
Abstract
PURPOSE:
The purpose of this study was to examine the effects of biofeedback therapy as a non-invasive intervention to treat Bladder Bowel Dysfunction in pediatrics.
METHODS:
Six databases were searched between February 2016 and September 2016. Biofeedback studies for children aged 4–16 with idiopathic urinary or fecal incontinence were included. Articles were excluded on subjects’ medical histories, study design, timeline of study, and lacking expert review. Quality was determined using Sackett’s Levels of Evidence and the PEDro scale.
RESULTS:
Twelve articles were included in the review. Quality of evidence was moderate, as the average PEDro score of the selected articles was 5.3. The participants’ ages ranged from 4–16 years old. Studies demonstrated that a multifactorial approach consisting of biofeedback therapy and behavioral modification can be successful in resolving Bladder Bowel Dysfunction.
CONCLUSION:
Biofeedback is a beneficial treatment for children with dysfunctional voiding and functional fecal incontinence. More conclusive research needs to be completed to explore the effects of biofeedback therapy treatment to make more concrete conclusions. Healthcare professionals should consider biofeedback as an alternative approach in conjunction with traditional treatments. A multidisciplinary approach is best when treating dysfunctional voiding and functional fecal incontinence in the pediatric population.
Keywords
Introduction
The term Bladder Bowel Dysfunction (BBD) encompasses both lower urinary tract (LUT) dysfunction and bowel dysfunction. The International Children’s Continence Society (ICCS) suggests that because the LUT and bowel have a close functional relationship that these systems should be grouped together [1]. BBD is common among school-aged children. The cause of BBD may be neurogenic or nonneurogenic. One disorder under the umbrella of BBD is dysfunctional voiding. Dysfunctional voiding is defined as habitual abnormal contraction of the urethral sphincter or pelvic floor during voiding [1, 2]. It is often the result of overactive pelvic floor muscles and excessive tightening of the urethral sphincter [1]. When this occurs, the common result is incomplete bladder emptying. Secondary symptoms include overflow or urge incontinence and urinary tract infection.
As mentioned earlier, concomitant bowel dysfunction may be seen with dysfunctional voiding. Studies have found that both disorders are closely related in the pediatric population. Functional fecal incontinence, also commonly referred to as encopresis, is defined as voluntary and involuntary passage of feces in inappropriate places in a child 4 years or older [2]. Further, like dysfunctional voiding, functional fecal incontinence may be caused by abnormal contractions of the associated external sphincter. Children with functional fecal incontinence often have chronic constipation and painful bowel movements. Cox et al. [3] suggests that this may be due to avoiding the bathroom and/or failing to maintain adequate intra-abdominal pressure during defection.
In addition to physical discomfort, children with dysfunctional voiding and functional fecal incontinence can experience emotional anguish in social situations or public places due to soiling or wetting their undergarments. Children who experience urinary or fecal incontinence in public are at higher risk for peer rejection and teacher alienation. Further, untimely urination and bowel movements may lead to undue parental punishment. This may result in deeper emotional issues such as humiliation, decreased self-esteem, familial estrangement, and withdrawal from social activities and friends [3].
According to the ICCS [1, 2], standard therapy for BBD consists of urotherapy. Urotherapy is a non-invasive, conservative treatment of lower urinary tract dysfunction. Standard therapy includes five basic components that include a variety of professionals. The five components include: providing information about the dysfunction and demystifying it, providing instruction on resolving the dysfunction, advising the patient on lifestyle changes, teaching the patient how to use a voiding diary, and providing support and encouragement from the caregiver [1]. In addition to previously mentioned factors, standard urotherapy can also include pelvic floor retraining, behavioral therapy, and psychotherapy if the standard proves ineffective for the child.
