
Abstract
PURPOSE:
The PEDI-CAT measures daily functioning of children and youth, aged 1 to 21 years, with a variety of physical, cognitive and/or behavioral disabilities. In order to use an instrument in another culture or language, translation and cross-cultural validation are important, particularly for end-users. This study describes the process of translation and cross-cultural adaptation of the Dutch version of the PEDI-CAT.
METHODS:
End-users were involved in all steps. First, the PEDI-CAT items were reviewed to determine whether the items were relevant and acceptable in the Dutch culture. Then, the PEDI-CAT was translated into Dutch using specific guidelines. Finally, the wording of the Dutch items and response options were reviewed and tested with 22 parents of children and adolescents with and without disabilities.
RESULTS:
All 267 items and response options of the original PEDI-CAT were assessed as relevant and translated into Dutch. A selection of 175 items was tested with Think Aloud interviews which revealed that the translation of 46 items could be improved.
CONCLUSION:
The role of end-users in the process of translation and cross-cultural adaptation was crucial. This collaborative process resulted in a Dutch version of the PEDI-CAT that has been optimally adapted to the Dutch language and culture.
Keywords
Introduction
The PEDI-CAT (Pediatric Evaluation of Disability Inventory Computer Adaptive Test) [1] is a computerized measurement tool that assesses the daily functioning of children and youth (from 1 to 21 years of age) who have a variety of physical, cognitive and/or behavioral disabilities. It is based on a paper-pencil test, the Pediatric Evaluation of Disability Inventory (PEDI) [2], which has served as a functional outcome measure for clinical research and practice and has a long history of application in developmental medicine [3, 4, 5, 6]. The original PEDI is a fixed-format test in which all items need to be administered to derive a score, making the administration time-consuming and burdensome. Moreover, the tool was normed on children up to the age of 7.5 years, creating a ceiling effect when administered to older children and those with higher functional abilities [3, 7].
Steps in the translation and cross-cultural adaptation of the Dutch PEDI-CAT.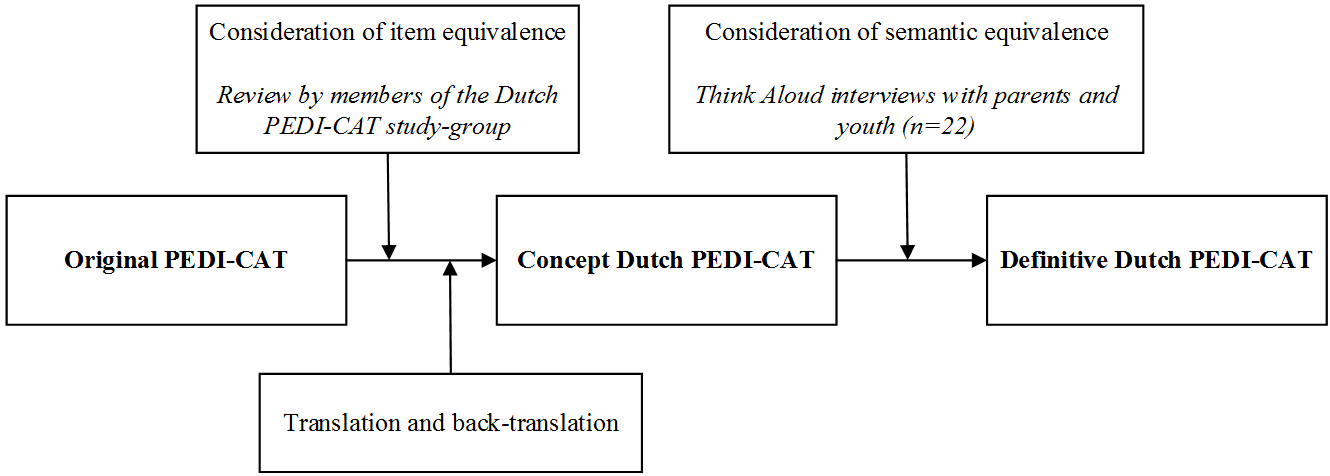
The PEDI-CAT however, utilizes Computer Adaptive Testing (CAT) methodology with new item banks covering a broader age range (from 1 to 21 years of age) [1, 7, 8, 9]. The PEDI-CAT software uses Item Response Theory (IRT) to create items and ratings on a continuum of functioning for each domain. An algorithm selects the next item based on the response to current one. In addition, it has filters for age, gender, use of walking devices, and wheelchairs [1]. Therefore, a child’s functioning can be assessed with a minimal number of items individualized for each child.
