
Abstract
PURPOSE:
To investigate the effects of robot-assisted gait training (RAGT) alongside conventional therapy on the standing and walking abilities of children with cerebral palsy (CP).
METHODS:
The study sample consisted of children (aged 4–18 years) with CP whose gross motor function classification system (GMFCS) was at levels I–V. In total, 75 children with CP were evaluated and 38 patients completed the study. Patients were divided into two groups as GMFCS levels I–III (Group 1) and levels IV–V (Group 2). RAGT (30 min/session) and conventional physiotherapy (30 min/session) were applied together in the treatment. The treatment duration was 60 min per session, 3 or 4 sessions per week, for a total of 30 sessions over 8–10 weeks. 10-meter walk test (10MWT), 6-min walk test (6MinWT), gross motor functional measurement 66 (GMFM66) -D, and -E tests were performed.
RESULTS:
We showed that in both groups of CP patients (mild-moderate and severe), meaningful improvements were seen in the standing (D) and walking (E) sections of GMFM-66 after treatment. When we compared the post-treatment changes in 10-m walk test, 6-min walk test, GMFM66-D, and -E between Groups 1 and 2, we noted that the improvements were statistically significant in favor of Group 1 (
CONCLUSION:
RAGT in combination with a conventional treatment program was significantly associated with improvements in the standing and walking abilities of children with mild to moderate CP (GMFCS levels I–III).
Keywords
Introduction
Cerebral palsy (CP) comprises a permanent, non-progressive group of movement and posture disorders caused by damage to the brain of a developing fetus or infant [1, 2, 3]. CP is the most common cause of motor dysfunction in childhood [4, 5]. The incidence of CP is 2–3 per 1000 live births in developed countries [1, 6]. The main characteristics of children with CP are muscle weakness, spasticity, contractures, deformities, and postural instability. As a result, 90% of children with CP have difficulty walking [4, 7].
The gold standard in CP rehabilitation is multidisciplinary in nature [8]. Thus, physiotherapy, occupational therapy, orthoses, medications, and orthopedic and/or neurosurgical operations form the center of treatment [9]. Standing and gait rehabilitation have a major place in CP treatment. Independent gait development is an important therapeutic goal for many children with CP [10]. For this purpose, the search for alternative solutions to so-called conventional exercises started many years ago. First, body weight-supported treadmill training (BWSTT) was used. BWSTT improves walking ability and endurance in children with mild to moderate CP and in adult stroke patients [10, 11, 12]. The limitations of BWSTT treatment also resulted in new developments in the field of rehabilitation engineering. The problem with stimulation tolerance and BWSTT’s failure to contribute to the acquisition of functional movements resulted in the development of robot-assisted walking systems [13, 14].
Compared with other exercise methods, robot-assisted gait training (RAGT) has advantages, such as maintaining a more intensive, longer-lasting, and highly patient-oriented exercise program and objectively monitoring the effectiveness of the treatment [15, 16]. In RAGT sessions, treatment parameters such as speed, walking distance, walking duration, body weight support, and guidance forces are defined and recorded, therefore allowing easy comparisons between patients. This provides new opportunities for both research and special patient treatment programs [15, 16]. For these reasons, RAGT has been used frequently in recent years. Moreover, to enhance neuroplasticity, current theories have focused on task-specific training and motor learning. Through task-specific training, continuous repetition and intensive functional training provide effective treatment in support of motor learning [17, 18, 19, 20].
RAGT based on these concepts has proven effective and reliable in improving walking ability in children with CP and in adult patients with stroke and spinal cord injuries [15, 21, 22, 23]. When considered from this point of view, RAGT can play a complementary role to conventional physiotherapy [15, 17, 24]. Despite the general acceptance and popularity of RAGT among patients and parents, well-designed controlled trials are necessary for its further development in clinical practice [15, 17]. Also, additional studies are needed to standardize the treatment concept, as patient diagnoses, treatment protocols, and additional therapies differ from study to study [25].
