
Abstract
PURPOSE:
To identify factors associated with success of corrective bony hip surgery among patients with cerebral palsy (CP).
METHODS:
A retrospective review was conducted of medical records of patients diagnosed with CP and hip displacement who underwent surgery from 2004 to 2016 at the authors’ institution and who had a one-year minimum follow-up. Patient age, sex, Gross Motor Function Classification System (GMFCS) level, surgical procedure(s), type and extent of CP, presence of preoperative and postoperative hip pain, and hip migration percentages (MPs) were recorded. Surgical success was defined as a postoperative MP
RESULTS:
Thirty-eight patients (55 hips) met the inclusion criteria. Mean age at surgery was 10.2 years (range, 2–24 years). Mean MP (standard deviation) improved from 64
CONCLUSION:
In patients with CP and hip displacement, early preventative correction of hip displacement after age 5 may improve clinical outcomes, though future studies are needed to provide more definitive clinical direction.
Introduction
Progressive hip displacement is one of the most common orthopaedic problems in patients with cerebral palsy (CP), occurring in approximately one-third of all children with CP and in 90% of those with GMFCS level V [1]. Hip displacement can cause pain, limit function (including ambulation, sitting, and perineal care), and diminish quality of life [2]. The most frequently used measure of hip displacement is Reimer’s hip migration percentage (MP). Hips with a MP
Surgical approaches for treating hip subluxation or dislocation are classified as preventive, reconstructive, or salvage [4]. Preventative procedures involve soft tissue releases (e.g., adductor or hamstring release) and are typically used to prevent subluxation. However, once a hip begins to undergo subluxation, preventing further displacement via soft tissue releases becomes difficult [5]. Reconstructive hip surgery typically involves proximal femoral varus derotational osteotomy (VDRO) to correct coxa valga and femoral anteversion and/or pelvic osteotomy to correct acetabular deficiency. Salvage operations are limited and include femoral head resection, hip arthroplasty, or hip arthrodesis. In general, a MP greater than 40% is an indication for surgical intervention to prevent hip dislocation [6].
Though multiple factors likely influence surgical outcomes for patients with CP and hip displacement, the timing of corrective hip surgery in the context of the patient’s pain (i.e., proactively (before onset of pain) or reactively (after pain is reported)) is of increasing clinical interest. The relationship between hip morphology and pain in patients with CP is unclear and remains controversial [7]. Furthermore, pain is often difficult to assess in this patient population, especially among severely affected patients with communication impairments. In such cases, physicians rely on caregiver reports of the patient’s pain to help determine when to proceed with hip surgery. Corrective bony hip surgery is an invasive procedure that requires a long recovery period; thus, patients and their caregivers may choose to delay surgery as long as possible. Because physical therapists often work closely with patients with CP and can assess pain levels, elucidating how preoperative pain influences surgical outcomes may help to inform physical therapists about when to refer patients for surgical evaluation.
To the authors’ knowledge, no study has reported on the associations of preoperative hip pain and MP with surgical outcomes in patients with CP undergoing corrective bony hip surgery. The purpose of the study was to investigate how patient age, sex, GMFCS level, type of surgery, type and extent of CP involvement, preoperative hip pain, and MP correlate with surgical outcomes in this patient population. This inquiry is important because it may influence the timing of corrective hip surgery, about which there is presently no consensus.
Methods
Study population
After institutional review board approval at Johns Hopkins Medicine was obtained, medical records were reviewed for all 84 patients diagnosed with CP who underwent corrective bony hip surgery at the authors’ institution between 2004 and 2016. Forty-six patients were excluded because they had (a) less than one-year follow-up, (b) multiple/repeat bony hip surgeries, (c) femoral head resections, and/or (d) incomplete medical records (e.g., missing radiographic images). Thirty-eight patients (22 males and 16 females) who underwent 55 bony hip surgeries (17 bilateral and 21 unilateral procedures) met the inclusion criteria. For patients who underwent bilateral corrective hip surgeries, we included each hip as a unique case in our analysis, such that 55 total hips were analyzed. This was done to increase the power of statistical analysis. For each patient, a detailed medical record review was performed by two authors (EC and DJ), with discrepancies resolved by the senior author (CS). Patient, surgical, and radiographic data, as well as data on preoperative and postoperative hip pain, were collected (Table 1).
Demographics of 38 patients with CP who underwent corrective bony hip surgery at one institution, 2004–2016
Demographics of 38 patients with CP who underwent corrective bony hip surgery at one institution, 2004–2016
CP, cerebral palsy; MP, migration percentage; GMFCS, Gross Motor Function Classification System; VDRO, varus derotational osteotomy.
