
Abstract
BACKGROUND:
There is evidence that channelopathies are the cause of many different neurological diseases. The epileptic perinatal encephalopathy due to mutation in the KCNQ2 gene is a rare disease involving severe tetraparesis and cerebral visual impairment. Diseases of this kind are associated with severe disability that involves multiple systems and requires accurate genetic diagnosis and early multidisciplinary care once clinical stability is reached.
CASE REPORT:
We describe a case of a baby girl with KCNQ2 encephalopathy who came to our observation for rehabilitation at age 2 years and 6 months.
CLINICAL REHABILITATION IMPACT:
We stress the importance of a correct clinical, pharmacological and visual diagnosis. Correct diagnosis made it possible to involve the baby girl and her care-giver in an early process of visual rehabilitation lasting 6 months, the effects of which proved to persist at follow-up after more than a year, making it possible to start a useful inter-professional rehabilitation plan.
Keywords
Introduction
There is much evidence that channelopathies are the cause of many different neurological diseases. These can manifest in different ways, involving the central, peripheral and somatic nervous systems, and have major functional impact [1]. KCNQ2 encephalopathy (decrease in potassium-dependent ion channels) is a rare disease requiring accurate genetic diagnosis [2]. When associated with drug-resistant epilepsy [3] it requires correct pharmacological therapy to obtain good control of seizures and therefore a high level of observation and collaboration to enable good multidisciplinary care and integrated rehabilitation. In cases of cerebral visual impairment, it is important to conduct visual assessment and early orthoptic rehabilitation in the framework of a complex rehabilitation plan. From an early stage of development, the visual system is the preferential channel for integrating perceptual experience and relating to the world. The term cerebral visual impairment is used here in the sense of impairment of visual function due to retrogeniculate functional injury in the absence of eye disease [4]. It is often associated with other motor and cognitive disabilities and is the most frequent cause of visual deficit in children of western countries, where its incidence is increasing. Severe impact on motor, cognitive and behavioural development requires early diagnosis to determine residual visual potential in these young patients, optimise its use and reduce disability, thus favouring the learning of adaptive strategies to achieve the best possible quality of life for the infant and family.
Case report
The baby girl of Caucasian race, second child of healthy parents, was born at 40 weeks by spontaneous vaginal delivery after an uneventful pregnancy. At birth the baby showed cyanosis and low vigour and required cardiopulmonary intensive care/resuscitation; APGAR 1’ 7; 5’ 9; weight 3170 g, length 55 cm, CC 36 cm. In the first hours a critical episode with perioral cyanosis extending to head and trunk was recorded together with laryngeal stridor. Phenobarbital therapy was administered to treat repeated critical episodes characterised by hyperactivity with crying, stridor, cyanosis and opisthotonos associated with EEG series showing discontinuous activity, multifocal anomalies with burst suppression pattern and multifocal intercritical paroxysmal anomalies. Topiramate and multivitamin therapy (pyridoxine) were subsequently added due to incomplete response of myoclonic seizures. Array CGH analysis showed significant genomic anomalies; normal 46: XX karyotype. Cranial MRI initially showed absence of focal lesions in the posterior cranial fossa and supratentorial region, besides patent dural sinuses and normal ventricular complex. Subsequent MRI (28/2/2013) showed slight hyperintensity of the pallidal nuclei in T2-weighted images. Plasma but not CSF concentrations of lactose were elevated (3049 mg/dl); plasma and CSF concentrations of alanine and biotinidase were normal; CSF amino acids and neurotransmitters were normal; palmityl-protein thioesterase was normal. Topiramate assay was 4.9 mg/L (n.v. 2.0–2.5). The CTSD gene was mutation-free.
