
Abstract
OBJECTIVE:
To investigate whether pre-operative Quantitative Sensory Testing (QST) can identify patients who experience persistent post-operative knee pain following Total Knee Replacement (TKR).
DATA SOURCES:
PubMed, EMBASE, CINAHL, EBSCO and grey literature.
STUDY SELECTION:
1056 studies were retrieved. The title and abstracts were screened by two independent reviewers, of which 45 were retrieved for full text analysis and 16 studies were included. Studies of any design were included if they recruited adults who underwent TKR; completed any component of the German Research Network on Neuropathic Pain QST or conditioned pain modulation testing preoperatively and assessed post-surgical joint pain using a self-reported outcome measure at a minimum of three months post TKR.
DATA EXTRACTION:
Data was independently extracted by two researchers. Disagreements were resolved through consensus. The extracted data was recorded in a predefined spreadsheet. Domains included demographic data, type and site of QST, pain outcome measure, follow up duration, statistical methods and associative data. Two independent reviewers assessed the quality of studies using Quality in Prognosis risk of bias tool and the certainty of evidence using the GRADE framework.
DATA SYNTHESIS:
Sixteen cohort studies met the eligibility criteria (n = 2051 patients). Data was analysed narratively because of the heterogeneity across the QST procedures (mechanical and thermal detection and pain thresholds, conditioned pain modulation and temporal summation of pain), measures of reporting pain (Western Ontario and McMaster Universities Osteoarthritis Index, visual analogue scale and numeric pain rating score) and follow up time points (3 to 18 months).
CONCLUSIONS:
Due to the heterogeneity and low-moderate quality studies included, it remains unclear whether QST can identify patients who are likely to experience persistent postoperative joint pain following TKR.
Introduction
In the United Kingdom (UK) National Health Service (NHS) the largest waiting lists are for people with bone and joint (orthopaedic) pain. As of January 2024, there are more than 800,000 people currently waiting to see an orthopaedic clinician, of which 45% have been waiting longer than 18-weeks [55]. One of the most common orthopaedic operations is a total knee replacement [56]. Around 110,000 total knee replacements are conducted each year in the NHS, primarily to treat knee arthritis, at a cost the NHS around £770 million each year for the NHS [57]. Projections from the National Joint Registry (2022) anticipate an increase of 36.6% in the number of TKR surgeries by the year 2060 [38]. The most common reason that individuals undergo a total knee replacement is pain relief. However, between 10– 34% of patients experience pain which persists beyond three months following their knee replacement, for which there is no evidence-based treatment. People who experience persistent pain following total knee replacement are more likely to be dissatisfied with the outcome of their surgery. At one year following surgery, 17% of patients, report that they regret their decision to have a knee replacement [38]. Therefore, around 20,000 people a year in the UK have a total knee replacement in the NHS that will not benefit them, at a cost of around £140 million [57].
In recent years, much research has been undertaken to understand whether it is possible to identify patients who are likely to experience poor outcomes following total knee replacement, prior to surgery. The results of this research have been inconsistent and not led to any significant changes to care pathways for people undergoing total knee replacement.
Quantitative Sensory Testing (QST) uses a group of non-invasive, quantifiable sensory stimuli procedures can provide insight into a person’s somatosensory nerve system function and integrity [3, 20]. Quantitative sensory testing quantifies these altered responses by utilising various stimuli to assess perceptions of proprioception, touch, pinprick/blunt pressure sensitivity, vibration, as well as sensitivity to heat or cold stimuli [3, 20]. It is suggested that people who may have altered nociceptive activity, may be more likely to experience persistent post-operative pain [20]. If QST is able to identify individuals who are likely to experience persistent post-operative pain following total knee replacement, it could significantly reduce the burden of unsuccessful surgeries on both individuals and society by improving patient selection for surgery and informing future intervention development. A recent systematic review suggested that QST may have the potential to identify patients, who are likely to develop persistent post-operative pain from orthopaedic surgery [20]. This systematic review aims to understand whether pre-operative QST can identify people who will experience persistent post-operative pain following total knee replacement.
Methods
This systematic review was reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Statement (PRISMA) [41].
