
Abstract
PURPOSE:
To evaluate variables that modulate pain during intramuscular botulinum toxin A injections in children.
METHODS:
As part of a Quality Improvement project, this retrospective analysis compared
reported pain during and five minutes post injections with patient and procedural
variables using subgroup and regression analyses (
RESULTS:
Mean procedural pain for all procedures (
CONCLUSION:
Age, topical anesthesia, and injected region impact procedural pain and in nearly 96% of cases, patients report mild or no pain within five minutes. Additional research into these predictors is necessary, but short-lived procedural pain may suggest that frequent use of sedation/anesthesia is unnecessary.
Introduction
Since the initial report of successful use in 1993, intramuscular botulinum toxin injections have become common and effective procedures for management of limb and axial spasticity in children [1]. The typical therapeutic effect of the botulinum toxin A (BoNT-A) is 3–6 months, therefore patients often undergo repeated procedures [2]. Clinical practice includes wide variations of injection style, procedural sedation/general anesthesia (which carries risks for increased morbidity and adds cost), topical anesthetic, and distraction techniques [3, 4, 5, 6]. No information is published analyzing the impact that procedural factors have on pain in this population. The goal of this retrospective analysis was to identify factors that could be targeted to reduce procedural pain as part of a larger quality improvement project.
Methods
A retrospective chart review was conducted of patients who received BoNT-A
injections during a two-and-a-half-year period between 2014 and 2016
(
Average and median pain ratings during the procedure and post-procedure were
calculated. In addition, changes in pain between during- and post- procedures were examined.
Pre-existing differences in pain ratings and age between subgroups of patients were compared
using t-tests (alpha
Exploratory regression models were calculated to determine potential predictors
of pain, which included age, repeat procedure, presence of Child Life, use of either
vapo-coolant spray or topical lidocaine/prilocaine cream, number of injection sites and
region(s) of the body injected (leg, thigh, arm, hand and axial). Pain during the procedure
was treated as a continuous variable and a multiple linear regression was conducted [7]. Pain was further classified as absent (rating of
0), mild (ratings of 1–3), moderate (ratings 4–7) and severe (ratings 8–10) [8, 9].
Post-procedural pain scores were dichotomized into pain (any score
Results
All procedures undergoing final analysis (
Patient demographics and procedural characteristics
Patient demographics and procedural characteristics
Procedural pain ratings were reported in the moderate range for 33% of cases and
severe for 12% of cases (Fig. 1).
However, the vast majority of children had either no pain (83.8%) or mild pain (12.1%) five
minutes after the procedure. For all procedures, mean pain during the procedure was 3.8 (sd
Procedural pain ratings across intervention subgroups
Change in pain ratings following injection. Distribution of pain ratings during and
post-procedure. Graphs B-D represent the distribution of post-procedure pain for each
respective subgroup of absent, mild, moderate, and severe procedural pain.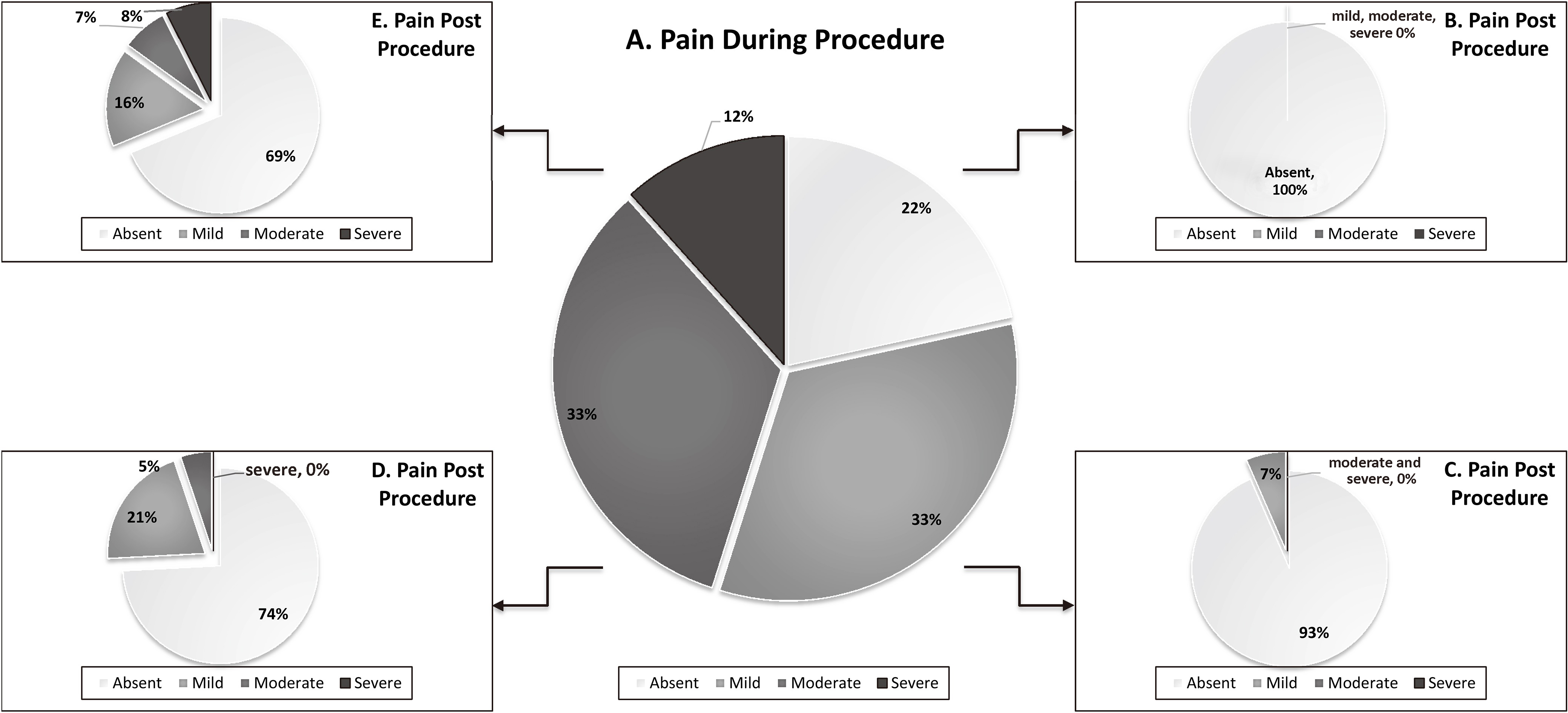
Regression analyses of procedural pain ratings at both time points are shown in
Table 3. The model explained about 64% of overall
variance in pain scores. Injections into the leg, thigh and hand were positively associated
with procedural pain, as was the use of any topical anesthetic. Age was negatively related
such that reports of pain were lower among older children. A logistic regression was
performed to determine significant predictors of the likelihood of post-procedural pain (no
pain versus any pain
Factors predicting pain during and after BoNT-A injections