Phenobarbital was gradually tapered as daytime wakefulness/alertness improved,
while therapy was continued with topiramate 15 mg twice a day, calcium levofolinate
pentahydrate 2–4 mg twice a day, biotin 5 mg twice a day, lansoprazole 15 mg 1/2 capsule per
day, pyridoxine chlorohydrate 300 mg 1/4 capsule per day, thiamine
The patient came to our observation at age 2 years and 6 months. Examination showed laryngomalacia and compression of the trachea by the innominate artery with recurrent episodes of stridor, dysphagia and feeding difficulty (limited to small amounts of blended food 100 ml/day). Feeding was usually in half-seated position with frequent regurgitation. Neurological examination showed overall developmental delay: communication prerequisites such as rotation of eyes and head towards sound or speech, attempts at eye contact, recognition of persons, possible proto communicative exchange with therapist, recognition of routine, response to stimulus with attempts to move hands and feet, and vocalisation were present. Eye examination showed the anterior segments normal with lenses in situ, and fundus oculi without significant abnormalities. Also present were bilateral photomotor reflex, alternating exotropia, convergence spasms, fixation and pursuit deficit. While saccadic movements could not be evoked, VOR (ocular vestibular reflex) and VEP were normal. Severe hypotonic tetraparesis with unreliable head and trunk control was present. Poor and repetitive spontaneous motility of the four limbs, good muscle trophism, absence of spasticity and clonus were observed. Rolling to the right with assistance was seen, while crawling was absent, and walking was not possible. The patient was being treated with topiramate 15 mg 1 capsule twice a day and lansoprazole 7.5 ml. Visual evoked potentials were within normal limits. EEG showed multifocal anomalies with partial organisation of brain electrical activity. Genetic testing was recently confirmed positive for KCNQ2 gene mutation.
(a): LEA grating acuity test; (b): LEA T.0. 0.25 CPCM initial treatment; (c): 0.5
CPCM: LEA intermediate phase; (d): 2.0 CPCM: LEA intermediate phase; (e): LEA T.1. 8.0
CPCM final treatment.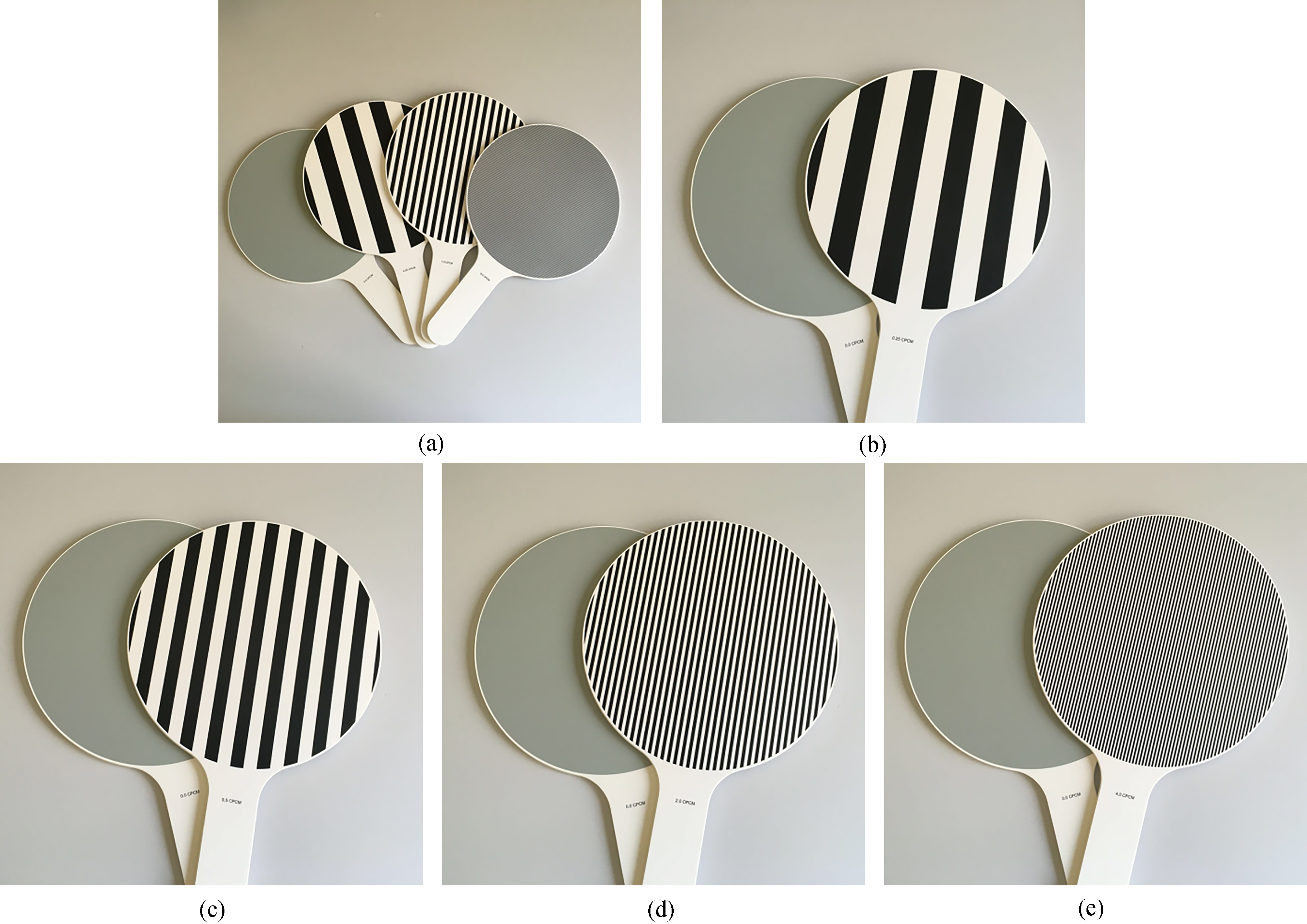
The neuromotor rehabilitation plan for the patient included physiotherapy twice
a week for 6 months (setting: supine, prone, sitting with and without anterior table, on
side, long-sitting, transition from supine to sitting by rolling on sides) aimed at
increasing proximal, girdle and trunk musculature and improving axial stability. Static
verticalisation in prone position with ankle-foot orthosis braces to increase
antigravitational recruitment. A wheelchair with postural system favouring realignment of
head and trunk enabled the patient to increase from 7/20 to 9/20 on the Sitting Assessment
Scale-SAS [5]. Refractive correction under
atropine cycloplegia (
The perceptual component measured by the LEA grating acuity test [6] (Fig. 1) was initially 0 and 8.0 cycles per cm (CPCM) of