Search strategy
A systematic search was performed of four databases (EMBASE, CINAHL, SCOPUS, PubMed) and grey literature on 29th March 2023 and updated on 30th January 2024 using a search strategy with components of quantitative sensory testing, persistent postoperative pain and total knee replacement. An example of the search strategy employed in the PubMed database can be found in Fig. 1. A manual search of reference lists of the acquired articles, along with relevant systematic reviews and meta-analyses was completed to identify studies that may not have been found through the initial search. No contact with expert authors in the field was attempted. After importing identified studies into EndNote X9 (Clarivate Analytics) and eliminating duplicates, a comprehensive assessment was carried out by the two researchers (V.K and G.F) blinded to reduce risk of bias and increase reliability. The titles and abstracts of the retrieved studies were scrutinised to determine inclusion. Finally, the full-text versions of the selected studies were obtained and analysed independently to assess their eligibility. Any differences that arose were resolved through consensus.
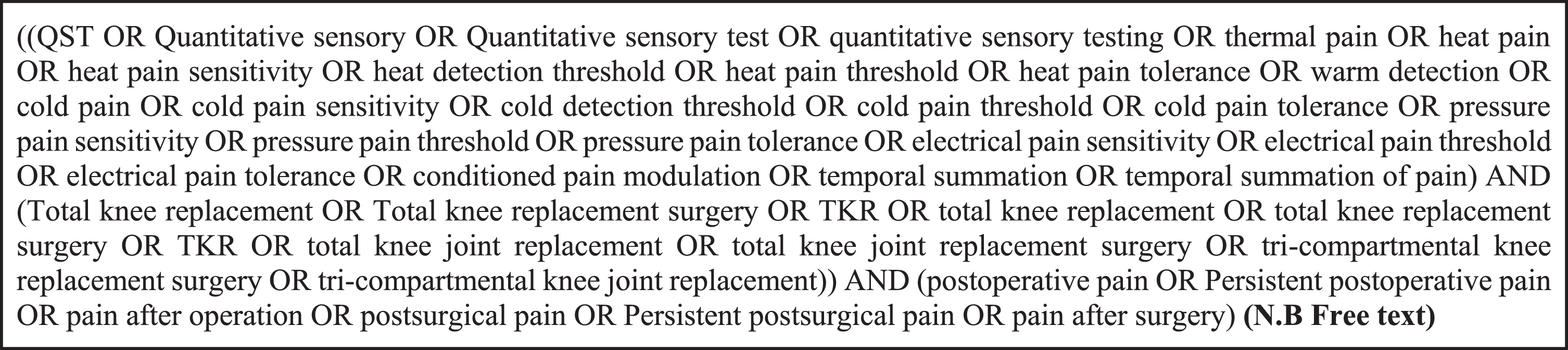
Pubmed search strategy.
Studies were included if they met all the following criteria: A study population of adults (aged 18 years and above) who underwent total knee replacement (TKR). Completed any component of the German Research Network on Neuropathic Pain (DFNS). Assessed post-surgical pain using a self-reported outcome measure at a minimum of 3 months after TKR (in accordance with the ICD-11 definition) [4]. Statistically associated or correlated preoperative QST and the above-stated pain outcome measure.
Studies were excluded if they met the following exclusion criteria: Animal or cadaveric studies. Commentaries, editorials, single case studies, reports or laboratory data, books or book chapters, letters, conference posters or proceedings or study protocols.
Assessment of methodological quality
The methodological quality of the included studies was assessed independently by 2 reviewers (V.K and G.F) using the Quality In Prognostic Studies (QUIPS) tool [42]. The QUIPS tool was deemed suitable since it is specifically aimed at assessing the risk of bias in studies investigating prognostic factors in line with the recommendations of the Cochrane Prognosis Methods Group [51]. This tool focuses on 6 domains that include study participation, study attrition, prognostic factor measurement, outcome measurement, study confounding, and statistical analysis and reporting with the final risk of bias of the study graded as low, moderate, or high.
Data extraction and synthesis
Data was independently extracted by two researchers (V.K and G.F). The extracted data was recorded in a predefined spreadsheet based on the works of previous research [19, 20] included bibliographical and demographic data, total number of participants, type and site of QST, pain outcome measure, follow up duration, the type of statistical method used to investigate association and its findings. Any disagreements that arose were resolved through consensus. Significant heterogeneity was observed in the administration of QST protocols and pain outcome measures employed among the individual studies. On performing the chi-square test of homogeneity test, an I2 value of 65% denoted substantial heterogeneity. Therefore, a meta-analysis was not recommended, and a narrative synthesis of the findings was performed.