In this study, we sought to investigate the effects of RAGT alongside conventional therapy on the standing and walking abilities of children with different types of CP classified according to motor function.
Methods
Setting and participants
The study sample consisted of children (aged 4–18 years) who were diagnosed with CP by a resident doctor and who admitted to the Private Aktif physical medicine and rehabilitation central. All children with CP who admitted to the clinic with various types of chronic gait disturbances whose gross motor function classification system (GMFCS) score were at levels I–V were enrolled [26]. As a inclusion criteria, the children were capable of expressing pain, fear, or discomfort, and parents of each patient signed the informed consent form before the study started. This research was conducted between October 2015 and October 2016. The femur length of all patients was at least 21 cm (device limitation), corresponding to children aged 4 years and older. RAGT was performed at the Private Aktif physical medicine and rehabilitation central. Exclusion criteria were a botulinum toxin injection within 4 months, orthopedic surgery (soft tissue release) within the last 6 weeks or lower limb osseous surgery within 12 weeks, severe spasticity (grades 3 and 4 according to Modified Ashworth Scale) or lower extremity contracture that would interfere with the use of RAGT, fractures, osseous instabilities, severe osteoporosis, thromboembolic diseases, cardiovascular instability, aggressive or self-harming behaviors, scoliosis (Cobb angle
Study flow chart.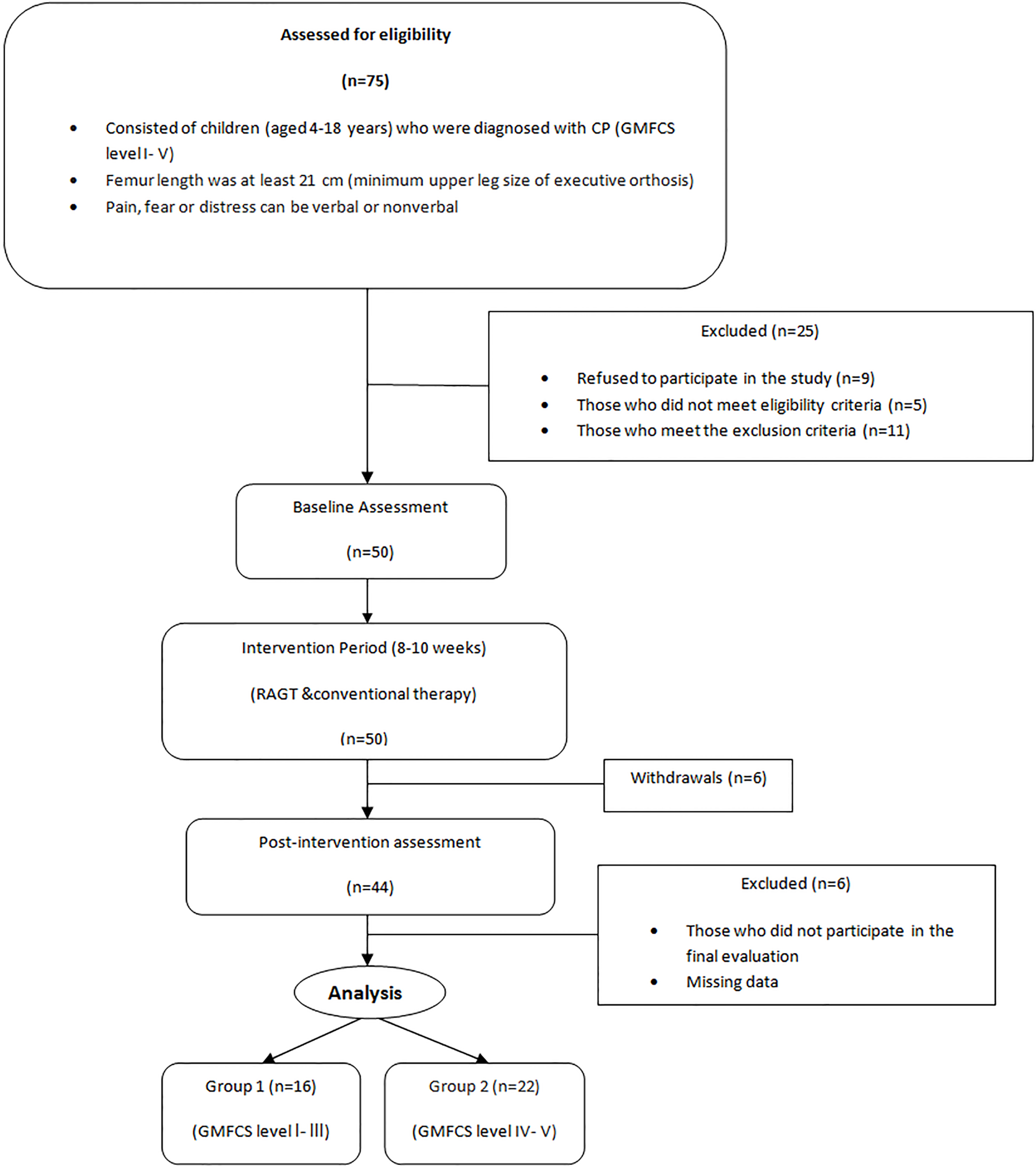
The RAGT device, Robogait
Interventions
RAGT and conventional physiotherapy were applied together in the treatment of children with CP. The treatment duration was 60 min per session, 3 or 4 sessions per week, for a total of 30 sessions over 8–10 weeks. RAGT was used as the basic intervention tool for patient special walking training, and at least two sessions each week were performed using RAGT for 30 min.
Also, conventional physiotherapy (space therapy, occupational therapy, massage, sensory integration therapy, stretching, joint movement, and strengthening exercises), standardized for all children, was performed every session during the whole treatment course. Conventional physiotherapy sessions lasted for 30 min during RAGT sessions and for 60 min during other treatment sessions.
