
Abstract
This pilot study compared a Nintendo Wii intervention to single-joint resistance training
for the upper limb in children ages 7 to 12 with spastic hemiplegic cerebral palsy (CP).
Children were randomized to Wii training (
Keywords
Introduction
Cerebral palsy (CP) refers to a range of childhood syndromes of posture and motor impairment, that arise as a result of a static (non-progressive) lesion in the developing brain [1]. It is the most common cause of physical disability in children, with a prevalence of 2 to 2.5 per 1000 live births in Western countries [2]. It is associated with a variety of other medical conditions, including intellectual disabilities, epilepsy, speech, language and communication delays, visual and sensory impairments, feeding difficulties, and also the co-occurrence of other disabilities [3]. There are several sub-types of CP, one of which is spastic hemiplegic CP, which occurs in approximately 23% of children with spastic CP [4]. Spastic hemiplegic CP involves unilateral static lesions in regions of the brain associated with upper limb movement [3] and is associated with motor impairments, including range of motion restrictions [4], fine motor coordination deficits [5], disrupted sensory mechanisms [6], and muscle weakness [7]. Motor impairments have a significant impact on upper limb function in children with spastic hemiplegic CP [8, 9] and can severely compromise a child’s ability to perform upper limb functions such as reaching, grasping, and manipulating objects, or performing activities of daily living, such as eating, dressing, and bathing [10].
Conventional approaches to the management of spastic hemiplegic CP involve medical, surgical or rehabilitative strategies [11]. With respect to rehabilitation, options typically include physiotherapy, occupational therapy, constraint-induced movement therapy, hand-arm bimanual training, or resistance training [12]. However, systematic reviews have proven largely inconclusive as to which rehabilitative approaches are superior for children with upper limb impairments, and under which conditions, intensities and durations they are most effective [13, 14, 15]. Furthermore, there is not as much emphasis in the published literature on comparisons between different rehabilitation strategies, particularly in the home environment [11, 13, 15, 16].
The importance of motivation in therapy, especially for children, is an area of study that has been somewhat neglected in the scientific literature for this population. Studies show that children with CP have significantly lower levels of motivation related to the mastery of tasks when compared to children of typical development [17, 18]. Lower levels of motivation can adversely affect a child’s functional abilities and potential, and decrease the effectiveness of therapeutic intervention. Motivation is a critical element of pediatric rehabilitation [17], and has been identified by physiotherapists as the single most influential personal characteristic that determines motor and functional outcomes in physiotherapy [19]. Therefore, improving motivation may ultimately be one of the most meaningful ways to improve compliance, and actualize the goals of treatments for clinical populations such as children with CP.
One novel approach to rehabilitation that has the potential to address the need for motivating, home-based therapy for children is the use of virtual reality (VR) training. The Nintendo Wii is a subset of VR technologies known as active video games, which are games that require physical activity beyond that of conventional hand-held controller games [20]. With respect to pediatric CP, the Wii has been studied in domains such as exercise intensity, balance, postural control and muscle activation patterns [21, 22, 23, 24]. Several studies which focus on Wii training for the upper limbs in children with CP [25, 26, 27] report positive clinical and functional outcomes that warrant further investigation. Furthermore, the ability of VR technologies to promote motivation in therapy is also supported by research into motivation theory. For instance, Ryan et al. [28] utilize self-determination theory (SDT), outlined by Deci and Ryan [29], to argue that VR incorporates the main factors needed to promote intrinsic motivation related to the mastery of tasks. These main factors are autonomy of the player, feelings of competence when playing, and a sense of immersion in the task [30]. Furthermore, the use of VR technologies may align well with the mandate of recreational therapy, as VR devices such as the Wii are primarily designed for leisure [31]. Moreover, some theorists, such as Datillo et al. [32], use SDT as a framework for therapeutic recreation service delivery. Based on these features, it is therefore possible for the Nintendo Wii to be intrinsically motivating to participants, which can be harnessed for rehabilitation in order to increase motor and functional outcomes for clinical populations such as children with CP.