Results
Study selection
The search strategy retrieved 1056 studies and three studies from the electronic databases and grey literature, respectively (Fig. 2). On removing 579 duplicates, the title and abstracts of the remaining 493 studies were screened, of which 45 were retrieved for full text analysis. Interrater reliability between the two reviewers was measured using a weighted Kappa statistic on a sample of included papers (n = 10). The agreement rate was deemed substantial (>90%)(k = 0.80). Sixteen studies met the inclusion criteria with the most common reasons for exclusion (29 studies) being: association of QST and chronic pain outcomes not analysed (45%), insufficient data (31%), revision replacement (17%) and change in pain reported as a measure (1%).
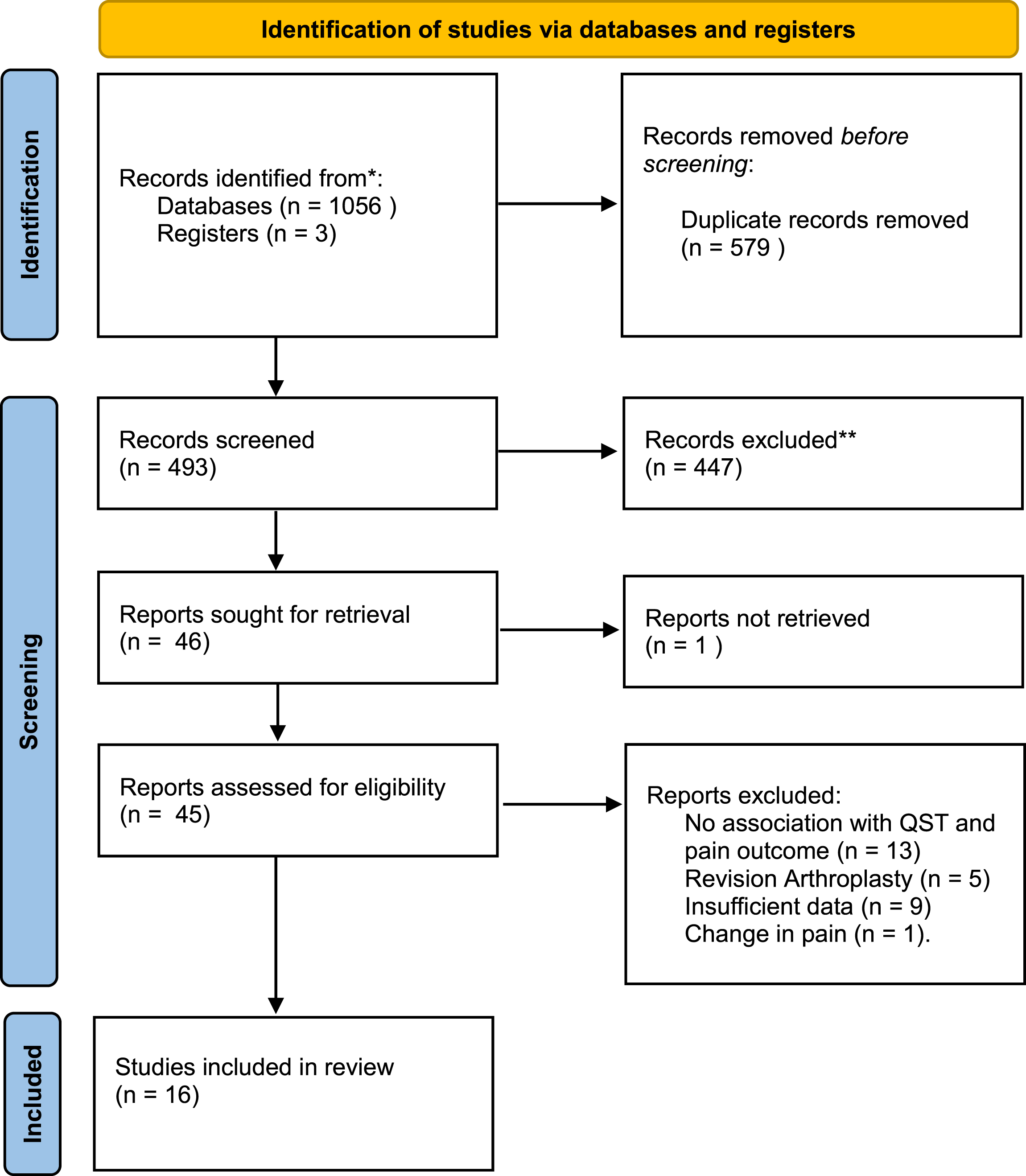
PRISMA flowchart.