The content of the PEDI-CAT is based on the theoretical framework of the International Classification of Functioning, Disability and Health (ICF) [10] and its version for children and youth (ICF-CY) [11]. The PEDI-CAT consists of four domains. Three functional skill domains (Daily Activities, Mobility and Social/Cognitive) address the Activity dimension of the ICF, defined as the performance of discrete tasks. The fourth domain, Responsibility, examines an area of participation, i.e., engagement in life situations. This domain addresses the extent to which a child takes responsibility for life tasks that are important for independent living [1]. The assessment focuses on typical performance at the present time and can be completed by the child’s parent(s) or professionals who know the child well. The PEDI-CAT item pools were derived from the original PEDI and supplemented with items from existing performance-based and functional pediatric measures. Parents played an important role in the final selection of items for the PEDI-CAT by providing feedback about content coverage, content relevance, and item clarity [7].
The PEDI-CAT, which is validated and used in the United States [9] and Brazil [12], could be a valuable tool in pediatric rehabilitation practice and research in other countries. In order to be used in other cultures, the items must be translated accurately and adapted culturally to maintain the content validity of the instrument [13, 14]. Therefore, in order to use the original PEDI-CAT in another culture and/or language, translation and evaluation of cultural equivalence are important. The tool adaption process involves several steps [13]. Specific guidelines, including an important role for end-users, have been prescribed by the developers of the PEDI-CAT.
Overall there is growing consensus about the crucial role of end-user involvement (including patients, relatives and professionals) in research; initiatives and publications on this topic are rapidly increasing [15]. The recognition of the family as the expert, one of the core principles of the family-centered approach in pediatric health care [16, 17], is acknowledged more and more, not only in healthcare, but also in research [18, 19]. End-users play a crucial role in ensuring that the translation process yields a new version that is culturally appropriate, and that items are interpreted similarly in the original and comparison culture.
This study describes the Dutch translation and cross-cultural adaptation of the PEDI-CAT. It focuses on: item equivalence, translation and back-translation, and semantic equivalence with input from end-users.
The content, an example of an item and the scoring scale for each PEDI-CAT domain [1]
The original PEDI-CAT was translated into Dutch following the guidelines provided by PEDI-CAT authors based on generally accepted guidelines for cross-cultural adaptation of measures [13, 14]. The following steps were performed: a review of item equivalence, translation and back-translation, and semantic equivalence (Fig. 1). End-users (i.e. parents and professionals in pediatric rehabilitation) were involved in all steps. When reviewing item equivalence, the PEDI-CAT study-group played a central role. This group consisted of a representative of the parent organization BOSK (Association of Physically Disabled Persons), two pediatric rehabilitation physiatrists, two pediatric physical therapists, one occupational therapist, two human movement scientists, and one expert in research methodology. The representative of the parent organization BOSK was one of the two translators. A mother (native English) of a child with cerebral palsy was one of the two back-translators. Finally, parents and adolescents were involved in the evaluation of semantic equivalence.
This study was reviewed and approved by the Research Committee of the Center of Excellence for Rehabilitation Medicine Utrecht, and Ethical Committee of De Hoogstraat Rehabilitation, Utrecht, The Netherlands. Informed consent was obtained at inclusion.
Instrumentation
The PEDI-CAT measures the performance of activities in the child’s and adolescent’s daily environment, using an item bank of 276 items across four domains. Three domains concern the performance of daily functional skills: Daily Activities, Mobility and Social/Cognitive. These domains are scored on a one- to four-point Likert scale. The fourth domain, Responsibility, measures the extent to which a child takes responsibility for life tasks that are important in becoming an adult. This domain, which can be used for children starting at age 3, is scored on a one- to five-point Likert scale.
The PEDI-CAT does not have any special administration requirements other than the use of a computer to install the PEDI-CAT software. It can be completed independently by the child’s parent(s)/caregiver(s), or by a professional. Table 1 provides a short description of the content, example items, and the scoring of the domains.