Biofeedback therapy is a readily available, non-invasive technique in treating pediatric pelvic floor dysfunction. Biofeedback used as a physical therapy intervention attempts to train the appropriate pelvic muscle activity necessary for normal bowel and bladder function. Two main types of biofeedback utilized by therapists in treating these dysfunctions are electromyography (EMG) and uroflow. EMG biofeedback tends to be used with functional fecal incontinence, while both uroflow or EMG biofeedback is used for dysfunctional voiding [4]. The treatment methods consist of training the child through video-like games, which provides direct feedback to relax previously contracted sphincters during bowel movements and urination. Though it has been shown to be effective in the treatment of women with pelvic floor disorders, there is a discrepancy regarding the effectiveness of biofeedback therapy in the pediatric population.
Purpose
Previous systematic reviews of the effectiveness of biofeedback for dysfunctional voiding and functional fecal incontinence have been conducted. However, they were either comprised of mostly low-level evidence or limited amounts of evidence [5, 6]. The authors felt that an updated systematic review was warranted. The purpose of this study was to examine the effects of biofeedback therapy as a non-invasive intervention to treat dysfunctional voiding and functional fecal incontinence in pediatric patients.
Methods
Study identification
Two searches of the literature were performed to identify appropriate articles for the review. The first search was completed between February and March 2016, and the second during September 2016 using PEDro, PubMed, and EBSCO (Medline, CINAHL) databases. Search terms used were “biofeedback,” “child”, or “children”, in combination with “voiding”, “encopresis”, “incontinence”, and “dysfunctional voiding”. See Fig. 1.
Methods.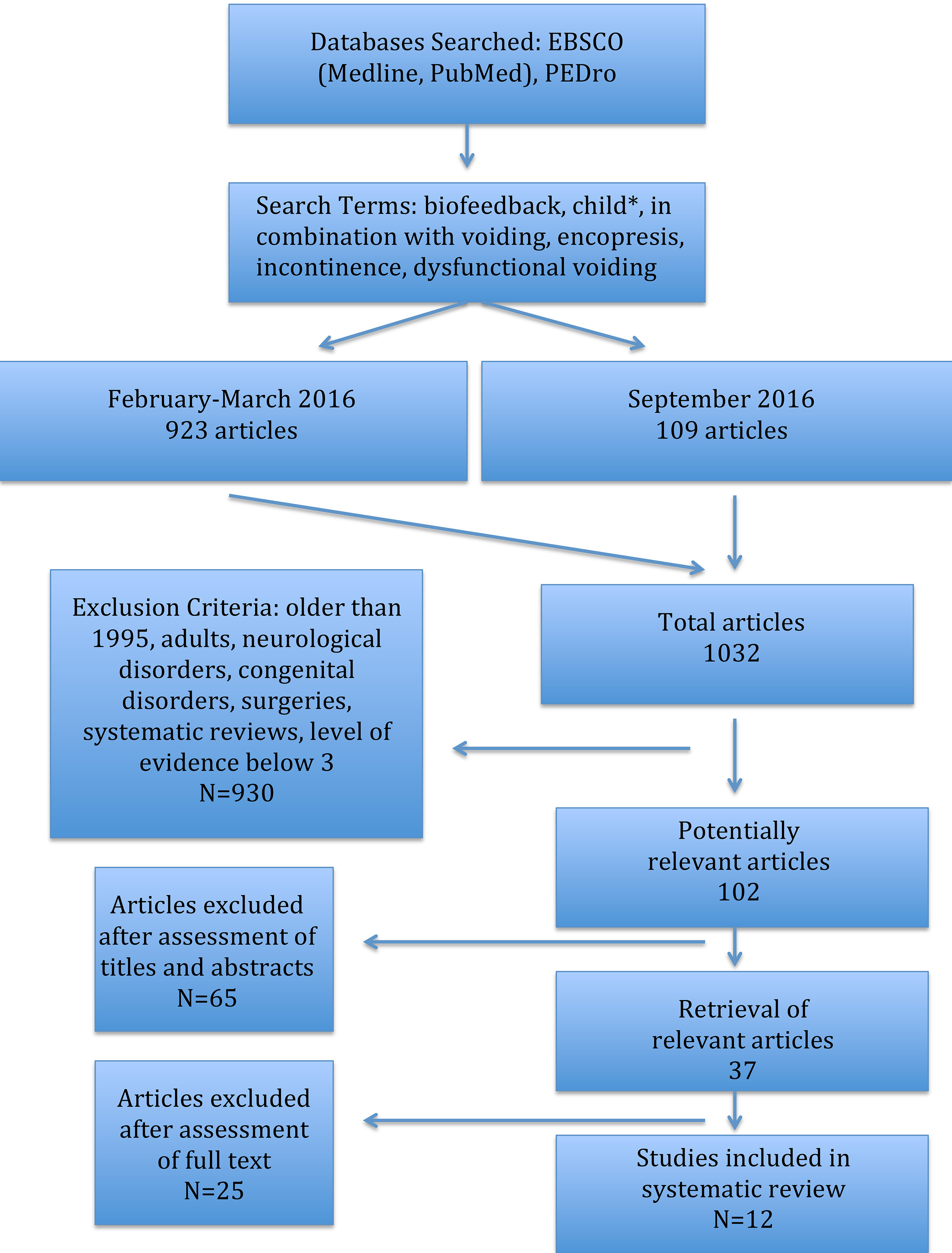
The inclusion criteria were 1) children with dysfunctional voiding, incontinence, and/or encopresis, 2) biofeedback as an intervention, 3) peer-reviewed articles, and 4) PEDro score four or greater [7]. Exclusion criteria for articles included 1) subjects with a neurological or congenital disorder and/or prior pertinent surgeries, 2) systematic reviews without meta-analyses, 3) were written prior to 1995, or 4) had hierarchy level of evidence four and below [8].
Validity assessment
The authors determined the validity of the individual studies utilizing the 10-point scale according to PEDro [7]. The PEDro scale is a measure of the methodological quality of clinical trials. After independently rating each article for their PEDro score, the authors conferred to discuss the ratings of each article and agreed upon a score. See Table 1. The authors determined that studies scoring below 4/10 on the PEDro scale were excluded from the study in order to incorporate the most credible information in the systematic review. Each article was also assessed independently for its level of evidence according to Sackett [8], and the authors again conferred on the scores. This information is presented in Table 2.