This systematic review reports 16 studies, all of which were classified as prospective cohort studies. Most studies (n = 8) originated from Denmark [11, 31] and the United Kingdom [24, 43] and were published between the years 2007 to 2022. Table 3 demonstrates the characteristics of these included studies. The 16 studies sampled a total of 2051 patients who underwent primary unilateral TKR. Sample sizes ranged between 14 to 300 with a median of 128. The patients had a median age of 68 years, ranging from 62 to 73 years. All studies included in this analysis followed a longitudinal cohort design and investigated a population diagnosed with osteoarthritis. The majority of the participants were female, accounting for 60% (1231) of the total sample.
Preoperative QST assessment
Type of QST
This systematic review describes the utilisation of 14 QST modalities, including static modalities such as mechanical (three tests), thermal (six tests), and electrical (two tests), as well as dynamic (two tests). Mechanical QST was the most commonly reported test modality (12/16 studies), followed by dynamic measures (10/16 studies).
Test timing
Not all studies reported the timing at which preoperative QST was performed; those that did (four studies) reported times ranging from 57 (average), 17 (average) days to 1-2 weeks prior to surgery.
PPSP assessment
Outcomes
The most commonly reported outcome measures were validated questionnaires on pain and disability such as the Visual Analog Scale [8, 31] (seven studies), Western Ontario and McMaster Universities Osteoarthritis Index Pain sub-scale [23, 43] (six studies) and the Numerical Rating Scales [28, 44] (three studies).
Assessment timing
Only studies assessing postoperative pain at a minimum of 3 months following surgery were included, in accordance with the defined criteria for persistent postsurgical pain (PPSP) [4]. Pain assessments were conducted within a timeframe ranging from 3 months to 18 months following the total knee replacement surgery. The time period most frequently reported was 6 months [23, 44] (eight studies) followed by 12 months [11, 31] (six studies). Additionally, two studies reported time frames of 4 and 18 months [8, 28], respectively.
Preoperative QST association with PPSP
Mechanical
The assessment of mechanical quantitative sensory testing is commonly conducted using Frey filaments, whereas the determination of pain threshold is typically performed using blunt pin pricks and pressure cuffs [22]. Pressure pain threshold (PPT) was the most frequently administered test [11, 43] (11 studies) along with pressure tolerance threshold (PTT) and mechanical pain threshold (MPT) reported in three [26–28] and two [29, 30] studies respectively.
PPT
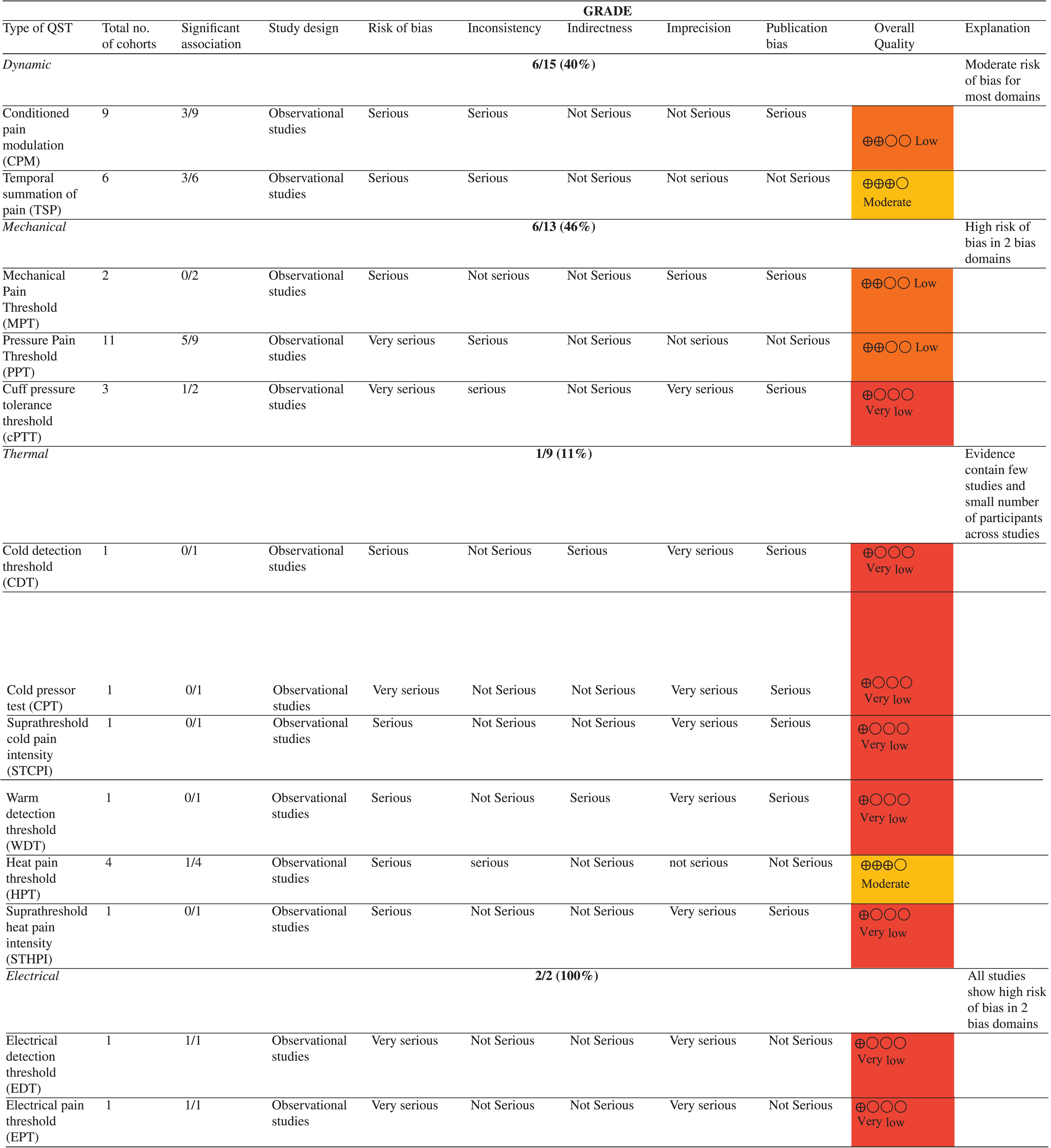