During RAGT sessions, walking speed started at 0.3 km/h and then increased to 1.2 km/h according to the clinical characteristics of the patient. Body weight support was started at 100% and then reduced as much as possible according to the body burden and the knee flexion angle by adjusting for each patient individually. The least possible support was provided 50%.
Study design and outcome measures
This is a cross-sectional study. Clinical and demographic characteristics of the study sample (age, gender, age of diagnosis, type of delivery, drug use, botulinum toxin injection, orthopedic surgery history) were recorded. The patients’ CP type and GMFCS levels were determined by a attending doctor. The participants were classified into two groups according to the GMFCS level as mild-moderate (GMFCS levels I–III per group 1) or severe (GMFCS levels IV–V per group 2). The mildly to moderately affected group was designated as usually able to walk without the need for walking aids, whereas the severely affected group consisted of patients who were mobile with a wheelchair or who could not walk without assistance. All patients were evaluated pre-intervention (1 day before the first session) and post-intervention (1 day after the last session).
The Gross Motor Functional Measurement 66 (GMFM-66), which comprises 66 test items categorized according to five developmental dimensions, is a safe and useful standard observational tool measuring rough motor functions in children with CP. High scores in GMFM-66 show that rough motor functions are better. Experienced physiotherapists tested patients on the GMFM dimensions D (standing) and E (walking, jumping, running). GMFM-66 (D) and (E) scores were determined for statistical analyses as follows: GMFM-66 (D) score
Maximum walking speed and endurance were assessed by a physiatrist with a 10 meter walk test (10MWT) [30, 31], and a 6-min walk test (6MinWT) [32]. The GMFM-66 parts D and E, and the 6MinWT and 10MWT were performed after resting 10 minutes because repeated tests can lead to fatigue and performance.
The 6MinWT assessment was accomplished at a hospital using 10 meter repeats with turns along a 13.5 meter long, smooth, flat, uncluttered corridor with patients being instructed to: ‘walk for as long as you are able’. Patients were not provided with a rest break and once they stopped walking, irrespective of whether they completed the 6 minutes, the test was ended. In the 10MWT, the time taken (seconds) to walk 10 meter with a dynamic start, in the same environment was recorded [30].