PEDro Scale Results
PEDro Scale Results
Thirty seven articles, according to their titles and abstracts, were identified by the authors to be relevant to this systematic review. Twelve out of the 37 articles were chosen based on the inclusion and exclusion criteria and were critically analyzed. Ten of the selected articles were randomized control trials (RCT) studies [3, 9, 10, 11, 12, 13, 14, 15, 16, 17], one was a comparative study [18], and one was a cohort study [19]. See Table 2. The participants’ ages ranged from 4–16 years old. The average PEDro score of the selected articles was 5.3.
In the reviewed articles, the results varied on the effectiveness of biofeedback in children with two separate diagnoses: dysfunctional voiding and functional fecal incontinence. In the majority of articles, the results were positive for biofeedback contributing to improvements in dysfunctional voiding, whereas the results were inconclusive for functional fecal incontinence. There was no defined difference in effectiveness of biofeedback with relation to older participants as compared to younger participants. Each of the studies had its own definition of “standard therapy” which may or may not have aligned with the definition provided by the ICCS. The following results are organized according to diagnoses and the alternative therapies applied.
Dysfunctional voiding
Of the 12 articles analyzed, seven examined the effects of biofeedback on dysfunctional voiding. Outcomes analyzed included urine flow, voiding episodes, post-void volume, flow curve, maximum urine, voiding time, and urinary tract infection (UTI) occurrence. All of the articles cited improvements in voiding as a result of biofeedback, although significant differences were not attained when compared to standard therapy. In a study by Zeng et al. [18], biofeedback helped to resolve 16 cases compared to six in a pharmacologic comparison group, suggesting that biofeedback be the first intervention attempted for children specifically with post-urination dribbling. In a study by Ladi-Seyedian et al. [16], animated biofeedback significantly improved voiding episodes, voiding time, and maximum urine flow in patients who underwent biofeedback training compared to patients who underwent only standard urotherapy at six months and one year after treatment. Although none of these studies had detrimental side effects, the effectiveness varied anywhere from measurable results to simply improve-
Question: What is the effectiveness of Biofeedback therapy in managing Bowel
Bladder Dysfunction in children?
