
Abstract
PURPOSE:
This study aims to evaluate the effectiveness of a prefabricated carbon-composite ankle foot orthoses (c-AFOs) on gait parameters in children with unilateral spastic cerebral palsy (USCP) exhibiting a drop foot pattern.
METHODS:
Sixteen ambulatory children with USCP and a drop foot pattern were included (mean age: 9 years; gross motor function classification system: I
RESULTS:
Effects on the drop foot pattern were investigated while the children walked in shoes only. The shoes already increased the maximum ankle dorsiflexion in swing (
CONCLUSION:
Investigated c-AFOs are beneficial for improving drop foot patterns in children with USCP. Significant effects on pathological barefoot pattern were already achieved with the child’s regular shoes. This could be considered in clinical decision processes. In comparison to shoe walking, c-AFO additionally improved foot clearance and normalized initial heel contact. The third rocker deteriorates with the c-AFO. Since kinematics improved with the orthoses during swing and early stance phase, c-AFOs might reduce tripping and falling caused by a drop foot during long distance walking.
Background
One of the main impairments in children with cerebral palsy (CP) is a disturbed development of movement and posture [1]. Abnormal muscle tone, loss of selective motor control and reduced balance may arise due to the underlying non-progressive brain lesion [2] and affect walking ability in more than 70% of children with CP [3]. The restricted motor function can limit activity and participation in society [4]; therefore effective walking is an important goal in rehabilitation processes [5].
The ankle is described as the most affected joint in the lower extremity in ambulatory children with CP [6]. Especially in children with unilateral spastic CP (USCP), diminished dorsiflexion during swing or excessive plantarflexion during stance are the most common gait impairments [7]. Both patterns disturb normal walking and important gait prerequisites like foot clearance, stance stability and adequate step length [2]. Missing dorsiflexion during swing is classified by Winter et al. as Type I gait pattern in children with USCP and is called drop foot pattern [8]. In this gait pattern, normal ankle movement during swing phase from plantarflexion into dorsiflexion is reduced and toe clearance may be limited [8]. Several intervention strategies like gait training, ankle foot orthosis (AFO) or surgery procedures exist to restore disturbed gait prerequisites caused by the drop foot [9, 10, 11].
AFOs are frequently prescribed to either increase or maintain the range of ankle dorsiflexion and/or improve functional gait impairments [12]. Previous reviews investigating AFO effectiveness suggested positive effects on gait kinematics, kinetics and time-distance parameters [5, 13]. However, a consistent conclusion of results is difficult, since different AFO types and study designs were utilized as well as information on prescription protocols, AFO goals or patients functional status was limited [5, 13, 14].
Different materials like plastic or carbon are used to construct AFOs. The material properties of carbon (high tensile strength, high stiffness, elasticity, low mass) make carbon ideal for the construction of AFOs since it has the advantage of resisting dynamic stress while simultaneously having less weight than conventional polymer AFOs. This suggests that dynamic walking is supported more efficiently due to the energy recovery properties of carbon composites [15, 16]. Therefore, carbon composite AFOs (c-AFOs) are widely used to improve the efficacy of gait by preventing a drop foot during swing, limiting excessive plantarflexion during stance and supporting the push-off mechanics during pre-swing [15, 17, 18]. Customized AFOs with carbon components were investigated in patients with cerebral palsy and myelomeningocele and showed promising results regarding foot clearance, improvement of first foot contact and higher ankle power generation in contrast to posterior leaf spring or a hinged AFO made out of plastic [15, 16, 19]. Limited knowledge exists on prefabricated spring-like c-AFOs with layers of carbon fibers in children with USCP. The aim of this prospective study was to evaluate the effectiveness of prefabricated carbon-composite orthoses in children with USCP exhibiting a drop foot pattern on different gait parameters in comparison to barefoot and shoe walking.