Patient age at time of surgery, sex, GMFCS level, type of CP, and extent of CP involvement were recorded. GMFCS level was determined according to the revised classification tool by Palisano et al. [8], which was established for use in children aged two to 18 years. Because this classification system represents a person’s gross motor function and limitations, it was applied to all patients (aged 2–24 years) in this study: twenty-seven patients were nonambulatory and were classified as GMFCS level IV (
The CP type was categorized as spastic for 27 patients, mixed for seven, athetoid for two, and undetermined for two. The extent of CP involvement was categorized as quadriplegic for 27 patients, diplegic for nine, hemiplegic for one, and undetermined for one.
Type of surgery (specific procedure, as well as bilateral or unilateral), previous soft tissue releases and/or botulinum toxin injections, and perioperative complications were recorded. Nearly all surgeries (37 of 38 patients) were performed by one surgeon, with the procedure type(s) determined by the surgeon. Procedure types varied extensively, with all patients undergoing some combination of femoral VDRO, pelvic osteotomy, and/or muscle releases/lengthening. Pelvic osteotomies included iliac, ischial, and pubic osteotomies with or without autologous bone graft, following Dega, Pemberton, or Chiari techniques.
Hip pain
Hip pain was recorded as present or absent both preoperatively and postoperatively on the basis of medical record review. Pain was documented in the medical records by the operating surgeons or other providers during the clinical encounters as indicated through multiple forms of assessment, including by directly asking the patient (depending on the patient’s ability to communicate), physically examining the patient, and asking the caregivers. Quantitative pain ratings such as the Face, Legs, Activity, Cry, and Consolability (FLACC) scale, numeric pain scale, and facial scale ratings were recorded inconsistently in the medical records, so a more detailed analysis of pain was not possible.
Hip migration percentage
Preoperative and postoperative pelvic radiographs were evaluated blindly by the first author, who used them to derive Reimer’s MPs [9]. Typically, hips with MPs
Data analysis
Results were analyzed using two-tailed Student
Results
Surgical success
For all hips, mean MP improved from 55
Summary of the associations between patient age, sex, GMFCS level, degree of CP involvement, preoperative pain, and properative MP and surgical success among 55 studied hips
Summary of the associations between patient age, sex, GMFCS level, degree of CP involvement, preoperative pain, and properative MP and surgical success among 55 studied hips
Fifteen of 23 female hips (65%) and 23 of 32 male hips (72%) met the criteria for surgical success (
GMFCS level
No significant correlations were identified between GMFCS level and surgical success. Fourteen of 16 hips (88%) from patients with GMFCS level II or III were associated with a successful surgical outcome, whereas 24 of 39 hips (62%) from those with GMFCS level IV or V were associated with a successful surgical outcome (
Type and extent of CP involvement
No significant correlations were found between type or extent of CP involvement and surgical success. Thirteen of 15 hips from patients with milder involvement (diplegia or hemiplegia) were associated with a successful surgical outcome, whereas 25 of 38 hips from patients with more extensive involvement (quadriplegia) were associated with a successful surgical outcome (
Surgery type and complications
No significant correlation was shown between any surgery type and surgical success, which may be explained by the wide range of surgical interventions and small population size. Perioperative complications were recorded for seven patients (two cases of wound dehiscence and five wound-related infections); these did not correlate with surgery type or surgical success.
Preoperative and postoperative MP
A lower preoperative MP was significantly associated with surgical success. The mean (
Preoperative hip pain
The absence of preoperative hip pain was significantly associated with surgical success. Six of 14 hips (43%) associated with preoperative pain met the criteria for surgical success, whereas 32 of 41 hips (78%) that were not associated with preoperative pain met the criteria for surgical success (
Discussion
The results of this study suggest that patient sex, type or extent of CP involvement, type of surgery, and perioperative complications are factors that are independent of surgical success, as defined herein, among patients with CP who undergo corrective bony hip surgery. In contrast, the absence of preoperative hip pain (
The findings indicating that the absence of preoperative hip pain and a milder preoperative MP were associated with successful surgical outcomes may have especially important clinical implications because both factors are commonly considered in the surgical evaluation of hip displacement in this patient population. Hip pain and MP may be interrelated, but any relationship between the two is only ostensible; in the present study, patients may have had a completely dislocated hip and been free of hip pain or have had very little hip displacement and been bothered by hip pain. Hip pain itself may be assessed by caregivers or providers outside the clinic and may inform the referral of patients for surgical evaluation. Further, because hip pain and MP may develop and/or worsen over time, these findings suggest that early preventative surgical correction of hip displacement to prevent the onset of hip pain and minimize the preoperative MP may optimize clinical outcomes, though additional studies are needed to support this. Representative anteroposterior radiographs showing successful and unsuccessful surgical outcomes in two patients with CP undergoing corrective bony hip surgery are shown in Fig. 1.