Question: What is the effectiveness of Biofeedback therapy in managing Bowel Bladder Dysfunction in children?
ment in total relief or shorter treatment duration due to a learning curve [10, 14].
Computer games may augment the effectiveness of biofeedback as a physical therapy intervention, particularly by increasing the child’s level of active participation in the treatment. Khen-Dunlop et al. [19] found that there are two critical factors needed for biofeedback to be effective: a) there must be a relationship between the therapist, the patient, and the patient’s caregivers; and b) interactive computer games greatly contributed to the success of biofeedback in this population. Computer games increase the child’s attention span as well as teach proper pelvic floor muscle activity through visualization as a form of mental practice.
Six of the 12 studies examined the effects of biofeedback therapy on children with functional fecal incontinence [3, 11, 12, 13, 15, 17]. Two of the six studies reported positive improvements in symptoms with biofeedback therapy [11, 15]. In these studies, biofeedback therapy was found to reduce the use of laxatives as well as the episodes of incontinence. Furthermore, there is evidence that regardless of treatment location, solely in lab or at home, children presented with increased bowel movements in just 2 months with biofeedback therapy [15]. However, improvements in fecal and urinary incontinence were not experienced in all 12 studies. Four of the six studies found that biofeedback therapy did not contribute to the alleviation of symptoms in children with functional fecal incontinence [3, 11, 12, 17]. In those studies, biofeedback did not appear to provide relaxation of the pelvic floor muscles for defecation unless combined with other therapies such as laxative treatments and toilet training [3, 17]. However, although biofeedback therapy did not significantly improve functional fecal incontinence in children, it did improve the children’s behaviors in school. The authors are unsure why the children behaved more appropriately after biofeedback. However, it did appear to make a lasting impact to them, particularly in relation to social behaviors at school [12, 17].
Standard therapy
In addition to biofeedback, all of the studies included multiple interventions that are considered to be standard therapy for children with both of these disorders. Seven of the 12 studies included a conventional treatment group, in which dietary and toilet advice, enemas, laxatives, and diaries were utilized, as well as other varying standards of therapy [10, 11, 12, 14, 16, 17, 19]. Although behavioral modification was found to be important in reducing functional fecal incontinence, animated biofeedback therapy and pelvic floor exercises helped to diminish constipation and were able to completely resolve functional fecal incontinence [11]. In the sole study regarding post-urination dribbling, pharmacological therapy was incorporated as an intervention, in which one group was administered 1 mg of tolterodine twice daily. Biofeedback had a cure rate of 16 as compared to six cures in the pharmacologic group, suggesting that biofeedback should be the first intervention attempted for children with a disturbance of muscular coordination of the detrusor and sphincter urethrae with post-urination dribbling [18]. The remaining four studies examined the effects of enhanced toilet training, anorectal manometry, and uroflow parameters into their interventions in relation to biofeedback therapy [3, 9, 11, 15]. According to Cox et al. [3], toilet training was found to be the most beneficial route for children with functional fecal incontinence. The researchers found that enhanced toilet training required fewer treatments with a 76% reduction in incontinence. They noted that biofeedback therapy might contribute to more successful treatments if introduced after toilet training [3]. Standard therapies have been shown to be effective in conjunction with biofeedback treatments in decreasing the symptoms of dysfunctional voiding and functional fecal incontinence.
Discussion
This systematic review analyzed selected literature to determine the efficacy of biofeedback therapy as a non-invasive intervention to treat functional fecal incontinence and dysfunctional voiding in pediatric populations. The selected studies allowed us to examine the results of the intervention of various forms of biofeedback over a period of nearly ten years. Although levels of evidence remained limited, our review determined that children ages (4–16) with dysfunctional voiding can benefit from biofeedback therapy. Most of the articles examining voiding dysfunction had positive benefits from biofeedback therapy, including completely resolving 16 cases compared to six in the pharmacological comparison group in the Zeng et al. study [18]. In addition to measurable benefits related to the dysfunction, biofeedback also increased the patient’s participation in the therapy by making it fun and engaging, along with encouraging the mental practice of correct pelvic floor contractions [15].
