
Abstract
There is a considerable risk of malnutrition for children with Cerebral Palsy (CP) due to insufficient nutritional intake. The most important causes of insufficient intake are feeding problems which are highly prevalent in children with CP (depending on definition, age and heterogeneity of the researched population). Considering these facts, nutritional status should have the full attention of healthcare professionals but this is not yet the case. Evidence from research in clinical practice suggests that: 1) there is no consensus regarding who should perform the measurement and how often, 2) no standardised nutritional assessment is implemented, and 3) there is suboptimal communication and management about feeding and nutritional status in most healthcare networks.
To overcome these problems, validated and practical tools for the screening and assessment of nutritional status should be a topic of research and subsequently made available and implemented in clinical practice. Because body composition is an objective indicator of available energy stores, research should focus on optimising measurement methods to determine body composition using anthropometric measures or bioelectrical impedance analysis (BIA). Furthermore, there is a definite need among health care providers for explicit and clear agreements on organisation and communication about nutritional care for children with CP.
Synopsis of the problem
In clinical practice, nutritional care for children with Cerebral Palsy (CP) does not meet the desirable quality standard (i.e., standardized and periodic evaluation of nutritional status). This may be due to a number of factors: 1) insufficient attention to nutritional status during doctor consultations, 2) no standardised nutritional assessment is carried out, and 3) suboptimal communication and management considering feeding and nutritional status among health care professionals.
These shortcomings may lead to missed treatment opportunities to improve health in these vulnerable children.
What this paper adds:
This paper outlines the contributing factors of current suboptimal nutritional care for children with Cerebral Palsy. It highlights the need for improving screening and assessment methods of nutritional status and organisation of nutritional care. It highlights the need among health care professionals for improving communication and organisation related to feeding and nutritional status. It gives suggestions for future research.
Nutritional challenges in children with CP
Depending on the researched population (age and heterogeneity) and used definitions, at least 19% of individuals with CP have feeding difficulties that may lead to malnutrition [1]. Extreme prevalence numbers (99%) can be found in the literature when considering children with severe CP [2]. Malnutrition in children with CP is a serious problem as it markedly increases their mortality rates [3] and worsens quality of life. Thus, nutritional status should have the full attention of healthcare professionals. The following case of Anna illustrates the omissions in clinical practice:
Anna is a six-year old girl with bilateral mixed type Cerebral Palsy. She walks with a walking aid (Gross Motor Functioning Classification System (GMFCS) level III) and has severe feeding difficulties because of oral-motor dysfunction, drooling, gastro-oesophageal reflux, recurrent periods of vomiting, and poor gastric emptying. Anna is completely tube fed, but occasionally, she is given a few bites orally for taste (Eating and Drinking Ability Classification System (EDACS) level V). Because of her swallowing problems, there is high risk of aspiration, leading to frequent respiratory tract infections. Despite extensive medical evaluation, parents report that they never received an explanation for the recurrent periods of vomiting.
At the age of 5.5 years, Anna learned to walk and is very proud of this accomplishment. Especially at school, she wants to walk and play with her friends as much as possible. Anna temporarily loses the ability to walk during exhausting periods of frequent vomiting and is unable to complete a full week of school attendance. In addition, she also loses weight during these periods.
This case shows the negative consequences of poor nutritional status on activities and quality of life.
Furthermore, it illustrates nutritional care should be optimized in healthcare networks, as set out hereafter:
To evaluate growth and nutritional status in “usual care”, Anna’s height has been measured with a standing calliper and weight has been measured with a scale device while she could barely stand up straight. From the age of 4 years, measurements have been carried out roughly every 6 months in an out-patient setting at paediatrician visits and have been recorded on a growth chart for typically developing children (Fig. 1). Reviewing the results, the consulted physician was satisfied and therefore expanded visit intervals to once every year. No other anthropometric measures or other (laboratory) diagnostic tests for nutritional assessment have been carried out. There are no further data about her ‘body composition’ (see also ‘What can we measure?’, body composition).