By contrast to Wii training, resistance training is a more conventional approach to rehabilitation of children with spastic hemiplegic CP [12]. Resistance training, which is also referred to as strength training in the literature pertaining to children with CP [30], is a relatively well studied therapeutic approach for children and adolescents with CP [7, 12] designed to increase the strength and endurance of targeted muscles groups [33]. Several studies which focus on upper limb resistance training in this population [34, 35, 36, 37] all report positive clinical and functional results that are in line with the conclusions of several systematic reviews [16, 38].
The present pilot study compared a Nintendo Wii intervention to single-joint resistance training for the upper-limbs for children with spastic hemiplegic CP. The aim was to explore the differences between a more novel approach to rehabilitation, such as the Wii, to a more conventional therapy in the home environment. Therefore Wii training was considered to be our experimental group, and resistance training was the control. Our first objective was to determine whether there were any improvements in the upper limb function after a Nintendo Wii intervention, and whether these benefits were comparable to that of single-joint resistance training. Our second objective was to explore differences in compliance rates, motivation levels and intervention feasibility, for parents and participants. Overall, we predicted positive functional outcomes in Wii training, along with higher motivation levels and compliance rates in Wii training.
Methods
Study design
This pilot study employed a pre-test, post-test experimental design, with
a 4 week follow up, and a non-equivalent control group. Participants were recruited from
the client database at a children’s treatment centre in Ontario, Canada. Children between
the ages of 7 to 12 with a diagnosis of spastic hemiplegic CP, were contacted by letter or
phone call, and invited to participate in the study. Exclusion criteria for the study was
any surgeries in the upper extremities in the past year, medical complications or
cognitive impairments that made exercise unsafe or impossible, regular, weekly play of the
Nintendo Wii, and/or the game used in the study, and/or regular participation in
resistance training interventions for the upper-limbs. Participants were recruited and
assigned to each group in the order that they contacted the researchers. The researchers
and participants were not blinded to group assignment. A total of
Intervention
Participants assigned to Wii training were given a Nintendo Wii U system, one Wii MotionPlus Remote controller, one Wii Nunchuck, and the Wii Sports Resort game, to be played at home. Participants were instructed to play their choice of games, out of a specific set of games in Wii Sports Resort approved by the researchers to promote higher upper-limb activity, as compared to other games. The approved games were: tennis, archery, swordplay, basketball, bowling, canoeing, golf and Frisbee. Participants were instructed to play the Wii using their affected (spastic) hand for at least 40 minutes each day, 5 days a week for 6 weeks (30 days). No adaptions were made to the Wii-mote for any participants. Participants assigned to resistance training were given one TheraBand hand-held ball weight, one Elite brand resistance band, and one gel filled squeeze ball. The ball weights were of 0.5, 1 or 1.5-kilogram sizes, and the resistance bands were of light or medium tension. The size of the ball weight and resistance band tension was based on the parent’s perception of the child’s initial strength and ability level at the beginning of the study, after the child tested all weights and bands under the supervision of the researcher and assistants. Participants were then given a series of 6 exercises to do at home, at an intensity of 12 repetitions per exercises, for two sets (i.e. corresponding to 24 repetitions for each exercise), 5 days a week, for 6 weeks. These exercises were: bicep curls with resistance bands, triceps extensions with hand-held weights, grip strength with squeeze ball, shoulder flexion with hand-held weight, shoulder abduction, with resistance bands, shoulder extension, with resistance bands. Each exercise was demonstrated to participants and their parents, and participants were given a booklet, consisting of pictures and written instructions on how to do each exercise. It was approximated that 12 repetitions would take the child approximately 3 to 4 minutes to complete, for a total of 36 to 48 minutes per day of exercise. Thus, the overall time commitment and intensity level of exercise between the Wii and Resistance groups is considered to be comparable for the purposes of this study.
In both groups parents supervised the exercise sessions and recorded the time of day, duration and games or exercises completed in a daily logbook. Parents were also asked to encourage the child to use their spastic hand as much as possible, and recorded how much they used their spastic hand in the daily logbook. Parents in the Wii group were also asked to ensure that the child attempted to mimic the real-life motions of the Wii game as much as possible (i.e. if playing tennis, to swing the remote like a tennis racquet, etc.)