Anteroposterior radiographs showing successful (A, B) and unsuccessful (C, D) surgical outcomes in two patients with cerebral palsy (CP) undergoing corrective bony hip surgery. (A) Preoperative image of a 12-year-old boy with spastic quadriplegic CP, no preoperative hip pain, and a worsening 49% migration percentage (MP) of the left hip. (B) The same patient 1.5 years after surgical bony hip correction via varus derotational osteotomy and pelvic osteotomy, showing fully corrected MP with no postoperative hip pain (successful surgical outcome). (C) Preoperative image of a 13-year-old boy with spastic quadriplegic CP, preoperative hip pain, and a worsening 61% MP of the right hip. (D) The same patient 1.2 years after surgical bony hip correction via varus derotational osteotomy and pelvic osteotomy, showing fully corrected MP. The patient continued to have postoperative hip pain (unsuccessful surgical outcome). Among all hips investigated in the present study, the absence of preoperative hip pain was associated with surgical success, which was defined as the absence of postoperative hip pain and a postoperative MP 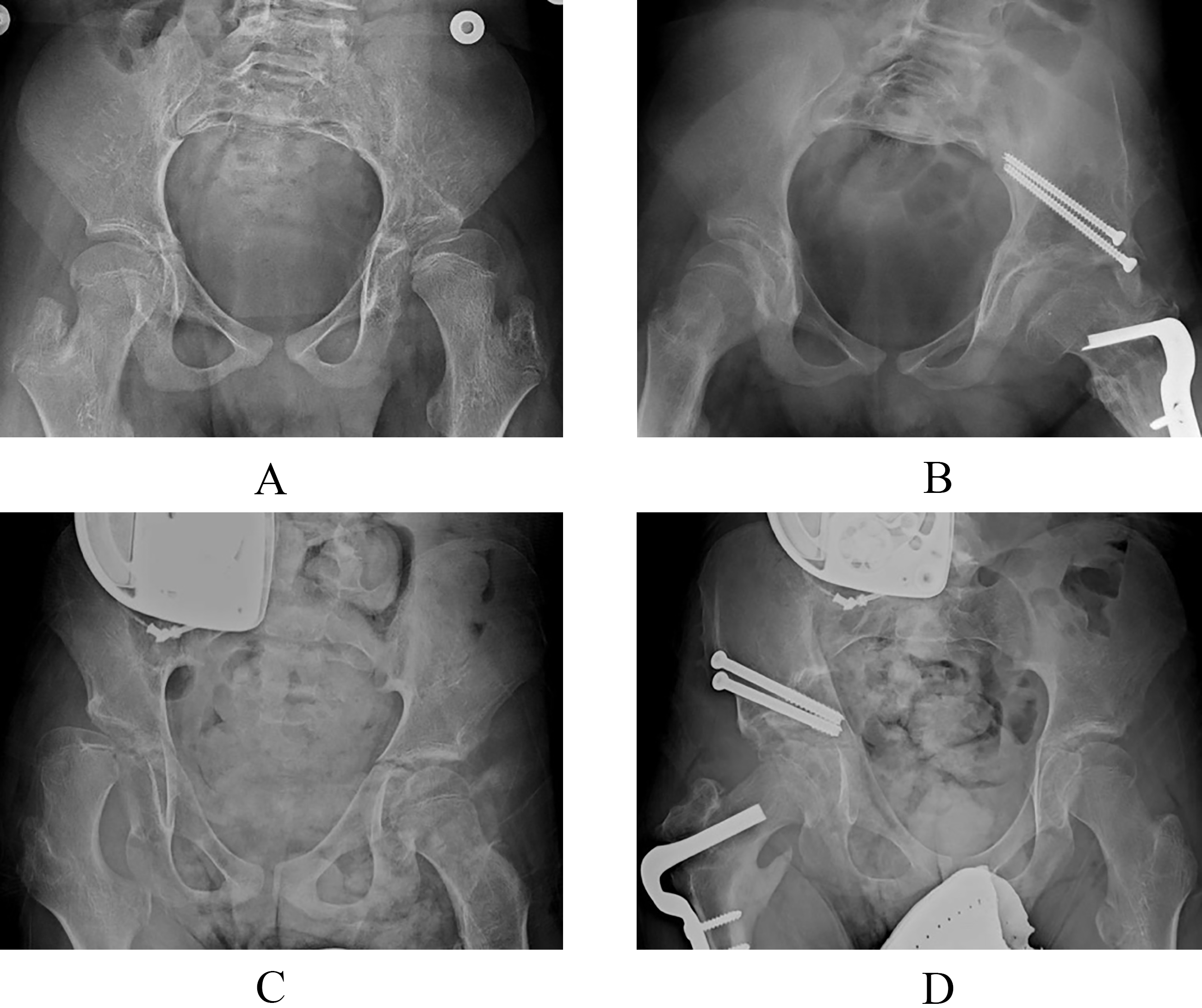
The current findings align well with the relevant literature to support previous conclusions and suggest future directions for research. In one of the few reports of patient sex and surgical outcomes in patients with CP, Zwick et al. [10] reported in 2012 that although both boys and girls with spastic, diplegic CP initially benefited from single-event multilevel surgery (bone and soft-tissue), boys eventually deteriorated in walking ability at 10 years of follow-up. Although most patients in the current study were quadriplegic, the study by Zwick et al. suggests that additional follow-up is needed to evaluate surgical success, as we have defined, for our patients in the long term. In addition, Lee et al. [11] reported in 2009 that parental satisfaction after single-event multilevel surgery in ambulatory children with CP was greater in parents of younger patients. Clinically, this finding may need to be balanced by our subgroup analysis that suggests that surgical intervention before age 6 is associated with lower rates of surgical success. Further, multiple other reports suggest avoiding surgical hip correction on very young children with CP [12, 13], including one by Schmale et al. [14] that reported a reoperation rate of 74% at 5-year mean follow-up in children with spastic CP who underwent bilateral VDRO before age 6 years. Additionally, multiple reports indicate that lower GMFCS levels are strong predictors of surgical success, defined quantitatively in terms of MP or the need for revision surgery [15, 16]. These findings support the current study’s subgroup analysis by GMFCS level, which suggests that GMFCS levels II and III were associated with higher rates of surgical success compared with GMFCS levels IV and V, though this finding was not found to be statistically significant (