While 11 studies used PPT as part of their preoperative quantitative sensory testing protocol, seven studies [11, 43] provided data of its association with postoperative pain. Of these, only five studies [23– 25, 43] revealed statistically significant associations. Interestingly, Leung et al. (2019) [23] found PPT to be correlated to post operative pain at 12 months but not at 6 months. This was corroborated with the findings of Kurien et al. (2018) [24] and Wylde et al. (2015) [25] who found statistically significant associations with PPT when correlated with pain at 12 months. The overall quality of evidence for PPT within this review was judged to be low. Details of statistical associations are summarised in Table 4.
PTT
Three studies reported the use of PTT preoperatively [26–28]. Although, it should be noted that one of these studies did not investigate the relationship between PTT and pain [27]. Furthermore, out of the other two investigations [26, 28], only one was found to have achieved statistical significance. Petersen et al. (2016) [26] performed a regression analysis to ascertain the prediction of postoperative pain and found that at 12 months, PTT was an independent parameter for predicting persistent post-operative pain (R = – 0.222, P = 0.034). Overall, these inconsistencies contributed to the quality of evidence for PTT to be very low.
MPT
The results of both studies investigating the mechanical pain threshold at 4 and 6 months [29, 30] following surgery did not reveal any statistically significant associations with post-surgical pain. The quality of evidence was assessed as low as measured by GRADE.
Thermal
Thermal modalities of QST typically involve the application of heat or cold stimuli to the skin surface. This is commonly achieved by utilising Peltier elements (semiconductor junctions that create temperature gradient through electric current). Additional non-standardized techniques are also employed to cool or heat the skin, including the utilisation of radiant heat, ice application, or limb water immersion. Thermal modalities of QST were reported in 5/16 studies (31.25%).
Cold stimulus (CPT, CDT, STCPI)
No statistically significant correlations were reported for all three measures: cold detection threshold (CDT) [31] (R = 0.025, P > 0.05), cold pain tolerance (CPT) [32] (P = 0.84), suprathreshold cold pain intensity (STCPI) [29]. The quality of evidence for the only three studies [29, 32] that reported thermal QSTs was determined to be very low.
Heat stimulus (WDT, HPT, STHPI)
Heat pain threshold (HPT) was most commonly reported (four studies) [29– 31, 43] followed by warm detection threshold (WDT) (one study) [31] and suprathreshold heat pain intensity (STHPI) (one study) [29]. The quality of evidence for WDT and STHPI was judged to be very low. Although only 17% (1/6) of the studies reported a correlation with postoperative pain, the overall certainty of the evidence was rated as moderate.