Outcome measures
Demographic information
Parents were asked to report their child’s overall level of functioning according to the Manual Ability Classification System (MACS) [39], and the Gross Motor Function Classification System (GMFCS) [40]. Parents were also asked to report botulinum- neurotoxin-A (boNT-A) dosage for their child, both 6 months before and during the study, and this information was verified by the developmental pediatrician at the children’s treatment centre with the consent of all parents and participants in the study.
Participant characteristics
Participant characteristics
To quantify upper limb quality of movement and functional ability, the Melbourne Assessment of Unilateral Upper Limb Function-2 (Melbourne-2), the ABILHAND-Kids questionnaire and average maximal grip strength in the spastic and non-spastic hand were assessed at pre, post and 4 week follow-up. The Melbourne-2 is a criterion-referenced test that divides 14 test items that involve reaching, grasping, releasing and manipulating objects into 4 categories of movement. These categories are range of motion, accuracy, dexterity and fluency. A score for each of these categories is generated, which is then combined and converted into a total percentage score, where the higher the percentage, the higher the child’s level of functioning [41]. The ABILHAND-Kids questionnaire is a parent reported measure that rates the child’s level of difficulty, as perceived by the parents, in completing a list of 21 tasks in daily life that require the use of the upper limbs. The raw score is then transformed into a linear measure, known as the logit, according to the Rasch model of analysis [42]. Finally, maximal hand-grip strength was measured in the affected (spastic) hand of all participants, using a baseline pneumatic (squeeze bulb) dynamometer, with a range of 0 to 15 pounds per square inch (psi) units. Participants were seated with shoulders in neutral position, and elbow flexion at 90 degrees. They were instructed to squeeze the bulb as hard as they could for 2 seconds, and the highest value attained was recorded. Two successive measurements were taken on each hand, with an approximately 10 second rest period between measures.
Compliance and parent feedback questionnaire
Compliance, motivation, and feasibility of each intervention for
parents and participants were also assessed at post-test. The daily logs were used to
determine participant compliance with the study’s protocol. In the logs, participants
were asked to state the date and time of their daily exercise; as well as the duration
of the exercise for the Wii training group, and the number of repetitions completed each
day for the resistance training group. For 100% compliance, the Wii training group was
required to complete 1200 minutes of exercise over the intervention period (40 minutes
In addition, the daily logs for both the Wii and resistance training groups asked the participants to directly respond each day to the following questions: 1. How much did you use your affected arm today? 2. How hard did you exercise today? and 3. Did you have fun exercising today? The children were asked to respond to these questions on a 6-point Likert scale, which is displayed in Fig. 2.
Finally, a parent feedback questionnaire was used to assess motivation and feasibility of the intervention, as perceived by parents. Parents were asked to rate their responses to a series of 4 questions. These questions and possible responses are displayed in Table 3.
Statistical analysis
Descriptive statistics were used to represent and compare trends in the experimental and non-equivalent control group.
Upper limb functional assessment scores
Upper limb functional assessment scores
Parent feedback form rate responses
Demographic information
Table 1 displays participant demographic information for all participants in the study. All 6 were male, between the ages of 7 to 12. The MACS and GMFCS level of participants ranged from I to II, and one participant received boNT-A injections in the upper limb during the course of the study.