This retrospective study has several limitations. Forty-six patients were excluded because they had less than one-year follow-up, multiple/repeat bony hip surgeries, femoral head resections, and/or incomplete medical records. It is unknown what effect this has on the findings. Further, the relatively small sample of 38 patients (55 hips) limited the power of statistical analyses, including the ability to account for correlations between one patient’s bilateral hips. Most importantly, the assessment of pain is a limitation of our study, as standardized pain ratings and scales were not used in the clinical notes. In addition, retrospective chart reviews are inherently limited in the availability and reliability of data. Nonetheless, the authors believe that the presence of hip pain, regardless of the rating, should be considered in the surgical evaluation of these patients. Further, as with similar studies involving patients with severe CP, accurately assessing hip pain in this patient population can be challenging and often relies on caregivers or other providers. We agree that prospectively collecting data and evaluating pain over time with a reliable and reproducible grading system would strengthen our study. We present our results to add to the literature on when to intervene surgically to correct hip displacement in patients with CP, a challenging topic for which there is currently no consensus. Additional potential confounders include the relationship between hip morphology and pain, which was not investigated; the surgical algorithms followed by the treating physicians; and the limited follow-up time, especially in skeletally immature patients. Although the authors believe that one-year follow-up is sufficient to gain insight into the correlations of interest in this study, these patients will continue to be followed so that longer-term follow-up may be reported in the future.
In patients with CP and hip displacement, early preventative surgical correction of hip displacement before the onset of bony hip pain and worsening MP may lead to improved clinical outcomes, though these findings must be considered cautiously in the context of this single-center retrospective study. The authors believe that pain and MP should be considered along with patient and caregiver preferences to promote successful surgical outcomes. Future studies with larger patient populations, standardized pain rating systems, and longer-term follow-up are needed to provide more definitive clinical direction.
Footnotes
Acknowledgments
The authors have no conflicts of interest to report. In addition, the authors wish to thank Jennifer Keller, PT, for her input and support, as well as two physical therapy students who assisted with data collection: Jessica Frank, SPT, and Lee-El Gakner, SPT.
Conflict of interest
None to report.