
Abstract
BACKGROUND:
Daily activities that involve upper limb movements require muscle activation from different body parts by transferring forces and energy along the functional kinetic chain. The scapulae connect and transfer forces between the trunk and the upper limbs, so scapular dyskinesis may compromise the performance of the kinetic chain.
OBJECTIVE:
To assess the relationship between core muscle performance and shoulder pain and function in individuals with shoulder pain, with and without scapular dyskinesis.
METHODS:
Data was collected from 77 non-athlete adults aged between 18 and 50 years with shoulder pain, 45 had scapular dyskinesis. Core muscle performance was measured using the prone bridging test (PBT). Shoulder pain and disability were measured by the Shoulder Pain and Disability Index (SPADI), and the upper limbs’ stability was assessed by the Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST). The peak torque of shoulder external and internal rotators was measured using an isokinetic dynamometer. Multiple linear regression models evaluated the relationship between the PBT and CKCUEST, SPADI, and shoulder rotator strength.
RESULTS:
Significant correlations were found between the PBT and the SPADI total score (r = – 0.522), pain domain (r = – 0.513), and disability domain (r = – 0.501); normalized score (r = 0.593), and the power (r = 0.624) of the CKCUEST; and peak torque for external (r = 0.256) and internal (r = 0.292) rotations. Scapular dyskinesis did not influence the magnitude of the correlations and predictive values.
CONCLUSION:
The PBT was correlated with shoulder pain and function, but scapular dyskinesis did not affect the magnitude of these relationships.
Introduction
The kinetic chain theory also called the kinetic link principle, provides a framework for understanding and analyzing human movement patterns and the rationale for using exercise conditioning and rehabilitation programs that emphasize the entire body despite a target joint that presents pain and disability [1]. The kinetic link principle describes how the human body can be considered in terms of a series of interrelated links or segments, meaning that a movement of one segment can affect its proximal and distal segments [2–5]. Within this integrated system, the core is responsible for a large part of the production of strength and energy to carry out tasks that require using the upper limbs. Furthermore, good core function ensures greater protection against potentially harmful forces that can result in injuries and pain in the shoulder joint complex [6–10].
The assessment of core muscular capacity is clinically relevant regarding the risk of pain and musculoskeletal injuries, including shoulder pain [11, 12]. Biomechanical alterations on the kinetic chain have been previously explored in the athlete population, indicating that there are altered patterns of movement neuromuscular control, stability, resistance, strength, and power of the core muscles, especially in athletes of overhead modalities with shoulder pain. These alterations can also represent risk factors for the development of sports injuries [13–19]. Although the kinetic chain is an important aspect to be assessed in any individual who uses the upper body in daily activities, and not only in sports activities, the literature about the kinetic chain characteristics of non-athlete subjects with shoulder pain is limited. Lower muscular resistance and mobility of the thoracolumbar and hip regions, changes in thoracic posture, neuromuscular control impairments of the lower extremity, and balance/body stability deficits were present in this population [20–24]. However, other biomechanical aspects of the kinetic chain require investigation in non-athletic populations.
Some muscles that are part of the core are related to muscles that stabilize the scapula through myofascial and kinetic connections, such as the lower trapezius, serratus anterior, and external oblique. This relationship has been widely discussed and is not fully understood [25, 26]. In this context, the scapula acts as a connecting structure, transferring energy between the trunk and upper limbs and ensuring greater efficiency to the kinetic chain [27]. Adequate movement of the scapula allows for a better length-tension relationship of the scapulohumeral muscles, contributing to the optimization of dynamic stabilization of the glenohumeral joint, helping to prevent microtraumas in the subacromial tissues [8, 28].
The morphofunctional characteristics of the shoulder joint imply minimal bone restrictions and limited action of passive stabilizers, so it mostly depends on the contribution of dynamic stabilizers, such as the rotator cuff muscle [29]. However, these muscles originate from the scapula and depend directly on its positioning and functional synergism [30]. The visible change in the positioning and movement pattern of the scapula has been conceptualized as scapular dyskinesis [31]. Multiple factors are described as possible causes of scapular dyskinesis, including altered activation of periescapular muscles [27].
The literature is controversial about the influence of scapular dyskinesis on the development of dysfunction and painful diseases in the shoulder. A systematic review published in 2018 mentioned that the altered movement of the scapula has been related to a 43% higher risk of shoulder pain in athletes [32], and later, in 2020, another systematic review concluded that it does not predict shoulder pain and injuries [33]. Factors like speed, pain, stiffness, and fatigue can influence the movement pattern. However, the different movement patterns between the scapulae may not be a problem, being just normal kinematic variability [34, 35].