Intervention dosage compliance rate, by group, for each participant.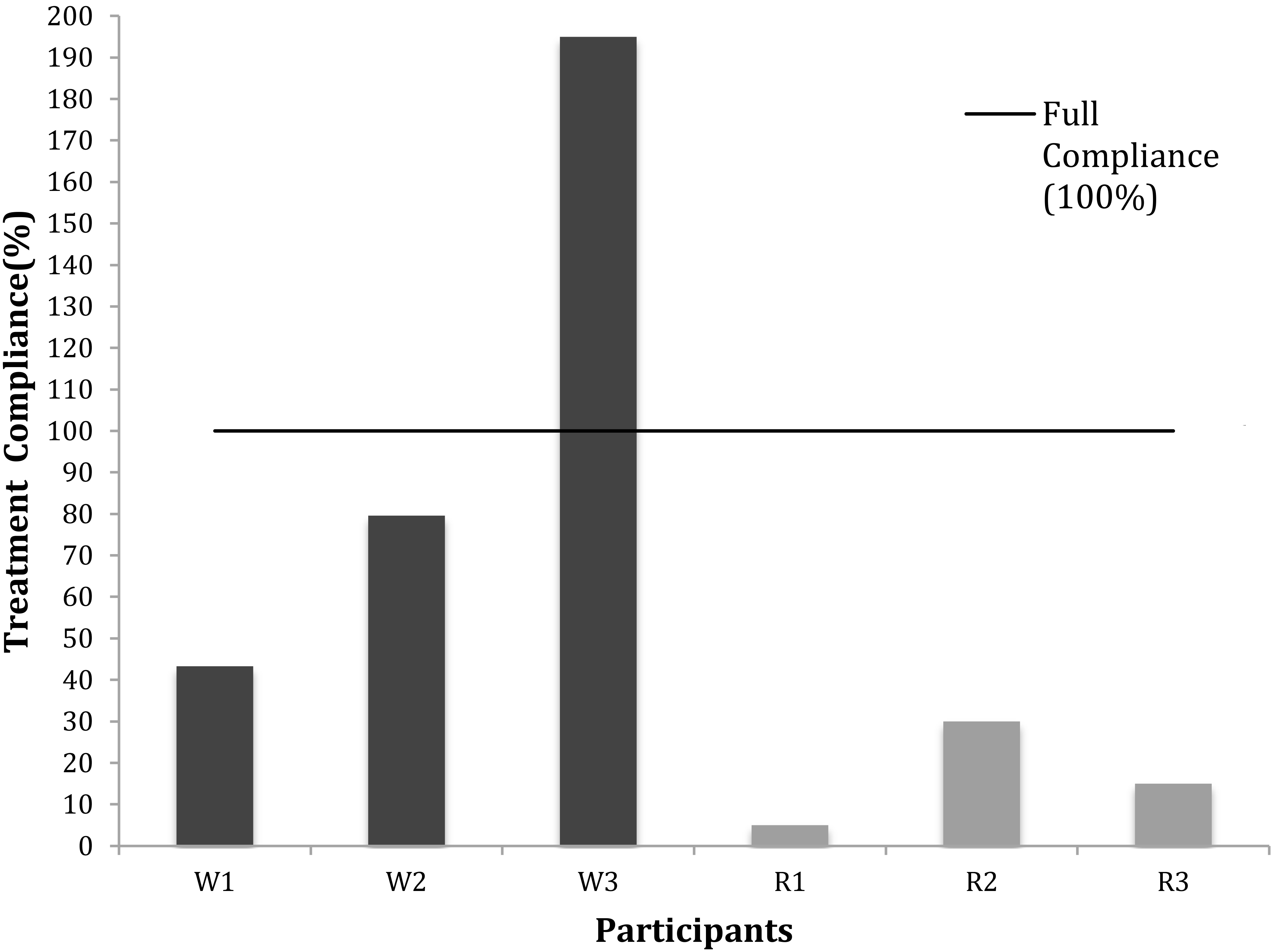
Child responses to daily log questions, by group and question.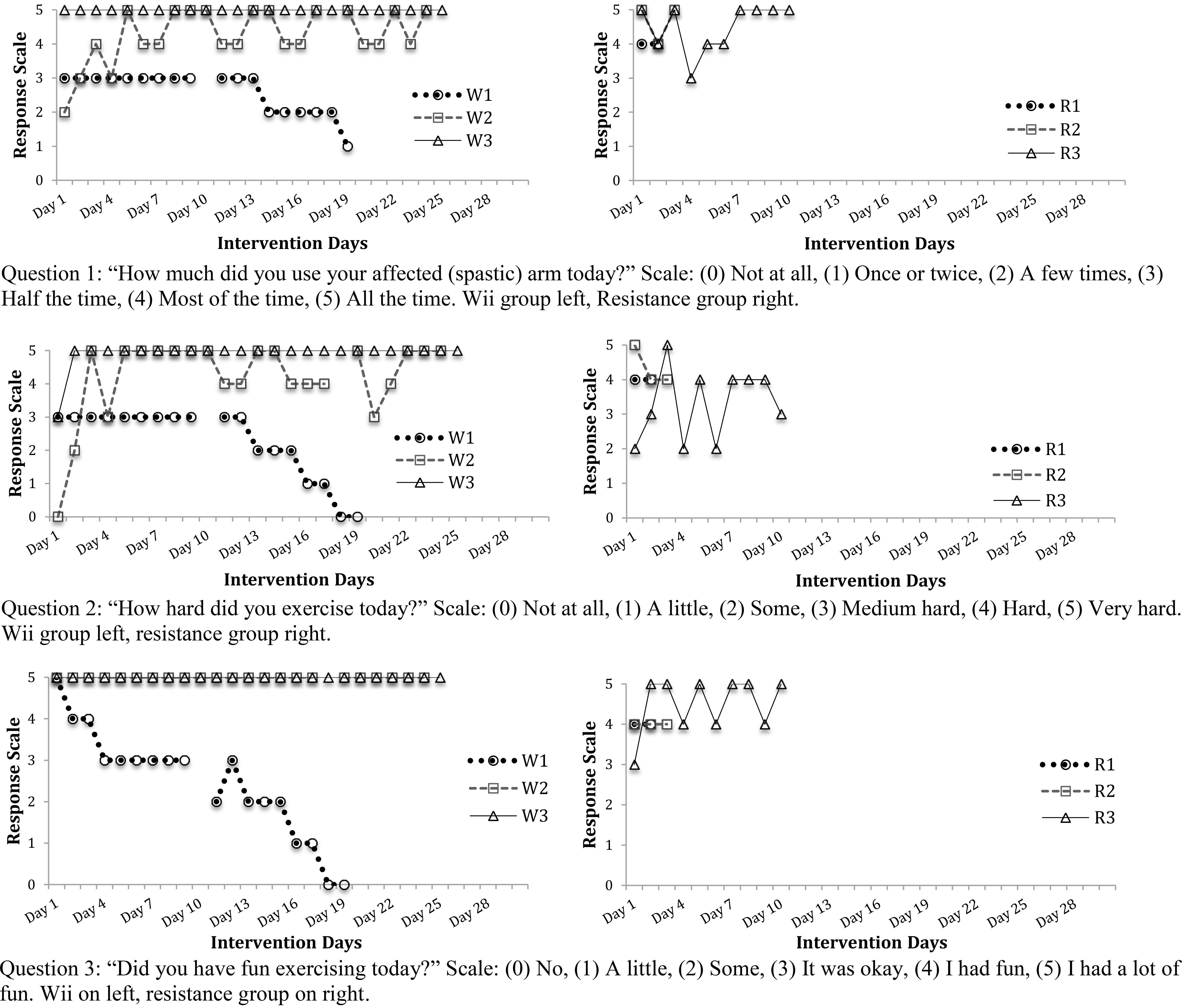
Table 2 displays the pre, post, follow-up and change score data for all participants, with respect to the Melbourne-2, ABILHAND-KIDS questionnaire, and maximal average grip strength in the affected hand. With respect to pre-follow-up change, for the Melbourne-2, the largest change from baseline was experienced by W3, and the smallest by R1; for the ABILHAND-Kids, the largest change was experienced by W2, and the smallest by W3; and for grip strength, the largest change was experienced by R3, and the smallest by R1.
Compliance and parent feedback questionnaire
Figure 1 displays the intervention compliance rate for participants in the Wii and resistance training groups. Overall, all participants in the Wii training group demonstrated a higher compliance rate than the most compliant resistance participant. Figure 2 displays the results from the daily log questions that the children were asked to respond to each day. Overall, trend lines for both groups were variable, and the Wii training group had a greater response rate to the questions. Table 3 displays the parent responses to the feedback form, where parents of participants in the Wii training group reported a more positive (higher) average response to all four questions asked. Parents of children in the Wii training group had a higher average positive response to all questions posed, regarding, motivation and feasibility.
Discussion
The primary objective of this pilot study was to explore whether there were any improvements in upper limb function after a Nintendo Wii intervention, and whether these benefits were comparable to that of single-joint resistance training. We hypothesized that there would be positive functional outcomes in the Wii training group. The results of this study suggest that there may be functional benefits to Wii training for this population, as Wii participants made some meaningful improvements on several outcome measures, that warrant further exploration and study.