The children were evaluated with assistive walking tools (orthoses, shoes, walkers, walking sticks) if they regularly used them. The RAGT system recorded average and total walking time (min), distance (m, km), and speed (m/s, km/h).
Statistical analyses
All statistical analyses were performed using the SPSS software (ver. 22.0; Chicago, IL, USA). Non-parametric test results are presented as the median. Some descriptive data (age, diagnosed age, and robotic therapy parameters) are presented as the arithmetic mean and standard deviation (SD). Normality of the data was assessed using the Shapiro-Wilk test. The non-parametric Mann-Whitney U-test and the Wilcoxon Signed Rank test were used because the variables (GMFM-66 parts D and E, and the 6MinWT and 10MWT) were not normally distributed. The Mann-Whitney U-test was used to compare groups at pre- and post-intervention measures (between-group comparisons). The Wilcoxon Signed Rank test was used to compare the results of tests performed pre- and post-intervention (within-group comparisons). The data for these tests are the differences in pre- and post-intervention measurements. For all analyses,
Results
In total, 75 children with CP and central gait disturbances at different GMFCS levels (I–V) were evaluated; 25 of these did not meet the inclusion criteria or refused to participate and were excluded. Thus, the study continued with 50 children. After the 8–10-week intervention (RAGT and conventional PT) period, 38 patients completed the study. Later, we classified the patients in two groups for statistical analyses (Fig. 1).
Clinical characteristics of the 38 participants
Clinical characteristics of the 38 participants
Patients’ data and robotic therapy parameters
f: female, m: male, n: Number of patients, SD: standard deviation, GMFCS: gross motor function classification system, min: minute, km: kilometer, m/s: meter/second, km/h: kilometer/hour,
Table 1 shows the basic demographic and clinical characteristics of the study sample. The mean (SD) age of the patients and the age at diagnosis were 7.8 (3.8) and 14.5 (12.6) years, respectively. Of the 38 children, 22 were males, and 19 had spastic tetraplegic-type CP. There were 22 patients in group 1 (GMFCS levels I–III) and 16 in group 2 (GMFCS levels IV–V).
During a mean (SD) of 15 (2.9) training sessions, patients walked a mean of 303.1 (48.6) m during a mean of 31.1 (3.5) min per session on the RAGT. The mean (SD) of total distance walked per patient during the trial was 4.5 (1.2) km. Individual details of patient data and RAGT parameters are shown in Table 2.
Differences within group
With respect to the GMFM score, the change in the median standing score (D) between pre- and post-intervention in group 1 was from 56.4% to 76.9% (
RAGT, 10 MWT, 6 MinWT results pre- and post-intervention in the groups 1 and 2
RAGT, 10 MWT, 6 MinWT results pre- and post-intervention in the groups 1 and 2
D: standing dimension, E: walking, running, jumping dimension, GMFCS: gross motor function classification system, GMFM66: Gross Motor Function Measure 66, 6MinWT: 6-minute walk test, 10MWT: 10-m walk test, pre: pre-intervention, post: post-intervention, imp: improvement, %: percentage, m: meter, m/s: meter/ second, Group 1: GMFCS levels 1–3, Group 2: GMFCS levels 4–5,
The median change in the scores on the walking section (E) from pre- to post-intervention from group 1 was from 38.9% to 59.7% (
Median maximum walking speed assessed with the 10MWT in group 1 improved from 0.7 m/s to 1.0 m/s, representing an increase of 20.7% (
Median walking endurance assessed with the 6MinWT in group 1 improved from 195 m to 215 m, representing an increase of 8.7% (
When we compared the post-treatment changes in 10MWT, 6MinWT, GMFM66-D, and -E between Groups 1 and 2, we noted that the improvements were statistically significant in favor of Group 1 (
Discussion
Cortical motor learning is directly related to the intensity and frequency of training, which is strengthened by therapy focused on education in walking [33]. In this respect, RAGT offers almost ideal conditions for specific gait training due to its ability to increase its intensity and frequency while continuing a physiological walking pattern [15]. Several RAGT studies performed on children with CP have reported that RAGT had positive effects on activity parameters such as standing, walking speed, and distance [34, 35]. However, the evidence for the use of RAGT for children with gait disturbances is weak and controversial [34]. Thus, there is a need for further studies to clarify the effectiveness of training programs by monitoring patient outcomes [34]. In this study, we described the effects of the RAGT program we implemented as a basic intervention for gait training in functional walking and standing parameters on children with CP and gait disturbances. We also evaluated improvements in these parameters by classifying patients into two groups according to their GMFCS levels (i.e., mild-moderate or severe).