surface at discharge. The stimulation of pursuit eye movements and saccades by showing
objects in a sequential and systematic manner (target at an initial angular distance of
15
Visual skills inventory questionnaire
Visual improvement after constant use of optical correction enabled the child to progress from a facilitating work setting (darkness with luminous/ dissociating target) to a setting with normal light, first with a black and white and then with a high-contrast colour target with complex perception characteristics. Fixation improved considerably since the child became able to fixate objects of interest and to maintain stable gaze. This had a positive effect on the whole rehabilitation programme and on mother-daughter relationship.
The visual system is a preferential channel for integrating the various perceptions of daily life in the real world. Hand-eye coordination, postural control and walking all require the mediation of visual perception. Also the sleep-wake cycle and relationships with the mother and other family members are mediated by visual function. The visual cortex of mammals is not completely developed at birth. This is why environmental stimulation is needed in the first months of life to complete its structural maturation. Certain studies have shown that growing up in an enriched environment influences development of the visual system in rats, activating the central nervous system and especially visual plasticity [9]. A multisensory approach (visual-auditory-tactile) in an enriched environment involving for example a black and white checkerboard, soft toys of different colours and tactile consistency, black and white or coloured objects of different shapes, size and consistency, coloured lights and so forth plays a fundamental role in activating brain plasticity, especially in early infancy [10].
Providing a correct posture system allowed good alignment of the trunk, and corrective lenses enabled targeted and personalised orthoptic rehabilitation. Last but not least, the good mother-daughter relationship and constant training of the care-giver were important, enabling the infant to be correctly stimulated on a daily basis and helping her to explore her surroundings by providing structured material agreed upon by the rehabilitation team. The domestic environment was also modified with appropriate lighting.
Conclusion
Our rehabilitation plan became possible and productive when the infant’s waking state improved after suspension of phenobarbital and after control of epileptic seizures, once correct diagnosis had been achieved, the correct dose of topiramate found [11] and infections (largely respiratory) reduced. Only the improvement of visual-perceptual skills of the baby girl made it possible to develop a useful inter-professional, integrated rehabilitation plan aimed at promoting the best possible quality of life and participation for the baby and her family, despite the severity of the cerebral palsy [12].
Footnotes
Conflict of interest
No potential conflict of interest was reported by the authors.