Consideration of item equivalence
This step focused on a review of the original PEDI-CAT items to determine whether the items were relevant and acceptable in the target culture. The full set of items was presented to members of the Dutch PEDI-CAT study-group, including pediatric rehabilitation professionals from various disciplines, a representative from the parent organization BOSK, and scientists. They classified all items as “definitely relevant”, “maybe relevant” or “definitely not relevant”. The respondents were asked to explain exactly why they classified items as “maybe relevant” or “definitely not relevant”.
Then, the items were categorized into several grou-ps: (1) Items that could be translated “as is”; (2) items that required only minor modifications before translation (e.g. substituting a more culturally-appropriate example); (3) items that needed to be replaced because they were not culturally-accurate; and (4) items that would need to be eliminated because they were irrelevant. As items could be classified differently by different members of the study-group, a strict decision-rule was used to decide how to handle items in the translation process. For each item, the highest category (1 through 4) was used, e.g., if one member of the study group classified an item as category 3, and the others as category 1, it was decided to handle it as category 3 (item needs to be replaced because not culturally-accurate).
Demographic data of participants
Demographic data of participants
* with the help of a sign language interpreter.
Two translations were performed, one by a representative of the parent organization BOSK (JV) who is fluent in both English and Dutch, and one by an official translation agency. One draft version of the Dutch PEDI-CAT was made by combining these two independent translations. This version was translated back into English by two independent individuals, both native English speakers who have lived in The Netherlands over 20 years. One of the translators was a mother of a child with cerebral palsy. This version of the Dutch PEDI-CAT was called the concept version.
Consideration of semantic equivalence
Using cognitive interviewing techniques, the next step was to evaluate whether the translated items and response options were understood as intended for end-users of the PEDI-CAT.
Participants
Twenty-two participants were included. Criteria for inclusion for parents were: (1) they had a child from 1 to 21 years of age, and (2) had to be able to read and speak Dutch. The goal was to have a broad sample of parents to participate in the cognitive interviews, including those with varying levels of education, variety in native language, and children with a variety of physical, cognitive and/or behavioral disabilities as well as typically developing children in a wide range of ages from 1 to 21 years. Although the original PEDI-CAT has not yet been validated for self-report by adolescents, the developers have encouraged the exploration of self-report by adolescents [20]. Therefore, some adolescents (from 16 to 21 years of age) were included in this step.
Participants were recruited through open invitations via social media (i.e. Facebook and Twitter), the parent organization BOSK, and Rehabilitation Center De Hoogstraat. The following demographic data were collected: parent’s gender, residence, educational level and native language; and child’s gender, date of birth, disability and use of walking devices. Table 2 describes the characteristics of the participants.
Procedure
The Dutch PEDI-CAT items (including the response options) were tested through Think Aloud interviews, which is a cognitive interviewing method that aims to reveal the mental process of respondents while answering a question [21, 22]. These interviews were conducted by two people (authors NB and NvR), each interviewing 11 participants. The individual interviews took place at either the participant’s home or at De Hoogstraat Rehabilitation in Utrecht, The Netherlands. In order to prevent participants from having to go through all 276 items, items were pre-selected by the Dutch PEDI-CAT study-group. The unambiguous translated items agreed upon by all members of the study-group were left out of the Think Aloud interviews. The remaining items were sorted based on the age of the child so that only relevant items were presented to participants.
Participants were provided with instructions and asked for permission to record the interview. During the interview, participants read and answered the items aloud and, at the same time, talked about how they interpreted the item and how they arrived at their answer. If the participant hesitated, the interviewer started to ask questions, such as: “How would you rephrase that sentence in your own words?” or “How do you interpret […]?”. To encourage participants to focus on the meaning of the items, the illustrations of the Daily Activities and Mobility domains were not shown.