For the Melbourne-2 (MA2), 3 participants improved from baseline to follow-up (Table 2). Two of these participants (W2, and W3) were in the Wii training group. W2 and W3 improved from baseline to follow-up, while W1 improved from baseline to post-test. Interestingly, W2 and W3 had lower scores on the Melbourne-2 at baseline, and were both a MACS and GMFCS level II (Table 1). This finding is in line with Winkels et al. [25], who found that children with CP with low Melbourne-2 scores at baseline showed greater improvements after a Wii intervention. Since a progressive level of optimal challenge is necessary for motor and functional improvements in exercise rehabilitation [43], it is possible that children with CP at MACS and/or GMFCS level I ( that is, higher levels of functionality), do not experience Wii training and/or the Wii Sports Resort game as challenging enough to facilitate functional improvements. Therefore, it is possible that Wii training may be most appropriate for children at lower levels of functionality (MACS/GMFCS II or higher), who might experience the games as challenging enough to elicit functional improvements. With respect to the control group, the resistance training group participant that made improvements on the MA2 from baseline (R2) was the only participant to undergo boNT-A injections in his upper limbs during the course of the study. The possible role and effects of boNT-A injections on resistance training, and Wii training should be explored in future research.
In the ABILHAND-Kids assessments, 3 participants improved from baseline to follow-up, and two of these were in the resistance training group. However, the improvements for all participants were minimal, and one participant, W3 experienced a deterioration score (Table 2). A decrease in some participant’s ABILHAND-Kids scores after a Wii intervention was also reported by Winkels et al. [25]. While it is possible that Wii upper-limb functional improvements (as measured by the MA2) do not translate into improvements in the performance of daily activities (as measured by the ABHILHAND-Kids questionnaire), it is also possible that the ABILHAND-Kids may not be a sensitive enough assessment tool to measure parent-perceived change over the study’s time span of 10 weeks. The question of whether Wii training, and also resistance training translates into daily-life improvements for children in this population should be a focus of future research and larger trials.
For maximal average grip strength, 3 participants improved from baseline to follow-up, and two of these were in the resistance training group. Positive improvements in W3, in his spastic hand, was an interesting finding as the Wii Sports Resort game does not include any games that primarily target strength. Grip strength has been found to be strongly correlated with total muscle strength in children and adolescents [44]. It is possible that the action of holding the limb suspended during arm movements, and squeezing the Wii Remote to press buttons was enough to elicit strength improvements in children with spastic hemiplegic CP, who are known to have a considerable degree of muscle weakness [3, 12]. Chiu, Ada and Lee [2] also reported a trend towards improvements in grip strength in their upper limb Wii intervention for children with CP. The possibility of Wii training leading to strength improvements in this population would be an interesting direction for further studies, as well as the strategic selection of active video games to address specific motor and/or rehabilitative goals.
The second objective of this pilot study was to explore differences in compliance rates, and motivation and feasibility, as perceived by parents in the feedback questionnaire. With respect to compliance, all participants in the Wii training group had higher compliance rate than the resistance participant with the highest compliance rate (Fig. 1). As the intervention dosage and time commitment was set to be comparable for each group, this high compliance rate experienced by the Wii training group is an encouraging finding, as non-compliance with treatment is one of the greatest barriers in effective rehabilitation [45]. Furthermore, this finding is in line with those of other Wii studies for children with CP, such as Chiu, Ada and Lee [27], who reported a 96% compliance rate for Wii training in their home-based study. The over-compliance of W3, who exceeded the intervention dosage by more than 95%, is a notable finding. While it is not known whether extreme exercise rates such as this are typical for Wii or VR interventions, it is possible that in this case, it was due to the personal idiosyncrasies and preferences of this participant. However, it is also possible that some other factor influenced this result, which was not controlled for in the study. For instance, the presence of a similar-aged sibling, with who W3 may have played the Wii, could have positively influenced W3’s compliance and enjoyment during the study, leading to higher compliance rates. Factors such as these should be controlled for and/or investigated in future studies.