Methods
Participants
Sixteen children with USCP were recruited in the area of south-east Germany. Inclusion criteria were unilateral spastic CP, age between 4 and 17 years, ambulatory without walking aids and drop foot pattern. We classified the drop foot with two different clinical presentations which had to be observed during visual gait analysis: forefoot/plantigrade first foot contact and missing observable dorsiflexion during mid-swing. Exclusion criteria were previous surgery of the lower extremity or surgery that could affect walking ability in the past twelve months, botulinum toxin injections in the lower extremity in the past six months, spasticity of the lower extremity
All subjects were informed about the goals and the process of this study. Parents and children gave their informed consent. The study was approved by the local ethics committee of the Technical University Munich, Germany (Vote: 5867/13) and carried out according to the latest version of the Declaration of Helsinki.
Material
The investigated prefabricated c-AFOs are made out of layers of carbon fiber, kevlar and fiberglass (manufactured by CAMP Scandinavia, provided from BASKO Healthcare). The orthoses contain an insole with a semi-rigid full length foot plate with fore foot rocker, a lateral extension without articulating elements and a ventral attachment (Fig. 1a). The lateral extension is perpendicular to the footplate. Although the c-AFO has no hinge, sagittal ankle movement during stance phase is permitted due to the flexibility of the material composition. For older children and adolescents, the c-AFO is named ToeOFF
Individual patient characteristics and clinical examination
Individual patient characteristics and clinical examination
GMFCS: Gross motor function classification system; PF: plantarflexion; DF: dorsiflexion; MAS: Modified Ashworth Scale; passive DF measured with knee extension and neutral position of subtalar joint using a goniometer; strength measured with manual muscle test; parameters of involved side only for: MAS PF, strength dorsiflexors, passive DF.
ToeOFF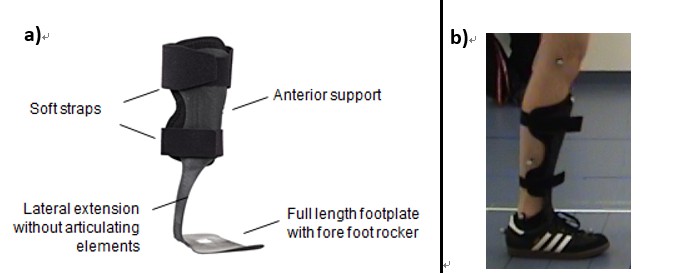
Participants were prospectively analyzed during three randomly assigned conditions; (1) barefoot, (2) walking in shoes, and (3) walking in shoes with orthosis. Prior to three-dimensional gait analysis, anthropometric parameters were measured and adapted for each condition. For the PluginGait marker set, heel and toe markers had to be placed on the child’s shoe for the shod conditions (Fig. 1b). Markers were placed as close as visually and tangibly possible to the correct anatomical position. Positions of the markers were not changed between shod conditions. A resting period between walking trials was given according to the patient’s needs. Since most children wore the orthosis for the first time, they started walking with the c-AFO prior to data collection to get familiar with the orthosis. Familiarization with the c-AFO was specified by achieving individual comfort and a homogenous gait pattern. The individual familiarization time varied between one and ten minutes.
Children walked at a self-selected speed on a nine meter straight walkway. Vicon motion capture system with six infrared cameras was used for gait analysis (VICON, Oxford Metrics, Oxford UK). Two embedded force plates captured kinetics (AMTI, Advanced Mechanical Technology Inc., Watertown, MA, USA). Vicon Nexus (1.8.2) was used to define gait cycles and to calculate spatio-temporal parameters, kinematics and kinetic data. Data were further processed with custom made Matlab (Mathworks R2013b) routines.