Our research was unable to provide a more definitive conclusion on the efficacy of biofeedback therapy on functional fecal incontinence due to the limitations stated above. Some studies found an increase in number of bowel movements, while others found that biofeedback had no effect unless it was combined with adjunctive therapies [3, 15, 17]. A positive, yet unrelated effect of biofeedback on children with fecal incontinence is an improvement in social relationships and behavior at school. The authors were unable to identify a plausible reason why this effect occurred with the use of biofeedback, but nevertheless it is a positive side effect of the therapy [12, 17]. When analyzing these results together, it appears that a multifactorial approach consisting of biofeedback therapy and behavioral modification can be successful in resolving functional fecal incontinence, although further studies are necessary on the topic.
This systematic review had similar results when compared with other systematic reviews on dysfunctional voiding within the pediatric population. Desantis et al. [5] concluded that biofeedback is an “effective and non-invasive treatment for dysfunctional voiding, whereby approximately 80% of children benefited from the treatment.” Three of the articles they analyzed were also analyzed in our systematic review [10, 14, 19]. However, in the Desantis et al. [5] study, most of their findings were from case series with a low level of evidence, with only one RCT analyzed.
Fazeli et al. [6] performed a systematic review with a meta-analysis on the effect of biofeedback as an adjunctive therapy for symptoms of nonneuropathic voiding disorder in children. The meta-analysis pooled the data on 382 participants from four of the five studies examining resolution of urinary incontinence, incidence UTI, post-void residual volume, flow rate and mean maximal flow rate. Of the five articles they included with their study, three were also included in the current review [10, 13, 14]. Similar to our findings, Fazeli et al. [6] recognized that high quality RCTs on this topic are sparse and some findings support the use of biofeedback while others have shown no benefit. In the meta-analysis, Fazeli et al. [6] concluded that there was no significant difference in outcomes when biofeedback is used as an adjunctive therapy.
Limitations of our review
This systematic review has several limitations related to the quality of the articles included in the results. A majority of the articles exhibited a small sample size, thus reducing the power of the study [11, 16, 18, 19]. The time span for follow-up with the participants was often either short or non-existent [9, 10, 16, 19]. A limitation not directly related to the articles themselves was that the research available was sparse on current, innovative studies pertinent to the topic. Most studies were published in 2006 or prior, with only four relevant studies published after 2011. Finally, the differences among the studies’ assessment tools and outcome measures prevented the authors from conducting a meta-analysis.
Implications for practice
Physicians and physical therapists should consider the results of this systematic review in their clinical practice. In treating dysfunctional voiding and urinary incontinence, the evidence suggests that significant relief can be attained when biofeedback therapy is used in conjunction with other interventions. The therapist may want to consider alternative approaches in combination with biofeedback with a team of healthcare professionals in order to best address the patient’s goals and limitations. In treating functional fecal incontinence in pediatrics, the therapist will best find success in utilizing behavioral modification in conjunction with biofeedback and referring to other providers such as physicians and nurse practitioners to provide standard medical therapies. As with any method of intervention, the therapist should place high priority on establishing rapport with the patient and patient’s network of support [19]. The administration of biofeedback by a physical therapist provides a viable, non-invasive treatment for the pediatric population that experiences dysfunctional voiding and functional fecal incontinence.
Conclusion
The current systematic review on BBD focused on the treatment of dysfunctional voiding and functional fecal incontinence with biofeedback. Through analysis of articles that were collected, the authors concluded that biofeedback is a beneficial treatment for children with dysfunctional voiding and functional fecal incontinence. More conclusive research needs to be completed to explore the effects of biofeedback therapy treatment in order to make more concrete conclusions.
Footnotes
Conflict of interest
The authors have no conflict of interest to report.