, there can be significant variability across settings in how clinical competencies are implemented, and to ensure up-to-date, evidence-based practice, these would need to be updated regularly. A certification program can ensure that all neonatal therapists are held to the same, current, and evidence-based standard of validation, providing a consistent framework to achieve oversight. In addition, the American Academy of Pediatrics published a guideline that recommends that a PT or OT with neonatal expertise, as well as someone with expertise in neonatal feeding and swallowing, be on staff in Level III and IV NICUs [12]. Neonatal therapy certification provides a process of validation as a subspecialty area of therapy practice. Ninety-eight percent of survey respondents indicated they were interested in neonatal therapy certification.
Since this survey, an international process of neonatal therapy certification was implemented in 2016–2017. The requirements for certification include a minimum of 3 years as a credentialed professional (OT, PT, or SLP), 3500 hours of experience in the NICU, 40 hours of education about NICU-specific content within the last 3 years, 40 hours of mentored experiences, and a passing score on the Neonatal Therapy National Certification Examination [13]. The 3 years of clinical practice and the 3500 hours of experience in the NICU that is required for neonatal therapy certification is consistent with other advanced certification programs, such as hand therapy, which requires a minimum of 3 years of practice and 4000 hours in hand therapy. Mentoring and current education is also important if a therapist intends to work in the NICU. Therefore, the requirement for neonatal therapy certification also includes 40 hours of education within the previous 3 years and 40 hours of mentoring. Passing an exam is an indication of adequate knowledge in an area of practice. In addition, the use of an exam is consistent with other multidisciplinary certification programs, such as hand therapy. The neonatal therapy certification process can aid therapists who are interested in entering practice in the NICU by providing a roadmap to achieve the experience and knowledge needed to work independently in the NICU. The certification process can also be valuable to hospital administration, providing an avenue to validate that a therapist is able to provide therapy services in the high-risk setting of the NICU. After 2 years of implementing the neonatal therapy certification program, there are now over 300 Certified Neonatal Therapists worldwide.
Study limitations
This study was limited by the absence of a complete and comprehensive list of neonatal therapists to survey. Lists that were used reached other disciplines (nurses, hospital administration, and neonatologists) in addition to neonatal therapists. Therefore, the response rate could not be calculated. It is also unclear how many neonatal therapists could not be reached by the survey. Thus, while this survey aided our understanding of the minimum existing number of neonatal therapists and perceptions among them, there may be population bias in responses related to those who could be reached and those who responded. In addition, a much higher number of neonatal therapists likely exists, based on the presence of many NICUs in the United States alone. However, this is one of the first reports of its kind and paves the way for future studies. After data collection, the number of neonatal therapists per NICU bed was calculated to identify how many are typically employed based on NICU capacity. However, this estimate is limited since the number of beds does not necessarily reflect the average number of patients in each NICU. The number of patients cared for by each therapist was not collected. Finally, this was a study of therapists who are already practicing in the NICU setting. The perceptions of those who seek to enter the NICU setting were not represented. However, a certification process can aim to provide a pathway toward entry into the NICU, which could serve both current and prospective neonatal therapists.
Conclusions
Although therapists practicing in the NICU are expected to obtain additional NICU-related training and skills in this advanced area of practice, prior to 2016 there was no formal validation process to ensure those working in the NICU had adequate neonatal expertise for safe, evidence-based practice. This initial practice analysis identified a pool of at least 468 neonatal therapists with significant NICU-related education and experiences. The need for oversight was deemed highly important, and the interest in a national certification program was high. These findings were used to define the need for and requirements for neonatal therapy certification. Future practice analyses will aim to ensure the certification process is aligned with current NICU practice and to employ improved methodologies to reach all neonatal therapists. In addition, future practice analyses can determine if the examination adequately assesses necessary knowledge to function as a neonatal therapist.
Footnotes
Acknowledgments
We would like to thank Laura Renew, Sue Ludwig, Chrysty Sturdivant, Kati Knudsen, Elizabeth Jeanson, Kay Thurston, Jen Hofherr, Erika Lee, Mary Stanford, Johanna Siemon, Jennie Jacob, Lisa Kleinz, Margaret Miller, and Deanna Gibbs. In addition, we would like to thank the neonatal therapists who graciously gave their time to take the survey and help us better understand this practice area. Finally, we wish to thank the National Association of Neonatal Therapists for their dedication to improving the practice of neonatal therapy and for establishing an independent board to develop neonatal therapy national certification.
Conflict of interest
Three of the authors (RP, AF, and JC) are past or previous board members of the Neonatal Therapy National Certification Board (NTNCB), but they did not receive any payment for their work related to this manuscript. Their participation on the NTNCB is volunteer in nature, and fees generated from the certification process have no direct financial benefit to them. There are no conflicts of interest relevant to this article to disclose for the other authors. The authors have no financial conflicts of interest relevant to publication of the subject matter or materials in this manuscript. There was no funding that supported this project.