Data analysis
The primary outcome was the ankle dorsiflexion in swing. Further outcomes contained ankle/foot, knee and hip kinematics during stance, ankle power and ankle moment during late stance, time-distance parameters and overall gait impairment, measured with the Gait Profile Score (GPS) [21]. The GPS is a global gait deviation index. It consists of nine kinematic parameters, which can be analyzed separately with the Gait Variable Score (GVS). Lower GPS and GVS values reflect a walking pattern closer to normative data, while higher scores reflect a more pathological gait pattern [21].
Mean and standard deviation (SD) of kinematics, kinetics and time-distance parameters of the involved side for all separate conditions with group comparison
Mean and standard deviation (SD) of kinematics, kinetics and time-distance parameters of the involved side for all separate conditions with group comparison
DF: dorsiflexion; PF: plantarflexion; deg: degree; max: maximum; min: minimum; W/kg: watts per kilogram; Nm/kg: newton meter per kilogram; m/s: meter per second; steps/m: steps per meter; m: meter;
Gait cycles were subdivided into swing and stance phase. The stance phase was additionally split into loading response (first double support phase: after initial contact until contralateral foot off), single support, mid-stance (first 50% of single support), terminal stance (last 50% of single support) and pre-swing (second double support phase: after single support, before swing phase). These subdivisions were used to investigate gait phase specific outcomes. For the evaluation of the first rocker, movement at the ankle during loading response was analyzed by calculating the differences between the angle of the ankle at initial contact and the ankle angle at the end of the first double support phase. Values less than zero indicate ankle movement from dorsiflexion towards plantarflexion or less dorsiflexion. For the calculation of the GPS and GVS, we used the method described by Baker et al. and published normative data [22, 23].
Three walking trials with valid kinematic and kinetic data of each patient and walking condition were used for statistical analyses [24].
Statistical analyses were computed with SPSS (IBM SPSS Inc., Chicago, IL, USA, version 21). Mean values and standard deviations for each condition were calculated for the kinematic, kinetic and time-distance parameters. For GPS and GVS, median and interquartile range was used to describe the change in gait impairment. The Friedman test was applied to examine statistical differences. In case of significant main effects, post-hoc Wilcoxon signed-rank test was conducted between each pair of conditions resulting in three paired groups (1. barefoot vs. shoe; 2. barefoot vs. orthosis; 3. shoe vs. orthosis). The Bonferroni procedure was used to avoid accumulation of alpha errors. The corrected significance level was set to
The whole testing protocol took 90 to 120 minutes per child including physical examination and gait analysis with three walking conditions. To obtain three walking trials with valid force plate contacts, 5 to 20 trials were performed in each condition.
Patient characteristics and results of clinical examination are listed in Table 1. Four of the patients already used the c-AFO in daily routine. The remaining patients wore the c-AFO for the first time during the study. Mann-Whitney test revealed no significant differences of any parameter during the c-AFO condition between these subgroups (
Ankle
A Friedman test revealed statistically significant differences for all tested ankle parameters (Table 2). A post-hoc test showed significant differences for maximum and mean dorsiflexion in swing between each pair of conditions (
Knee
The Friedman test showed statistical significant differences for knee angle at initial contact, for minimum, maximum, and mean knee angle during single support as well as for knee angle at the end of terminal stance (end of single support). Compared to barefoot walking, a post-hoc Wilcoxon test revealed a better knee extension at initial contact when wearing shoes (