Intramuscular botulinum toxin A injections have been shown to be effective at
reducing muscular tone, which is commonly utilized to improve function, range of motion,
positioning, and hygiene in patients with spasticity [10]. Peri-procedural pain ratings are a simplification of a broader experience
that also includes efficacy, anxiety, and guardian satisfaction [11]. Minimization of pain is important because pain with injection
has been shown to impact discontinuation of the intervention [12]. This study demonstrated that without the use of general
anesthesia, inhaled sedation, or enteral sedation, the vast majority of patients (roughly
84%) were pain free with only 4% reporting greater than mild pain at five minutes. This data
set is similar to unpublished data from an alternate institution, in which 98% of a small
cohort (
Two modifiable risk factors, topical anesthetic use and utilization of Child Life specialists for distraction, were examined because they are both potential means for improving patient experience. Distraction was associated with lower post-procedural pain scores. However, it is likely that clinical selection bias and age as a confounder limited the ability to draw impactful conclusions. This selection bias was clinically observed as a tendency to utilize more “pain relieving” and distraction techniques in children known to have a greater expression of pain. This bias may explain, in part, the finding that any topical anesthetic use was associated with significantly higher procedural pain ratings. A prospective, randomized evaluation of patients receiving sham versus topical anesthetics would provide more definitive information regarding the impact of topical anesthetics in this population. The patients’ novel versus repeat procedure status was not associated with changes in pain ratings in this population, which is not aligned with research in pediatric cancer patients demonstrating a potentiation of pain during subsequent visits [13]. The results of the exploratory regressions suggest that receiving injections in the leg, thigh, and hand were more painful for children than arm or axial sites. Therefore, pain reducing interventions may be more useful for those children.
Another potential limitation of the study was the inability to analyze differences between parent proxy and patient pain ratings. Younger children may have a higher frequency of proxy reports and as such, this limitation may have impacted the findings that showed an association between increased age and less procedural pain but increased likelihood of post-procedure pain. It has been shown that when using numerical scales, parents tend to assign higher pain ratings than children report [14]. Observational tools minimize the variance of patient vs. parent/guardian proxy ratings and have been shown to be a reliable and valid measure in children with cognitive impairment [15]. Anxiety may have a stronger impact on younger children’s procedural pain response. Resolution of the anxiety following the procedure could explain more complete resolution of pain than in older children. It would be useful to thoroughly examine anxiety states pre- and during- procedure in this population as it has been shown to be highly correlated to the experience of pain in children without disability [16, 17].
Conclusion
Pain was reported as absent or mild shortly after the procedure in at least 95% of cases. Exploratory findings suggest that younger age, use of any topical anesthetic, and location of injections significantly increase acute pain during a procedure. Acute pain during the procedure and older age increase the presence of pain 5 minutes after the procedure. Any efforts to improve patient experience should address short term pain reduction. Further exploration of these variables is required to reduce morbidity, avoid unnecessary costs, and determine ideal pain-relief practices.
Footnotes
Conflict of interest
The authors have no conflicts of interest to report.