Growth chart for Anna.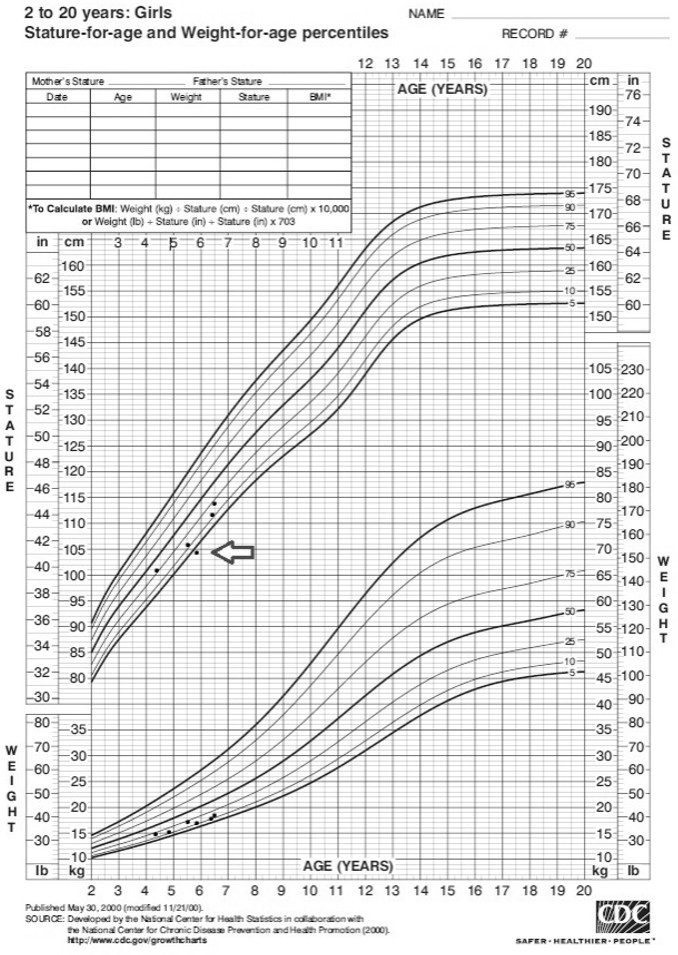
Currently, Anna and her mother regularly visit a ‘saliva control team’ for evaluation and treatment of her oral-motor problems. This team does not check nutritional status. Furthermore, a school-affiliated physiatrist and dietician are involved. Unfortunately, they do not have access to hospital data. Based on assumptions, the school team expects that specialists at the hospital will monitor Anna’s nutritional status. Occasionally, the dietician checks and adjusts the volume of the enteral formula according to age, but only when the mother asks for it.
In this case, the earlier mentioned problems are obvious: 1) there is an insufficient amount of attention given to nutritional status during doctor consultations, 2) no standardised nutritional assessment is carried out, and 3) there is a lack in communication and management considering feeding and nutritional status among healthcare professionals.
To investigate the extent of these shortcomings in clinical practice, a survey was conducted as part of a reliability study of the Dutch Eating and Drinking Ability Classification System (EDACS, accepted, 2017). Caregivers of 69 children with CP (child characteristics, Table 1) answered the following questions:
Demographics of participants
Demographics of participants
SCPE, surveillance of cerebral palsy in Europe; GMFCS, gross motor function classification system; EDACS, eating and drinking ability classification system.
What are the current height and weight measurements of your child? How often are height and weight measured? Who, among your child’s healthcare providers, feels responsible for evaluation of the height and weight?
The results are notable. Of the children, 36.2% (25/69) suffered from malnutrition (WHO definition of height/weight scores z-score
Scarpato et al. are calling for a practical approach of nutritional assessment for children with CP [4]. It is important that measurements are feasible in the outpatient setting, time efficient, inexpensive, and stress-free for the child and the parents. Repeated and reliable measurements should be carried out to prevent under or overdiagnosing, as well as starting nutritional intervention when unnecessary, putting the child at risk of becoming overweight.
Height and weight
As stated by the World Health Organisation, in typically developing children, growth monitoring is the best indicator of the health and nutritional status of a child [5]. Disturbances in health and nutrition, regardless of their aetiology, invariably affect the child’s growth. Height and weight measurements necessary to evaluate growth may be difficult to assess in children with CP; e.g. because of joint contractures that might complicate reliable measurement of height. Figure 1 (see the arrow) shows that in this case not all measurement points are in line with what can be expected based on age and growth pattern. Children may also be wheelchair users impeding adequate weight assessment. Thus, alternative approaches, like segmental measurements, may be necessary. An example of this is the calculation of approximate height from segmental measures like knee height [6]. After weight and height are measured or estimated, they are plotted on standard growth charts. These charts, based on healthy reference groups, can be used to monitor whether children remain in their growth curve, but they may not be suitable for conclusions about desirable growth and target height in children with CP. For example, children with CP who have GMFCS levels II-V are significantly shorter compared to ‘typically developing’ children. In an attempt to correct for this difference, CP specific growth charts were designed [3]. Unfortunately, there are three issues that introduce bias: 1) Segmental length formulas include some potential errors. For instance, when calculating body mass index (BMI), these errors are squared. 2) For the aforesaid reasons of feeding problems leading to risk of malnutrition, it is probable that some of the children from whom reference data were derived, were malnourished. 3) Because of altered body composition, height-for-weight and height-for-age measures do not properly inform the health care professional about available energy stores [7, 8, 9]. Therefore, solely depending on height and weight measurements as markers for ‘good nutritional status’ is insufficient in children with CP. Thus, the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) committee guidelines do not recommend the use of CP- specific growth charts [10].