Individual differences between shoe and c-AFO walking
Individual differences between shoe and c-AFO walking
Differences calculated by subtracting values derived with shoes from the values derived with the c-AFO (c-AFO-shoe). Positive values indicate movement in the direction of: dorsiflexion, knee flexion, hip flexion. Negative values indicate movement in the direction of: plantarflexion, knee extension, hip extension; all kinematic differences in degrees (
Compared to barefoot walking, cadence decreased when the children walked in shoes with a further decrease when wearing the c-AFO (
Kinematic traces during gait cycle of Gait Variable Score parameters. Graphs of Gait Variable Score parameters of all separate conditions; mean values of joint kinematics over 100% gait cycle averaged across all investigated patients; involved leg only. Solid black line: barefoot condition; dashed black line: shoe condition; dotted black line: AFO condition; grey: norm references with band of standard deviation. Ant/Pst: anterior/posterior; Int/Ext: internal/external rotation; Flex/Ext: flexion/extension; Add/Abd: adduction/abduction; Dor/Pla: dorsiflexion/plantarflexion.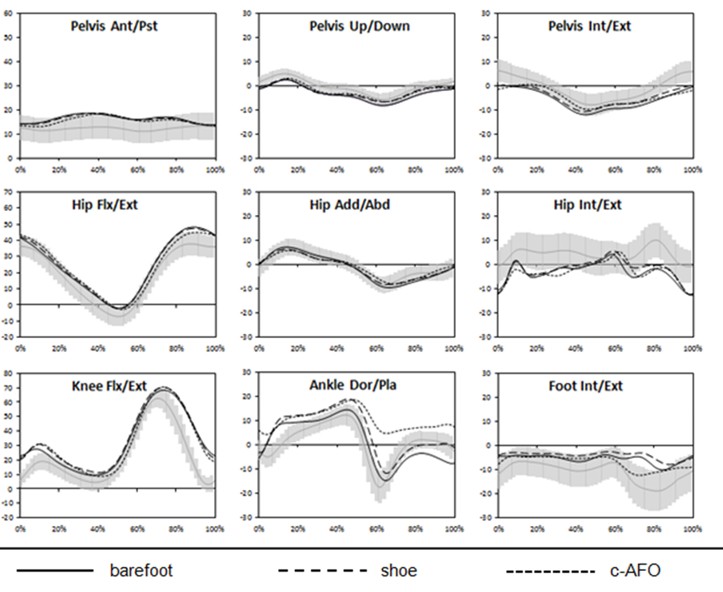
The Friedman test revealed no differences in overall gait impairment measured with the GPS between barefoot and shoe walking or between shoe and c-AFO walking (Table 4). In the GVS, only two parameters changed between the investigated conditions. Ankle parameter of the involved side increased when wearing the c-AFO as compared to the barefoot condition (
Discussion
Wearing the investigated prefabricated carbon-com- posite AFO improved foot clearance during the swing phase of the gait cycle and led to an improvement of first heel contact in children with USCP. Our results demonstrate that the drop foot pattern of children with USCP already diminished while wearing regular shoes. Especially the measured dorsiflexion during swing phase improved when wearing shoes. This had a slight positive effect on the following initial contact. While the ankle dorsiflexion did not change with shoes during initial contact, the sole angle improved slightly at this point of the gait cycle. The initiated changes at the ankle in swing and early stance phase by wearing shoes were even more pronounced when wearing the c-AFO. Moreover, ankle dorsiflexion at initial contact improved and the sole angle further ameliorated by wearing the c-AFO compared to the shoe condition. This led to an improvement of ankle motion during loading response. Apart from knee extension at the end of terminal stance phase, none of the observed changes at the knee or ankle joint during single support when wearing shoes were further modified by wearing the c-AFO. With shoes, the children walked in a slightly increased flexion at the ankle and the knee during single support. These changes may be induced by the shoes’ heel sole differential of one centimeter or the used wedge [25]. During mid stance, the only parameter which changed with the c-AFO was an improved sole angle. These changes may point towards a delayed heel rise in single support or less heel rise in mid-stance. This, in turn, may indicate slightly more stability during second rocker because of a larger contact surface. Improved knee extension at the end of terminal stance was the only parameter at the knee modified by the c-AFO. While wearing shoes had no effect on plantarflexion or kinetics at the ankle during late stance, the c-AFO hindered the movement into plantarflexion and the measured maximal ankle push-off power significantly.
Gait profile score and gait variable score of the involved side for all separate conditions with group comparison
Gait profile score and gait variable score of the involved side for all separate conditions with group comparison
GPS: gait profile score; GVS: gait variable score; IQR: interquartile range.