Shoulder pain is prevalent in the general population, representing 30% of all musculoskeletal painful diseases [36, 37]. Pain can be a modifying factor of movement patterns on the shoulder complex, including the scapulae [35]. Considering that the scapula plays an essential role in the transmission of forces, it is possible to speculate that scapular dyskinesis may act as a moderating factor in the relationship between the core and shoulder performances. The literature has shown associations between the core and shoulder muscles during the Upper Quarter Y-Balance Test and concluded that there is a moderate correlation between the performance on this test and the strength of the periscapular and core muscles, especially the serratus anterior and lower trapezius muscles in individuals with shoulder pain [38]. However, the presence of scapular dyskinesis as a moderating factor was disregarded.
In this sense, the present study aimed to evaluate the relationship between the isometric performance of the core muscles in the prone bridging test and shoulder pain and disability scores, stability of the upper limb in a closed kinetic chain, and the strength of the external and internal rotators of the shoulder of subjects with shoulder pain. Furthermore, to evaluate the interference of scapular dyskinesis in these associations.
Methods
Design, ethics, register, place and time
This cross-sectional study is part of a clinical trial registered at plataforma de Registro Brasileiro de Ensaios Clínicos (RBR-3g7q8bx). Data was collected at Universidade de Pernambuco, Petrolina Campus, Brazil, from August 2021 to February 2022. The local ethics committee approved the study (CAAE: 89885318.5.0000.5207), and all subjects signed the informed consent.
Recruitment and eligibility criteria
Subjects were recruited in Petrolina-PE and region through social media and in different health services. The researchers contacted some subjects directly, as they participated in previous studies. Males and females of 18– 50 years old, that presented bilateral or unilateral shoulder pain, associated with scapular dyskinesis or not (assessed by a yes/no method [31]) were recruited to participate in this study. They should be physically independent, non-athletes and have not participated in any structured physical exercise programs for at least three months. They must not have a history of trauma, fractures, and/or surgeries in the shoulder complex; or present serious changes in the thoracic and cervical spine (scoliosis, hyperlordosis, or hyperkyphosis) and upper limbs. Clinical tests for glenohumeral instability must be negative, and all subjects must be able to perform all the tests proposed in the evaluation.
Procedures
Recruitment and screening were carried out to identify eligible subjects. As they filled the inclusion criteria, they were informed about the objectives and procedures of the research, as well as the duration and possibility of withdrawing at any time. If they agreed to participate and signed the informed consent term, a questionnaire was applied as an interview to collect data regarding demographics, practice of physical activity, history of injuries or trauma to the shoulder joint complex, presence of pain or discomfort in the upper limbs or other regions and medication use. In addition, weight and height were measured, and the following specific tests were applied by an experienced researcher: Neer, Hawkins-Kennedy, Jobe, painful arch, and Resistance to External Rotation tests [39].
All subjects were submitted to an observational assessment of scapular dyskinesis by two experienced researchers simultaneously. The subject was in an orthostatic position and performed eight repetitions of a bilateral movement of raising the arm in the scapular plane until the maximum possible amplitude, holding dumbbells weighing approximately 3% of their body weight. The movement speed was standardized at three seconds for the concentric phase and three seconds for the eccentric phase, controlled by verbal feedback from the examiners. In case of disagreement between the examiners, the opinion of a third evaluator was required. The volunteer was classified into “with scapular dyskinesis” and “without scapular dyskinesis” [31, 40].
Outcomes
Shoulder Pain and Disability
The Shoulder Pain and Disability Index (SPADI) consists of 13 items that can be responded to 0– 10 scales and are distributed across two domains: pain (5 items) and disability (8 items). This questionnaire can be scored for each domain or its total score (0– 130 points). The higher the score, the worse the pain and/or disability of the shoulder joint. In case of pain in both shoulders, the volunteer was instructed to answer the questionnaire according to the most painful shoulder. The volunteer was reminded to report their pain and disability over the past week.