This cross-sectional study showed the treatment effect of RAGT, combined with conventional physiotherapy, on the standing and walking function in CP children with central gait disorders. The magnitude of the positive effect was evaluated and compared based on GMFM-66 (D and E) scores, 10MWT, and 6MinWT, as in other studies conducted on children with CP [15, 17, 35].
We showed that in both groups of CP patients (mild–moderate and severe), meaningful improvements were seen in the standing (D) and walking (E) sections of GMFM-66 after treatment. Although there was a 26% increase in walking speed in 10MWT results after treatment and a 21% increase in walking tolerance in 6MinWT in the mild-moderate group, there was no significant increase in the severely affected group.
When we compared the two groups, we observed that all improvement scores were significantly higher in cases with mild to moderate CP. Previously, it has been emphasized that repeated referent-specific walking therapies are beneficial, resulting in significant improvements in the GMFM-D and E scores of children with central gait disturbance [17]. Beyond GMFM-E scores, repeated referent-specific walking therapy has additional beneficial effects, such as stabilization of the upright posture and improvement in GMFM-D scores [25]. Our results were consistent with literature showing that the GMFM-D and E scores of patients were improved after the therapies [17, 25].
BWSTT has traditionally been used as a specific walking training method in children with CP. Furthermore, previous studies conducted with BWSTT have revealed significant improvements in the GMFM-D and E scores of children with CP [10, 12]. However, there is still no general recommendation for the duration or intensity of this treatment [15]. Additionally, BWSTT has limitations, such as the lack of total recovery of the physiological walking pattern and the need for more than one person in attendance during the process [15]. Although the protection of the physiological gait pattern provided by RAGT is accepted as an advantage over BWSTT, further studies are needed to compare the two approaches [25]. Schindl et al. [11] found that RAGT and BWSTT had equal therapeutic efficacy in GMFM-D and -E scores. However, it is hard to compare these data with other studies in the literature due to differences in the numbers and ages of patients and treatment protocols [25]. In our study, although RAGT and BWSTT were not compared, the fact that RAGT can provide a physiological walking pattern and can be done by a single physiotherapist remains an important advantage.
Wang et al. [36] suggested that a 3.7% increase in recovery rates of GMFM would be clinically significant. In our study, the recovery rates of all participants were 7.8% in GMFM-D and 5.5% in GMFM-E. Moreover, in the group of mildly to moderately affected patients, improvement rates were 14.4% in GMFM-D and 10.8% in GMFM-E scores, indicating statistically and clinically significant changes. Although improvement rates in GMFM-D (3.03%) and GMFM-E (1.7%) were statistically significant in the severely affected CP group, RAGT application did not show clinically significant improvement in their standing and walking abilities.
Improvements in the walking speed and stamina of children with CP have meaningful positive impacts on their interactions with peers and other people, especially by allowing short-distance walks [15]. RAGT can provide a positive contribution to daily life activities, based on walking in mildly to moderately affected patients by significantly improving their walking speed and duration.