Electrical
A study conducted by Lundblad et al. (2008) [8] is currently the sole study to investigate the electrical QST modalities in the context of chronic pain and post-total knee replacement outcomes. The study revealed a strong correlation between the electrical pain threshold (EPT) and electrical detection threshold (EDT) with pain at 18 months post TKR. The statistical analysis showed that the association was significant for both EDT (P = 0.045) and EPT (P = 0.012). Furthermore, the logistic regression model indicated that EPT was a strong predictor of pain (p = 0.01). The certainty of evidence was rated very low, primarily because of significant concerns in various domains such as imprecision. To improve the informational robustness, further studies involving a larger number of participantsare required.
Dynamic
Dynamic measures were the second most commonly reported QST modality in 10/16 studies (62.5%). The constituted measures such as Conditioned Pain Modulation (CPM) were utilised in 9/16 studies and Temporal Summation of Pain (TSP) in 6/16 studies.
CPM
Conditioned pain modulation was associated with chronic post-operative pain in only 3/9 (33%) studies [4, 28]. Vaegter et al. (2017) [28] and Durstler et al. (2021) [44] observed that preoperative CPM was found statistically significant at 6 months for postoperative pain, while Larsen et al. (2021) [27] reported this association at 12 months. Additionally, there was no standardisation of conditions in which test stimulus and conditioning stimulus were reported across all 9 studies. The overall quality of evidence for the use of CPM within this review was judged to be low.
TSP
TSP was found to be predictive of persistent post surgical pain in 3/6 studies (50%) at a minimum of 6 to 12 months post TKR [11, 31]. Kurien et al. (2018) [24] evaluated preoperative TSP with the use of cuff algometry and monofilaments. Although both methods correlated positively with post-operative pain at 6 months, the correlation between TSP elicited using monofilaments and post-operative pain was stronger. Petersen et al. found significant correlations between TSP and post-surgical pain at 12 months in both their initial study [11] (r = 0.24, P = 0.037) and a subsequent 3-year follow-up study [31] (r = 0.193, P = 0.013). In univariate linear regression analyses, they observed similar results with significant crude coefficients of 0.311 (P = 0.037) and significant P-values of 0.023, respectively. However, these associations were not found in the multivariate model. The remaining three studies [26, 35] did not find any association between TSP and post-surgical pain. Certainty of evidence for TSP was deemed moderate.
Risk of bias
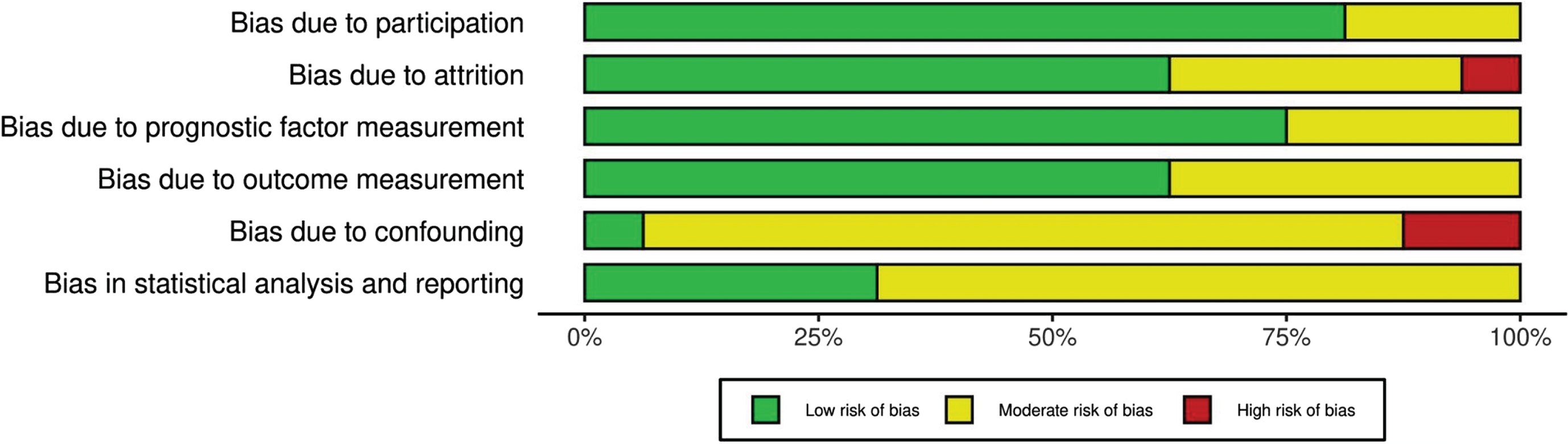
Overall, eight studies [11, 43] exhibited moderate bias, three were high [8, 28] and six [25, 44] were low. Cohen’s kappa was used to measure inter-rater reliability between the two reviewers in QUIPS bias evaluations with a result of 0.82 indicating a relatively high level of agreement. Disagreements in judgement were prevalent in the confounding factors domain, which consequently scored the highest risk out of the other domains as well, owing to most of the studies’ lack of clarity in describing confounding variables. These were subsequently resolved by consensus. Furthermore, the statistical analyses and reporting in the included studies were inconsistent, resulting in a moderate risk of bias within QUIP’s statistical analysis/reporting domain. Contrarily, the domains study participation and study attrition were judged to be of low risk of bias because of clear description of the population, transparent reporting of recruitment strategies and adequate accounting for participant losses to follow up. Although the use of standardised QST protocols such as the DFNS was not used in all the included studies, given the proven reliability and validity of assessment measures a low rating of risk was found in the prognostic and outcome measures domain. Individual risk of bias of the included studies can be found in Table 2 with the overall risk of bias of each domain demonstrated in Fig. 3.