The participant-response daily log response questions yield interesting findings with respect to Wii training, as they had a greater response rate to the questions. Question 1, concerning use of the spastic limb, and 2, concerning perceived participant exertion, are likely related, as the Wii participants who reported high to medium-high use of the spastic limb, also reported greater exertion throughout the course of the study (W2 andW3). Furthermore, with respect to participant enjoyment, captured in Question 3, the same Wii participants (W2 and W3) experienced constant and sustained levels of enjoyment over the study. This is especially notable, when taken with the results from the parent feedback form questionnaire, which reported that on average, Wii parents perceived that their children had more fun, were easier to motivate to do the study, and that the Wii was easier to integrate into their child’s daily schedule, Overall, it suggests that the links between study compliance and motivation, and how they compare to overall functional improvements in home-based VR interventions for children with cerebral palsy, is an interesting area of study that warrants further investigation in a larger study.
Ultimately, Wii and other forms of VR and active video game training in the home may represent a novel approach to rehabilitation for children with CP, which may have the ability to solicit higher compliance and motivation in participants to complete the prescribed exercise program. This hypothesis is supported by SDT, as applied to VR [28]. SDT, put forward by Deci and Ryan [29] posits that tasks which promote autonomy, feelings of competence and a sense of relatedness promote intrinsic motivation to complete a task [46]. As Ryan, Rigby and Przybylski [28] suggest, is likely that VR, technologies such as the Wii can address these parameters needed for intrinsic motivation. For instance, active video game VR technologies like the Wii typically provide a wide selection of games, and choices within those games, which provides players with a degree of autonomy, in how they exercise. Competence describes an optimal level of challenge (not to easy or too hard) that is needed to feel successful in a task, which VR can facilitate by providing a progressive level of difficulty in different video game levels or rounds. Finally, a sense of relatedness in the task is facilitated by the development of new technologies that can stimulate motion realism in the virtual world. Furthermore, Datillo, Kleiber and Williams (1998) service delivery model for therapeutic recreation proposes an interaction between self determination, intrinsic motivation, the perception of manageable challenge and the investment of attention, all of which endorse enjoyment and functional improvements [32]. As children with CP tend to have lower levels of motivation related to the mastery of tasks than children of typical development [17], it is necessary to address motivation when designing interventions for this population. Although there are clearly established benefits for resistance training in this population [7, 12] if participants do not comply with the training regimen, the functional benefits of resistance training will not be experienced by this population. Motivating interventions such as VR technologies should be investigated in more depth in the published literature, so as to promote greater functional outcomes and higher compliance rates with prescribed treatments.
Limitations
The primary limitation with this pilot study its small sample size, which was too low to run statistical analyses to determine group differences. This reduces our ability to draw detailed conclusions about the population of children with spastic hemiplegic cerebral palsy at large. Other limitations include the lack of a representative sample of children with spastic hemiplegic CP – in this study, all participants were male, which is not reflective of the 1.5 to 1, male to female distribution of CP [3], possible bias in group assignment, as participants that contacted us to participate in the study may share characteristics that make them unique from the target population, and the lack of a true control group that received a treatment as usual condition. It was also not possible for us to control for the effects of boNT-A, cognitive and/or co-occurring disabilities, the use of other AVGS consoles by participants, or their participation in other exercise programs during the course of the study. Another limitation is the inability of the daily intervention logs to capture the details of daily exercise, i.e. such as what individual exercises were done in resistance training, or the level and difficulty settings of each game played in the Nintendo Wii intervention. As there are very few valid and reliable clinical assessment tools to measure participant, or parent-perceived motivation levels in children with disabilities, it was not possible for us to use them in this study. Finally, researchers and participants in this study were not blind to group assignment, which may have introduced bias into the findings. However, despite these limitations, the results of this pilot study were able to explore differences between Wii and resistance training in a home setting for this population, and lay a foundation for future research in this area.
Conclusions
Overall, the findings of this pilot study suggest that upper-limb Wii training warrants further investigation as a home-based rehabilitation strategy for children with spastic hemiplegic cerebral palsy. Future research should focus on increased sample sizes, a more representative sample, randomization, a true control and exploring the effects of different combinations of intervention games, Wii remote adaptations, and exercise and intensity levels. This study is, to the best of our knowledge the first to compare the Nintendo Wii to single-joint resistance training in this population at the community level, and it is our hope that this study can be replicated by other community-based researchers and clinicians who are interested in affirming and/or expanding on its findings.
Footnotes
Acknowledgments
We would like to thank the Grandview Children’s Foundation in Ontario Canada, for their generous support for this research.
Conflict of interest
The authors have no conflicts of interest to report.