The SPADI is a reliable, valid, and responsive questionnaire for several shoulder pathologies, including non-surgical patients (shoulder pain, tendinosis, impingement syndrome, osteoarthritis, frozen shoulder) and surgical patients (rotator cuff repair, arthroplasty) [41]. The Brazilian version of SPADI showed high internal consistency (0.87 to 0.89) and excellent inter-session reliability (ICC 0.90 and 0.94) [42].
Upper limb stability
The Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST) was used to evaluate the stability of the upper limb in a closed kinetic chain task. Subjects were in a push-up position with their hands 91.4 cm apart and both shoulders aligned with their hands (Fig. 1). Two parallel and aligning tapes were placed on the floor to guide the movements of the hands during the test. From this position, they were instructed to alternately touch the contralateral hand (Fig. 1b) as fast as possible in 15 seconds while maintaining the correct push-up position [43]. Each subject performed three trials with a 45s-rest between trials. They were allowed to perform movement repetitions to familiarize themselves with the task.
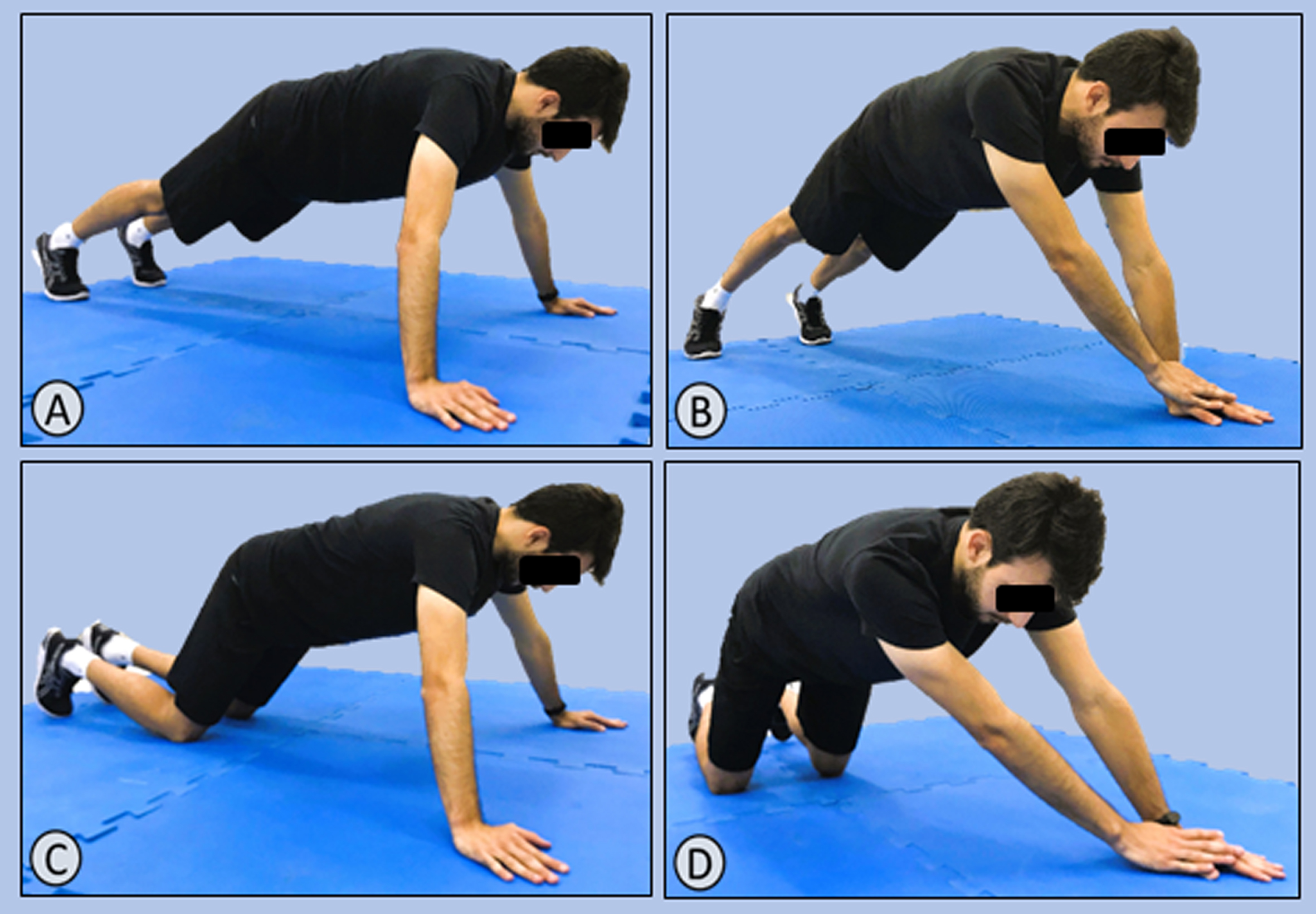
Body posture that should adopted during the Closed Kinetic Chain Upper Extremity Stability Test. A = Starting position for men; B = Body posture that men should maintain during the test; C = Starting position for women; B = Body posture that women should maintain during the test.