Other studies evaluating the effectiveness of different types of AFOs (e.g. hinged, solid, plastic, carbon AFOs) showed comparable results regarding an increase in dorsiflexion during swing [16, 19, 26] and improvement of first rocker [16, 19, 27]. Desloovere et al. and van Gestel et al. investigated the gait of children with USCP using c-AFOs [16, 19]. In both studies, the ankle angle at initial contact and dorsiflexion in swing increased. In these studies, the c-AFOs caused an improvement of first and second ankle rocker. Compared to their barefoot condition, the ankle power generation during third rocker significantly decreased when wearing the c-AFO [16, 19] but showed no significant difference compared to shoe walking [19]. The c-AFOs used in our study significantly reduced the maximum power generation compared to the barefoot and the shoe condition (Table 2). Differences of power reduction between the aforementioned studies and our results may be caused by the use of different types of carbon AFOs (dual carbon fiber spring AFOs), differences in walking speed (increased speed vs. stable speed) or by an extra tuning of the c-AFOs as performed in the other studies [16, 19].
A decrease in hip extension or decreased knee extension with less gastrocnemius stretching during late stance may be a contributing factor to a reduced power generation while wearing the c-AFO. Because most children showed an excursion towards hip and knee extension during late stance with the c-AFO (Table 3), the absence of ankle motion into plantarflexion during pre-swing which is hindered by c-AFO stiffness may be the main deteriorating factor of 3rd rocker. Given that the power is calculated by joint moment multiplied by angular velocity and angular velocity is limited when the movement is restricted, an AFO which limits the motion into plantarflexion by simultaneously not changing ankle torque reduces the amount of power generation at the ankle [18].
Carbon orthoses are suggested to absorb energy during early stance and return it later on to assist ankle push-off power [15, 18]. This mechanical assistance may have the impact to reduce the demands on calf muscles, which is why patients with weakness or easily fatigable plantarflexors could increase their walking distance or walking durations with a c-AFO [18]. The mechanical assistance might be of special interest in patients with spinal cord injury, myelomeningocele or poliomyelitis who have extremely low plantarflexor strength or paralysis of that muscle group. A reduced power generation at late stance may lead to a decrease in gastrocnemius muscle activity and could further decrease muscle strength with prolonged c-AFO use. This was already shown in studies investigating muscle activity when using solid or hinged AFOs [28, 29].
Individual c-AFO tuning processes were not applied because standard function of the prefabricated c-AFO should be evaluated. Modifications to alter shank kinematics in stance are important considerations in clinical practice [30]. Our results indicate significant changes of ankle and knee kinematics by wearing only shoes with a heel sole differential of one centimeter or a used wedge. Hence, further individual shoe adjustment may already be of clinical relevance to improve gait function for children with USCP. Differences regarding shoes’ sole thickness, sole or shoe stiffness or heel width of the individual shoes may have additional effects which should be considered and may lead to differences in c-AFO response.
The used c-AFOs caused no improvement in overall gait impairment measured with the GPS. The foot rotation parameter of the GVS improves with the c-AFO but the GVS of the involved ankle increased with the c-AFOs compared to the barefoot condition. GVS deviation at the ankle from normative values when the child walked with the c-AFO may be explained by overcorrections at the ankle during swing and the reduced range of ankle motion into plantarflexion during late stance (Fig. 2, ankle graph). While functional events like foot clearance in swing or first heel contact at the ankle improved with the c-AFO, the overall deviation from normative data (measured with the GPS) did not change. This highlights the question whether the use of a movement restriction of AFO is required for those children whose primary gait deviation is a decreased dorsiflexion during swing, as classified as Type I by Winter and colleagues [8]. Other aids which manipulate only the swing phase could be more beneficial for normalizing global gait indices and ankle GVS by simultaneously improving functional events limited by the drop foot.