Number of adjusted Dutch translated PEDI-CAT items and reasons to adjust the
translation
Number of adjusted Dutch translated PEDI-CAT items and reasons to adjust the translation
*PEDI-CAT domains: DA
A qualitative analysis was performed. All items with at least one comment were reviewed by the two interviewers to see if a change in wording was necessary. This resulted in two lists: items that did not require a modification of the translation, and items that required some modification. The wording of a translated item was not changed if: (1) the corresponding illustration clarified the meaning of the item; (2) a change in the translation would lead to another interpretation of the item; (3) a comment did not lead to an improvement of the translation; and/or (4) a comment was due to inadequate proficiency in the Dutch language. The wording of a translated item was changed if (1) a spelling or grammatical error was present; (2) a word was unclear for at least one participant; (3) an item was confusing for at least one participant; (4) there was an unnecessary word; and/or (5) an item contained an unusual example. Two authors (NB and NvR) proposed modifications of the items that required some changes. Their recommendations were reviewed and discussed with a third author (MK) until a consensus was reached.
Results
Consideration of item equivalence
All items were assessed as relevant by all members of the Dutch PEDI-CAT study-group. Two hundred sixty-seven items were identified as Category 1, items that could be translated “as is”. Nine items were identified as Category 2, which required only minor modifications, which included Imperial Measures (e.g., feet and pounds) that were converted into the Metric System; dollars that were converted into euros; and some examples of items required minor modifications. No items were identified as Category 3 or 4.
Translation and back-translation
All items and the response scales were translated into Dutch. The back-translation into English was discussed with the developers of the PEDI-CAT. No changes were considered necessary.
Consideration of semantic equivalence
Of the 276 items, 175 (63.4%) were selected by members of the Dutch PEDI-CAT study-group to evaluate whether the translated items and ratings were understood as intended by parents and adolescents through Think Aloud interviews.
Out of a total of 175 items, 101 (57.7%) items were commented on or were unclear to one or more participants. Moreover, the Think Aloud interviews revealed that in some cases the translation of one of the response options was not clear. The translation of the lowest response option (unable: Can’t do, doesn’t know how or is too young) in the three functional skills domains was often interpreted erroneously. Participants thought that this response option could be used in situations where their child did not perform an activity because the child’s skills were beyond this level, or the child simply did not do this activity, even though they had the ability. The translation clearly was misleading to participants and resulted in answers that did not fit with the exact meaning of the response option. Therefore, the wording of this response option was adjusted. It was then indicated that this option should only be selected if the child is unable to perform the activity.
On item-level, 55 of the 101 items were not adjusted because: (1) the corresponding illustration clarified the meaning of the item (7 items); (2) a change in the translation would lead to another interpretation of the item (5 items); and/or (3) a comment did not lead to an improvement of the translation (33 items). Finally, two non-native Dutch participants had problems understanding the exact meaning of ten items because of inadequate proficiency in the Dutch language. These items were ultimately not changed because they were clearly related to language issues. If the interviewer explained the content verbally, both non-native Dutch speakers understood the items as intended.
The wording of 46 items was adjusted as a result of the Think Aloud interviews (Table 3). Three items had to be adjusted due to a spelling or grammar error. The wording of 21 items was adjusted because a word in the translation was unclear for at least one participant. This was often a word that was present in several items, such as the words “signs” and “item”, which appeared in four and three items respectively. In most cases, the relevant word was replaced with a synonym. The wording of 14 items was confusing to one or more participants. Different strategies were used to improve the translation of these items, such as adding an explanation, changing the order of the sentence or changing the wording of the item. Four items contained an unusual example; in this case the example was changed. Another four items included an unnecessary word. In that situation, the unnecessary word was removed.
Discussion
In this study, end-users played a central role in the Dutch translation and cross-cultural adaptation of the PEDI-CAT, which included item equivalence, translation and back-translation, and consideration of semantic equivalence. All 267 items and the ratings of the original PEDI-CAT were assessed as relevant and were translated into Dutch. After translation and back-translation, members of the Dutch PEDI-CAT study-group including parent representatives and professionals, selected 175 (63.4%) items in order to evaluate whether the items were understood as intended. Based on cognitive interviews with parents and adolescents, minor adjustments were made to the wording of 46 items and one particular response option was adjusted.
If measures are to be used across cultures, the items must not only be accurately translated linguistically, but they also must be adapted to fit culturally in order to maintain the content validity of the instrument at a conceptual level [13, 14]. For the PEDI-CAT, this process involved several steps, with end-users playing an important role throughout. Parents, adolescents and professionals were crucial in ensuring that the translation process yielded a new culturally-appropriate version, and that items were interpreted similarly in the original and new culture.