Children with CP who have good motor skills have been reported to have greater ability compared with those having lower motor strength [17, 26]. However, in contrast, it has also been reported that treadmill treatment is more effective in the motor functioning of children classified as GMFCS levels III and IV [37]. Another study conducted in children with GMFCS levels II and IV showed that even though the level IV patients walked less with RAGT, they had significant improvements in gait-related outcomes [24]. This inconsistency may be caused by heterogeneity in the studies and differences in outcome measures [17]. In our study, improvements in standing and walking abilities, walking speed, and endurance in children with high motor skills (GMFCS levels I–III) were more clinically significant than were those in children with GMFCS levels IV–V.
Limitations
This study has some limitations. First, a control group could not be created because nearly all parents chose to use RAGT instead of conventional therapies. We wanted to separate robot-assisted therapy from the conventional method and then make comparisons, but it was impossible to convince the parents of children with CP to only use the conventional therapies for their children’s treatments. This situation prevented our comparing the effect of an alternative course for children with CP on outcomes. Second, those who evaluated the results were not blinded before and after treatment. However, the evaluators were neutral physiotherapists and physiatrists who were not otherwise involved in the study. Another limitation is that patients were grouped as levels I–III (mild to moderate) and levels IV–V (severely affected) according to GMFCS, which may be considered arbitrary. However, we took into consideration the significant similarities of patients in establishing these groupings. In addition, exclusion criteria and refusal to participate may affect the results of the study.
Our research also had some strong points. First, there is no general recommendation about the duration or frequency of walking therapy in children with CP [25]. Peri et al. [38] found that RAGT seems to have similar effect with respect to the traditional therapy, at least over a 10 week period. Nevertheless, we found that the average duration of therapy in the literature is between 3–12 weeks and that the average duration of physiotherapy programs that caregivers or parents prefer is 30 sessions over 8–10 weeks; the addition of 15 sessions of RAGT is a strong point of this study [15, 17, 25]. We made the RAGT sessions 30 min in duration, which is consistent with other studies in the literature, where they have ranged from 20 to 60 min [15, 17, 25, 27].
This study has shown that the mean velocity/session value is 0.16 (m/s), which is below the average of 0.4 to 0.5 (m/s) in the literature [15, 17, 25]. Thus, despite the mean duration of 30 min, the mean distance/session values were detected as 303 m in our study, below 470 m to 1150 m in the literature [15, 17, 25]. The mean velocity was kept low in our study for increased tolerability and compliance of patients with the RAGT device used for the first time.
Moreover, we used established and common evaluation tools in our study, namely GMFM-66 test D and E scores and the 10-m and 6-min walking tests, which offered good functional assessments of patient walking capabilities.
It has been noted in previous studies that the biofeedback system adopted for increasing patients’ participation in treatment and maximizing efficacy during RAGT session is important [15, 38]. It is thought that gait training in a virtual reality-based environment would be useful, provided that this feedback system is specifically developed for children and integrated into RAGT [39, 40].
In our study, the virtual-reality biofeedback system was not used because it is not specific to children and there are difficulties in patients’ adaptation to such a system. To maintain compliance during the therapy session the patients were allowed to listen to music or watch a favorite cartoon. Additionally, no undesirable side effect was reported by the patients or their families in the RAGT process.
In future studies with RAGT in children with CP, randomized controlled studies with larger numbers of patients are needed to determine more clearly the level of improvement in standing and walking functions according to motor ability level.
Conclusions
Repeated referent-specific walking therapies are known to be useful in children with CP who have central gait disturbances. However, conflicting results have been reported on improvement in the levels of motor ability shown by these children. In our study, RAGT in combination with conventional treatment program was significantly associated with improvements in the standing and walking abilities of children with CP. However, after RAGT combined with conventional treatment, children with mild to moderate CP (GMFCS levels I–III) had clinically more significant improvements in standing and walking ability than did those who were more severely affected (GMFCS levels IV–V).
Footnotes
Acknowledgments
We thank physiotherapists Nihat Bakırcı, Zeynep Zengin, Özge Büyükdoğan and Çağkan Çağlar, who contributed to the evaluation and data collection of patients. We thank the doctor Murat Uludağ for his consultative role. The authors declare that this study has received no financial support.
Conflict of interest
The authors report no conflicts of interest.