The measured ankle angles in this study cannot be used to describe exact values at the ankle when wearing shoes or the c-AFO. We used the same marker protocol for all conditions, after which the toe marker is placed on the second metatarsal head or close as possible to that landmark on top of the shoe. The heel marker is placed on the same height as the toe marker. Together with the tibia markers, a 90 degree angle of the ankle is processed. The placement of toe and heel marker on the shoe may lead to measurement errors in the shod conditions regarding true ankle dorsiflexion because of the shoes heel sole differential or the used wedge. While the ankle angle differences between barefoot and the shod conditions may be affected by this procedure, the comparison of the ankle angle differences of the shoe and c-AFO condition may approximately reflect the real kinematic change caused by the orthoses.
Furthermore, shoes modified the time-distance parameters to a greater extent than the c-AFO. Improvements in time-distance parameters are the most reported response of AFO use in the literature [5, 13, 16, 19, 24, 26, 27]. However, the c-AFOs investigated in this study demonstrated changes in cadence but no differences in walking speed or stride length compared to shoe walking. The children walked with a speed of 1.19 m/s and with a stride length of 1.15 m in shoes, which is close to normative values of a healthy reference population of our gait laboratory (norm: walking speed
Because of individual capacity or fatigue during investigation, resting time was given according to individual need. Persistent fatigue as a potential confounding factor was controlled via randomization of walking conditions. Individual c-AFO adaption times were allowed to consider possible heterogeneity in adaption capability to ensure a comfortable gait pattern. This may be a meaningful method for evaluating immediate effects whereas further gait pattern change due to longer c-AFO adaption periods cannot be ruled out. The comparison of the included subgroups of patients who already used the c-AFO in daily routine and those who wore the orthosis for the first time presented no significant differences in any of the investigated parameters. This is in line with previously published results showing that there were no significant differences of gait kinematics, kinetics, or time-distance parameters when children with CP walked with a newly prescribed orthosis directly after delivery or after four weeks [31]. Because of the different CP populations investigated [31] and our small subgroups (4 vs 12), further investigations are needed to elucidate the detailed mechanisms of how c-AFOs may affect the gait of children with CP after a longer adaption time.
Future studies are needed to compare the effectiveness of the investigated c-AFOs with other dynamic carbon-component AFOs or with orthoses or aids with the same functional goal. Likewise, the present study may provide preliminary evidence of c-AFOs in children with USCP as a precondition for larger prospective, longitudinal studies investigating possible functional and social benefits (e.g. less stumble, higher walking distances, and improved participation) that may be achieved by the kinematic changes.
The investigated prefabricated carbon-component AFOs improved the drop foot pattern in children with USCP. Significant effects on the pathological barefoot pattern were already observed at the ankle and knee while the children walked in their regular shoes. Consequently, clinical decision processes should include the individual effect of the child’s shoes on walking pattern. In comparison to shoe walking, the c-AFO additionally improved foot clearance and normalized initial heel contact. The power generation at the ankle during push-off deteriorates with the c-AFO because of reduced motion into plantarflexion during third rocker. This may lead to muscle weakening. Everyday wearing for longer periods should be recommended with caution for this population. Because of the positive effects of the c-AFO on the drop foot pattern in children with USCP, the investigated c-AFOs may be used primarily for long distance walking and in case of frequent stumble and falls due to reduced ankle dorsiflexion in swing.
Footnotes
Acknowledgments
The Technical University of Munich received financial support from CAMP Scandinavia and the D.H. Heijne Foundation. The investigated orthoses were donated by BASKO Healthcare for study purposes. The funders were not involved in study design, data collection, data analysis, or decisions in submitting the manuscript for publication. We would like to thank Dr. Alexandra Heidsieck, Munich School of Bioengineering (MSB), Technical University of Munich for proofreading of the final version of the manuscript and all participants and their parents for participation in the study.
Conflict of interest
None to report.