Males should perform the test with the back straight, the upper extremity weight should be perpendicular to the floor and over the hands, the knees should be out of the floor, and the feet should be kept in the starting position (Fig. 1a and Fig. 1b). Females were the same, but it was considered acceptable that the knees touched the floor from the beginning to the end (Fig. 1c e Fig. 1d). If the subject could not maintain the required body position during the execution of the test, it was interrupted and started again after 45 seconds of rest [43].
The final score of the CKCUEST was calculated by the average number of touches in 15 seconds, normalized by the subject’s height in meters. The power value of the test was obtained by multiplying the average number of touches by 68% of body weight in kilograms divided by 15.
The volunteers adopted a prone position on the floor and were instructed to lift their bodies from the floor, distributing their body weight on the forearms and feet, keeping the body as horizontal as possible [44] (Fig. 2). One maximal repetition of this test was performed in each session, and the test score was the duration in seconds that the athlete was in a plank position. The test was interrupted at the moment that the subject was not able to maintain the position.

Body posture that should be maintained during the prone bridging test.
The isokinetic muscle strength of the shoulder’s internal and external rotator muscles was assessed using the isokinetic dynamometer Kin-Com 125E (version 3.2; Chattanooga Group, Chattanooga, TN).
The torque produced by the internal rotator (IR) and external rotator (RE) muscles was evaluated using a protocol with an angular velocity of 60°/s during concentric actions with gravity correction [45]. Subjects performed three sets of five repetitions for each limb, with a two-minute interval between the sets and a 10-minute interval between the limbs. Before the evaluation procedures, a specific warm-up was carried out on the equipment, as the subject performed ten submaximal repetitions. During the assessment, to avoid compensatory movements, the trunk and pelvis were fixed to the seat with belts, as described in the recommendations proposed by the manufacturer. Peak torques (Newtons/meters) of internal and external rotation were used for analysis.
Statistical analysis
Numerical and categorical outcomes were described by mean and standard deviations or absolute and relative frequencies, respectively. The normality of distribution was checked with Shapiro Wik's test. To compare the subjects with and without scapular dyskinesis, t-tests for independent samples were used for the parametric data, while the Mann-Whitney test was used for non-parametric, and the Qui-squared test was applied to categorical outcomes.
Pearson correlation tests were used to test the association between the score obtained at the prone bridging test and the SPADI, the CKCUEST, and the isokinetic strength of internal and external rotator muscles. Scapular dyskinesis was added as a moderator effect of the correlations. Correlation coefficients were interpreted as poor (0.00 to±0.25), fair (±0.25 to±0.50), moderate (±0.50 to±0.75), or strong (±0.75 to±1.00) [46].
Multiple linear regression models were used to identify if the performance on the prone bridging test can predict the scores obtained on the SPADI, the CKCUEST, and the isokinetic muscular strength. Those models were adjusted by the presence of dyskinesis, sex, age, and body mass index. The stepwise method was adopted, maintaining the variables that presented statistical significance with the dependent variable, considering a p-value<0.05, and not overcoming a total of three factors due to the limited sample size (77 subjects). All models were tested for the following assumptions: Multicolinearity (Variance Inflation Factor < 5); absence of outlier and influence of values (Cook's distance < 1); absence of autocorrelation (Durbin Watson test between 1.5 and 2.5); normality and homoscedasticity of the residuals.
All analyses were carried out on the software JAMOVI (version 2.3), considering a significance value of 5%.
Results
Seventy-seven subjects, 34 females, average age of 35±8 years, were included in the study. Table 1 presents the characteristics of the total sample, as well as stratified for the presence (n = 45) or absence (n = 32) of scapular dyskinesis. P-values for the difference between the groups are also presented in Table 1, showing significant differences only for body weight (p = 0.021) and body mass index (p = 0.001).