QUIPS Tool (risk of bias for individual studies)
QUIPS Tool (risk of bias for individual studies)
Overall Risk of Bias.
Study Characteristics
Study Characteristics
(CPT) Cold pressor test, (CDT) Cold detection test, (CPM) Conditioned pain modulation, (cPTT) Cuff pressure tolerance threshold (EDT) Electrical detection threshold, (EPT) Electrical pain threshold, (HPT) Heat pain threshold, (MPT) Mechanical pain threshold, (PPT) Pressure pain threshold, (STHPI)Suprathreshold heat pain intensity (STCPI)Suprathreshold cold pain intensity, (TSP) Temporal summation of pain, (WDT) Warm detection threshold.
Statistical data on association
Summary of Findings
Previous systematic reviews have explored the relationship between presurgical QST and both acute and chronic post-surgical pain in total joint arthroplasties [19] and other surgeries [6]. However, this is the first systematic review to exclusively examine the relationship between presurgical QST and persistent post-surgical pain in patients who have undergone TKR. The current review is also the first to investigate which QST measures were most predictive of this relationship and aimed to evaluate the certainty of presenting evidence.
Among the 16 studies included a total of 13 QST measures were identified across four sub-types: mechanical, thermal, electrical, and dynamic. Given the variation in the timing of pain assessments, spanning from 3 to 18 months post-surgery, and the predominant use of non-standardized QST methods across most of the studies the evidence was narratively synthesised in this review.
In the current review, mechanical measures were the most reported (n = 12) wherein three measures— MPT, PPT and cPTT were utilised for preoperative QST. Among these measures, PPT seemed to demonstrate the most consistent correlation with persistent post-surgical pain (PPSP) in 5 out of 11 studies (45%). This percentage is lower compared to a recent systematic review [19], in which pressure stimuli were found to be correlated with post-surgical pain in 8 out of 12 studies (67%). These variations may be attributed to differences in the timing of pain onset and the inclusion of other joint arthroplasties within their study population. Furthermore, the selection of QST sites appears to influence pain outcomes, which may be inferred from the findings of one of the included studies, [43] revealing significant associations between PPT and PPSP in the forearm but not in the knee. The remaining measures, MPT and cPTT, yielded inconsistent results. MPT, in particular, demonstrated no significant correlation with PPSP, and the quality of evidence with regard to these findings was notably low.
The evidence for thermal QST presented conflicting findings overall. Among the three heat stimulus measures (WDT, HPT, STHPI), only 17% (1/6) of the studies reported a correlation with postoperative pain. The only study to demonstrate a positive correlation was specifically associated with the HPT measure, and the certainty of the evidence for it was rated as moderate, in contrast to the very low quality of evidence for WDT and STHPI. One study found no association between STHPI and persistent postsurgical pain (PPSP) [29]. However, a systematic review [15] has reported a strong correlation between STHPI and acute postsurgical pain in various surgeries such as total knee replacement [52], elective gynaecological surgeries, [14, 53] herniotomy, [54] and thoracic surgeries [10]. These discrepancies suggest that sensitivity to heat stimuli may indeed be dependent upon the timing of pain onset and type of surgery. Previous research has established that cold stimulus measures of thermal QST serve as strong predictors for neuropathic pain [45] and musculoskeletal disorders such as whiplash injuries [46]. However, within the context of postsurgical pain, our review examined three studies [29, 32] investigating cold stimulus measures (CPT, CDT and STCPI) found no significant correlations with PPSP in patients who underwent TKR with the quality of evidence supporting these correlations judged as very low. Interestingly, these results align with findings from three other reviews [6, 47], all of which failed to establish any meaningful association between cold stimuli and the development of PPSP.