Red flag warning signs
Red flag warning signs
Body composition, usually defined as the percentage of fat mass and fat-free mass, is a more objective indicator of available energy stores and therefore nutritional status [11, 12]. Body composition can be calculated indirectly from: 1) the deuterium dilution technique, 2) from dual-energy x-ray absorptiometry (DXA) scans and, double indirectly from 3) anthropometric measures like BMI and skinfold measurements [8, 13, 14, 15] and 4) bioelectrical impedance analysis (BIA) [16, 17, 18, 19, 20]. The deuterium dilution technique and DXA (indirect techniques) are mainly used in large-scale scientific studies because of their costs in terms of money and personnel. The double indirect techniques (BMI, skinfold measurements and BIA) are easy to use in clinical practice but their precision on an individual level is questionable and needs to be optimised [8, 13, 14, 15, 16, 17, 18, 19, 20].
Micronutrients
Along with the importance of ingesting enough fat, carbohydrates, and proteins, sufficient intake of micronutrients is crucial. Micronutrients consist of vitamins, minerals, and trace elements. They are important for many metabolic pathways and micronutrient deficiencies may affect cognition, behaviour, social interaction, developmental outcomes and hence quality of life [21]. Children with CP often eat less and non-diversified food compared to typically developing children, which puts them at risk for low micronutrient intake [22]. Also, when the child is exclusively tube fed, there is a risk of insufficient intake of micronutrients, because necessary amounts of micronutrients are only met when enough volume is consumed. Related to oral-motor and gastrointestinal impairment, volume intake is often reduced in children with CP. To assess the micronutrient status of a child, a blood sample needs to be collected which can be uncomfortable.
What should be measured?
Reviewing the options and pitfalls of the different measurement methods, it is a challenge to decide what measuring methods are applicable in which children and on what time interval. Valuing results in the absence of optimal reference values complicates these decisions even more. Until recently, there was no practical guideline for the clinical evaluation of nutritional status in children with CP. However, the ESPGHAN working group has developed guidelines for the evaluation and treatment of gastrointestinal and nutritional complications in children with neurological impairment [10]. Multiple suggestions and recommendations have been formulated with sometimes limited evidence to substantiate them.
The working group suggests combining measurements and ‘red flag warning signs’ for the identification of undernutrition in neurologically impaired children (Table 2). For now, this can be a practical and easily applicable tool to identify malnutrition. However, the identification of physical signs of undernutrition and used anthropometric measurements are prone to interrater variability [23]. These ‘red flag warning signs’ have not been validated yet. Statement 4 of this guideline suggests that children should have anthropometry assessment at least every six months and that micronutrients are checked annually. Because this guideline has not yet been implemented in clinical practice, the effects on nutritional management have not yet been evaluated.
Who should be measuring?
The case of Anna highlights that, beside the presence of a capable multidisciplinary team, it is crucial that there are regional agreements about who is responsible for each part of the nutritional assessment, who is responsible for the overall management, and that there is reciprocal communication among health care professionals and the child and/or parents.
Conclusion
There is a considerable risk of malnutrition for children with CP due to insufficient nutritional intake necessary for their needs. The most important causes of insufficient intake are feeding problems which are highly prevalent in children with CP (depending on definition, age and heterogeneity of the researched population) [1, 2]. Considering these facts, nutritional status should have the full attention of healthcare professionals but this is not the case yet.
Nutritional care in children with CP is complex, therefore, validation of practical tools for screening and assessment of nutritional status should be a topic of research. Subsequently, those tools should be made available and implemented in clinical practice (e.g. through education of health care professionals). Because body composition is an objective indicator of available energy stores, research should focus on optimising measurement methods to determine body composition (using anthropometric measures or BIA) [24]. Furthermore, there is a desperate need among health care providers for explicit and clear agreements on organisation and communication considering nutritional care for children with CP.
Footnotes
Conflict of interest
The authors have no conflict of interest to report.