Demographic, anthropometric, clinical, and general performance data for the total sample and the sample stratified by the presence/absence of scapular dyskinesis
Demographic, anthropometric, clinical, and general performance data for the total sample and the sample stratified by the presence/absence of scapular dyskinesis
SPADI: Shoulder Pain and Disability Index; CKCUEST: Closed Kinetic Chain Upper Extremity Stability Test; PT: Peak Torque. M: male, F: female, R: right, L: left; *statistically significant differences (<0.05).
Table 2 shows the correlation between the performance on the prone bridging test and the other variables, considering the total sample and the partial correlation, adjusted by the presence of scapular dyskinesis. In general, the significance level and the magnitude of the correlation did not change after the adjustment.
Correlations and partial correlations (adjusted for scapular dyskinesis) between the performance on the prone bridging test and the scores obtained from SPADI, CKCUEST, and peak torque during isokinetic muscle strength of rotator muscles
SPADI: Shoulder Pain and Disability Index; CKCUEST: Closed Kinetic Chain Upper Extremity Stability Test; PT: Peak Torque. *statistically significant correlation (<0.05).
The performance on the prone bridging test was negatively and moderately correlated with the total score of SPADI (r=– 0.522; p = 0.001) as well as with the pain (r=– 0.513; p = 0.001) and disability domains (r=– 0.501; p = 0.001). The performance on the prone bridging test was positively and moderately correlated with the normalized score (r = 0.593; p = 0.001) and power values (r = 0.624; p = 0.001) of the CKCUEST. Positive and fair correlations were found between the performance on the prone bridging test and the peak torque during external rotation (r = 0.256; p = 0.024) and internal rotation (r = 0.292; p = 0.010).
Table 3 presents the results from the multiple linear regression model adjusted for sex, age, body mass index, and presence of scapular dyskinesis. The analysis showed that the prone bridging test was capable of predicting disability (R2= 0.291); pain (R2= 0.280); the performance on the normalized (R2= 0.424) and on the power value of the CKCUEST (R2= 0.412); and the peak torque for external (R2= 0.394) and internal (R2= 0.451) rotations.
Results of the multiple linear regression model adjusted for sex, age, body mass index, and presence of scapular dyskinesis
SPADI: Shoulder Pain and Disability Index; CKCUEST: Closed Kinetic Chain Upper Extremity Stability Test; PT: Peak Torque. SE: Standard Error; CI: Confidence Interval; T: Test; M: Male.
The hypothesis that the core muscle performance would be correlated with shoulder pain, disability, stability of the upper limbs, and strength of the internal and external rotator muscles was confirmed since our results demonstrated correlations between fair and moderate. However, these associations were not modified by the presence of scapular dyskinesis. The multiple linear regression adjusted for age, sex, BMI, and presence of dyskinesis showed that the performance of the prone bridging test can predict almost 30% of pain and disability in subjects with shoulder pain.
Negative and moderate correlations were observed between the performance in the prone bridging test and SPADI scores, indicating that a lower core performance is associated with greater shoulder pain and disability. This can initially be justified by physiological factors related to the presence of pain and its ability to generate motor and cortical changes that modify the activation pattern and motor performance of the shoulder and shoulder girdle muscles, especially during isometric contractions [47]. During sustained contractions of these muscles, individuals with pain can generate altered muscle activation patterns that compromise force and energy transmission while maintaining closed kinetic chain postures [48, 49]. On the other hand, volunteers with high SPADI scores may have achieved lower performance on the prone bridging test due to the posture required, which involves weight bearing on the painful limb at a 90° flexion [43], which can cause pain during the test. This finding corroborates previous studies that showed lower performance of subjects with shoulder pain in the CKCUEST [50] and the Upper Quarter Y-Balance Test [51], which also require weight bearing in a close kinetic chain.
Scapular dyskinesis did not act as a moderating factor in the relationship between the prone bridging test and the SPADI. A possible explanation for this finding is that scapular dyskinesis is a functional adaptation and does not contribute to pain and disability, as an isolated factor [33, 34]. In fact, there is no consensus in the literature on whether scapular dyskinesis would be a risk factor for shoulder pain, being present in both symptomatic and asymptomatic individuals [52]. Previous studies have demonstrated that there are no significant associations between changes in scapular kinematics and symptoms of shoulder pain and disability [53, 54], and an intervention focused on the improvement of scapular mobility and motor control did not have a superior effect on the treatment of shoulder pain, compared to an intervention based on general exercises for the shoulder [55].