Whilst only one study reported electrical QST measures, [8] utilising EPT and EDT, the study reported that lower EPT was associated with PPSP following TKR. Electrical QST measures have also demonstrated predictive value for surgical pain in procedures like caesarean sections, [49, 50] albeit primarily for acute postoperative pain. In the literature, while one study [16] suggested that electrical measures correlated more strongly with post-surgical pain compared to mechanical and thermal measures, recent systematic reviews have reported inconsistent associations with post-surgical pain. Notably, due to a high risk of bias related to study attrition, the quality of evidence was rated as low.
Dynamic measures were the second most frequently employed QST modality in 10 out of 16 studies. While conditioned pain modulation (CPM) showed an association with chronic post-operative pain in only 3 out of 9 studies (33%) [4, 28], the temporal summation of pain (TSP) emerged as a slightly more consistent predictor of persistent post-surgical pain, being found in 3 out of 6 studies (50%) [11, 31]. It should be noted that the limited association of CPM with persistent post-surgical pain aligns with findings from previous works [6, 19]. These findings were rated as having a very low quality of evidence, primarily due to the lack of standardisation in the conditions under which the test stimulus and conditioning stimulus were administered across all 9 studies. In contrast, the evidence supporting TSP was rated as moderate. Coupled with the clinical feasibility of administering TSP and its stronger association with persistent post-surgical pain, the moderate level of evidence makes it the most suitable QST measure among those reported in this review.
It’s crucial to highlight that certain confounding factors, such as gender, were not considered in the sixteen studies investigating the development of PPSP. This may be significant given that 60% of the participants (n = 1231) in this review were female. A meta-analysis [37] of postoperative pain predictors in TKR has shown that the female gender is moderately associated with increased postoperative pain severity. This suggests that gender may indeed be a confounding factor that influences both postoperative pain outcomes and preoperative pain sensitivity and should be taken into account when investigating their relationship with QST.
Our study offers several advantages compared to previous research. Unlike earlier reviews assessing the body of evidence for quantitative sensory testing (QST), our review employs tools that are well-suited for prognostic studies, such as QUIPS, and conducts GRADE assessments to evaluate the quality of evidence for each QST measure. However, it is important to consider certain limitations when interpreting the findings of this study. Firstly, administration of most QST measures relied on unstandardised protocols with a limited number of studies and small participant cohorts, potentially impacting generalizability and results. Additionally, significant heterogeneity existed in the statistical methods used; some studies employed univariate analyses while others utilised multivariate approaches, introducing challenges in result comparison. Moreover, some studies did not report p-values and other non-significant findings, reducing the transparency and reliability of results and resulting in a moderate to high risk of bias.
This systematic review was unable to establish an association between QST and PPSP based on and therefore are unable to make recommendations for clinical practice currently. However, the heterogeneity QST methods, and the poor quality of the research suggests that more needs to be done to standardise procedures and then test in a substantive cohort study. The aforementioned limitations substantially diminish the overall quality of evidence for the reported QST measures, resulting in a very low level of certainty of these recommendations. Despite the low level of evidence and confounding factors, preoperative QST screening holds promise for individual risk assessment of persistent postoperative pain due to its ability to differentiate between peripheral and central pain contributors [48]. The clinical implications of this review particularly concern patients with osteoarthritis undergoing TKR. The results provide a graded assessment of evidence quality, offering the potential to enhance clinician’s decision-making and cost-effectiveness in the adoption of QST. This would reduce the practical limitations of conducting a battery of preoperative tests, instead streamlining the process, allowing for earlier and more efficient identification of patients at risk of developing PPSP.
Conclusion
Despite the overall quality of evidence being very low, preoperative QST holds some potential for identifying patient pain profiles at risk of developing PPSP in the preoperative stage. Although mechanical and dynamic QSTs have been widely reported within pain literature, the findings of this review found electrical QST to be consistent in predicting persistent pain in one included study. However, the lack of sufficient evidence and the varied methodologies employed in its current usage render these recommendations inconclusive. The included studies were heterogeneous in study designs and included a small number of participants, which limits the applicability of findings to clinical practice. This review recommends future research employ robust methodologies to ensure consistent findings that may contribute to clinical relevance of QST within the niche of persistent pain.
Conflict of interest
All authors declare no conflict of interest.