The input of end-users was especially important in the steps where the semantic equivalence of the translated PEDI-CAT was examined and where cognitive interviewing was used to evaluate whether the translated items and response options were understood as intended by parents and adolescents. Cognitive interviewing was conducted with Think Aloud, an evidence-based, qualitative method specifically designed to investigate whether a survey question fulfills its intended purpose [22]. This method relies on interviews with individuals who are specifically recruited. In this particular situation, a varied group of parents was recruited with children from a wide age range. They were diverse in terms of levels of education and native languages, and whether their children had physical, cognitive and/or behavioral disabilities. Moreover, two adolescents (from 16 to 21 years of age) were included in this process.
Cognitive interviewing as a strategy has some limitations; with this method, it is not possible to provide quantitative information about the impact of issues in the translation [21]. Some participants found it difficult to verbalize their mental processes; others found the cognitive process hard to verbalize, especially when the answer was very easy. However, the method of targeted and retrospective probing, combined with the high degree of diversity in this group, was very helpful in the process of cross-cultural adaptation. When an item was not exactly clear for at least one person, the wording of that item was discussed. The adolescents who participated did not come up with different issues compared to the parents. In general, there were only minor adjustments to items, which included fixing some errors in spelling, changing confusing or misleading examples, and adding some examples and specific terms to clarify the meaning of an item.
Two issues are important to discuss. The first concerns a response option that was not interpreted unequivocally by all participants. The PEDI-CAT is an assessment measure that focuses on performance of skills in daily life situations. The scoring of the lowest response option (unable) was discussed with the developers in an early stage, because the members of the Dutch PEDI-CAT study-group felt it was important to distinguish between capability and performance [23]. To emphasize a child’s performance instead of the ability to perform daily tasks, it was decided (with the developers’ approval) to translate the lowest response option so that the performance was central. The Dutch translation of “does not” was used for this response option. The explanation that follows “can’t do, doesn’t know how or is too young” was translated literally into Dutch. However, in some cases, parents used the option “does not” to indicate their child does not perform a specific activity because the child’s skills were past this level, or to indicate that their child does not perform the activity, even though the child is capable of doing it (e.g. the child is capable of riding a bicycle, but does not do it because the child does not like this activity). After discussion with the Dutch PEDI-CAT study-group and in consultation with the developers of the PEDI-CAT, the translation of this response option has been adapted to clarify this option.
The second important finding was the difficulty of understanding the exact meaning of some items by two non-native Dutch participants, despite the selection criterion “able to read and speak Dutch”. If the interviewer explained the content verbally, both participants were able to understand the item. Therefore, this finding did not lead to adjustments in the items. It is important to realize that some PEDI-CAT items may be difficult to understand because of language proficiency. This will probably not cause problems in the actual use of the PEDI-CAT in clinical practice. There were only minor issues with ten items, and the PEDI-CAT has the option to choose “I don’t know” as an answer in these cases. With this response option, the CAT algorithm automatically chooses another relevant item. For people with inadequate reading proficiency in the Dutch language, it is recommended that they use the PEDI-CAT with assistance.
The Dutch PEDI-CAT has taken its first steps. The role of end-users in the process of translation and cross-cultural adaptation was crucial. This collaborative process resulted in a Dutch version of the PEDI-CAT that has been optimally adapted to the Dutch language and culture.
Footnotes
Acknowledgments
The authors are grateful to all parents that participated in this study. The Dutch PEDI-CAT study group contributed to this study, and consists of A. Dallmeijer, VU Amsterdam; J. Verheijden, BOSK Utrecht; J. Wassenberg-Severijnen, Utrecht University; J. Custers, University of Applied Sciences Utrecht; H. Gorter, Roessingh Rehabilitation Enschede; G. Verkerk, Academic Medical Center Amsterdam; J. Voorman, Wilhelmina Children’s Hospital, UMC Utrecht; M. A. Kuijper and I. van Wijk, De Hoogstraat Rehabilitation, Utrecht. This study was financially supported by the research foundation De Hoogstraat Rehabilitation, Utrecht, The Netherlands.
Conflict of interest
Richard Moed is a co-owner of CREcare which distributes the PEDI-CAT. The other authors have no conflict of interest to report.