The CKCUEST was positive and moderately correlated with the performance on the prone bridge test, and dyskinesis was not a moderating factor in this relationship. Although the CKCUEST assesses the stability of the shoulder girdle and shoulder, it requires a lot of trunk stabilization to maintain the required posture during its performance [56]. A biomechanical analysis of the CKCUEST was performed and showed that men and women are supposed to support around 65% and 24% of their body mass, respectively, with their upper limbs. The remaining percentage is supported by the lower limbs, and the transmission of forces between the support points needs to go through the entire kinetic chain, especially through the core region [57]. In this sense, it seems plausible that there is a significant correlation between core performance and CKCUEST scores, and that the performance on the prone bridging test can predict up to 42% of the result of CKCUEST.
It is important to mention that the presence of shoulder pain could impact the performance on the prone bridging test given the loading that occurs through the shoulder and scapulothoracic complex during this task, so the correlations found between the prone bridging test and the CKCUEST and the SPADI may reflect that the prone bridging test incorporates loading through the shoulder, rather than a specific relationship between core muscle performance and these other variables. In order to have more precise conclusions about the performance of the core muscles, future studies should assess them independently.
Previous studies have shown a positive correlation between core muscle performance and periscapular muscle strength [26, 59]. Therefore, it is possible to speculate that volunteers with better conditioning of the core muscles may have a better transfer of force and greater activity of the periscapular muscles, resulting in better stability of the shoulder girdle and ensuring better performance in the CKCUEST. Once again, this was not interfered by scapular dyskinesis, similar to a previous study that showed that scapular dyskinesis did not influence the functional performance of the upper limbs on closed kinetic chain activities [60].
The performance of subjects with shoulder impingement on the Upper Quarter Y-Balance Test, which requires similar body posture with the CKCUEST and the prone bridging test, has also been correlated with core muscle strength. This study attributes the better performance on the Upper Quarter Y-Balance Test to a greater strength of the trunk flexors and lateral flexors, serratus anterior, and lower trapezius muscles [38].
Also, there was a positive and fair correlation between the performance on the prone bridging test and the peak torque of the shoulder rotator muscles, being able to predict the peak torque in external rotation by 39% and the peak torque in internal rotation by 45%. These findings corroborate with previous studies [61, 62] that found weak correlations between the isometric resistance of the core muscles and the peak torque of the shoulder rotators of athletes. However, there is limited literature that supports and explains this relationship. Possible explanations are based on studies that demonstrated prior activation of core muscles during upper limb movements [63–65]. This anticipatory activity could maintain trunk stability and contribute to transferring energy to the upper limb through the scapulae and periscapular muscles [25, 66].
Some limitations of this study should be assumed: (1) the core endurance was assessed during an isometric task, which does not represent all daily-life activities and the chosen test for core performance may be influenced by the presence of shoulder pain during the task; (2) the sample is composed of young and physically inactive adults, so these findings cannot be generalized to older groups and those who practice sports; (3) our results are valid for subjects with shoulder pain of low intensity and long duration, that jeopardize the generalization of the results for high intensity and acute kinds of pain; (4) the cross-sectional design does not allow to establish cause and effect relationships, but only associations between the analyzed outcomes. In this sense, future studies should explore these gaps to verify whether the inclusion of exercises aimed at improving the conditioning of the core muscles in rehabilitation programs can benefit patients with dysfunctions of the shoulder joint complex.
Still, these findings are clinically helpful for physiotherapists’ decision-making in the evaluation and rehabilitation processes of non-athlete patients with subacromial pain, as they reinforce the presence of a functional relationship between the core performance and the shoulder joint complex, and on the other hand, suggest that scapular dyskinesis doesn’t seem to influence it.
Conclusion
The performance of the core muscles during the prone bridging test is negatively and moderately correlated with shoulder pain and disability and positively and moderately correlated with the performance on the CKCUEST. The correlation between the performance on the prone bridging test and the isokinetic strength of external and internal shoulder rotators was fair and positive. The presence of scapular dyskinesis does not influence these associations.
Footnotes
Acknowledgments
None.
Conflict of interest
No conflict of interest is declared.
Ethical considerations
The local ethics committee approved the study (CAAE: 89885318.5.0000.5207), and all subjects signed the informed consent.
Funding
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) and Fundação de Amparo à Ciência e Tecnologia do Estado de Pernambuco (FACEPE).