
Abstract
BACKGROUND:
Knee swelling is common after total knee arthroplasty (TKA). However, there is limited literature on its clinical implications.
OBJECTIVE:
The study aimed to determine whether a correlation exists between increased postoperative knee circumference, pain, functional score and range of motion.
METHOD:
Between November 2019 and June 2020, 114 patients were retrospectively enrolled in this study. Primary endpoints included the correlation between knee circumference change (KCC, and 1) postoperative pain 2) Oxford Knee Score, and 3) postoperative range of motion. These data were collected on day 2 and at 6 months postoperatively.
RESULTS:
The mean knee circumference (KC) increase on postoperative day 2 was 9.27%. No statistically significant correlation was found between KCC and pain (p = 0.853), KCC and patient-controlled analgesia (PCA) consumption (p = 0.265), KCC and knee flexion (p = 0.729) and extension (p = 0.157). At 6 months postoperatively, no statistically significant correlation was found between KCC and pain (p = 0.909), and Oxford Knee score (p = 0.137). However a statistically significant correlation was observed between increased KC of more than 10% and extension deficit at 6 month postoperatively (p = 0.012), as well as between KCC on day 2- and at 6 months postoperatively.
CONCLUSION:
After TKA the average increase in KC is around 10%. Increased postoperative knee effusion is neither an indicator for increased pain nor for unfavorable functional scores. At 6 months postoperatively, a correlation exists between increased KC and extension deficit for knees with more than 10% KCC. This study addresses common patient inquiries to physiotherapists regarding knee swelling following TKA.
Keywords
Introduction
Total knee arthroplasty (TKA) consistently ranks among the top 5 most frequently performed surgeries annually in the United States [1], and results in a high degree of patient satisfaction [2]. However, one in five patients (19%) is not satisfied with the outcome [3] and complication rates of up to 22% are reported [4]. Common non-medical complications are instability, periprosthetic joint infection, stiffness, deep venous thrombosis, implant loosening and neuro-vascular injury [5]. Preoperatively, knee effusion on osteoarthritis indicates joint distress. An osteoarthritic knee with effusion can lead to altered activation of the quadriceps and hamstring muscles during walking [6, 7]. After TKA, knee swelling, which is considered a minor complication is found in 15.6% of patients [8]. Furthermore, it is a frequent cause of arthroplasty-related hospital readmission [8]. For some authors, knee swelling after TKA leads to pain, reduced range of motion and negative perception of the recovery process [9, 10].
Knee swelling after TKA is attributable to both effusion and oedema. The intra-articular swelling tensioned the capsule and limits range of motion (ROM) while extra-articular swelling causes a cam effect on the soft tissues [11]. Knee circumference (KC), measured 1 cm above the patella, is a good indicator of knee intra-articular effusion [12]. Furthermore, this measurement has excellent intra-tester reliability in patients with TKA, allowing its use in patient follow-up [13]. KC measurements include all the anatomic structures, without allowing to differentiate what is attributable to soft tissue, typically muscle volume versus joint effusion. This study was motivated by the scarce literature on postoperative knee swelling and its impact on functional scores, ROM, and pain. The aim of this article is provide the physiotherapist with data to anticipate possible issues and address their patients’ inquiries regarding postoperative knee swelling. Furthermore, it would enable us to better identify patients who need close monitoring. The main hypothesis is that patients with major postoperative swelling will present higher pain levels, lower functional scores, and reduced ROM.
Methods
Approval for this retrospective study was obtained by the institution’s ethic committee before data collection. 163 patients who underwent TKA between November 2019 and June 2020 were screened for potential eligibility. Inclusion criteria were unilateral TKA in patient aged from 40 to 95 years with end-stage knee osteoarthritis of grade four according to Kellgren-Lawrence classification. Exclusion criteria were patients with 1) missing data in the file 2) chronic pain management issues defined as pain lasting longer than three months [14] and not related to knee osteoarthritis, 3) antecedent of knee arthrotomy and/or hardware implantation around the knee joint. 114 patients meeting study criteria were enrolled (Fig. 1).
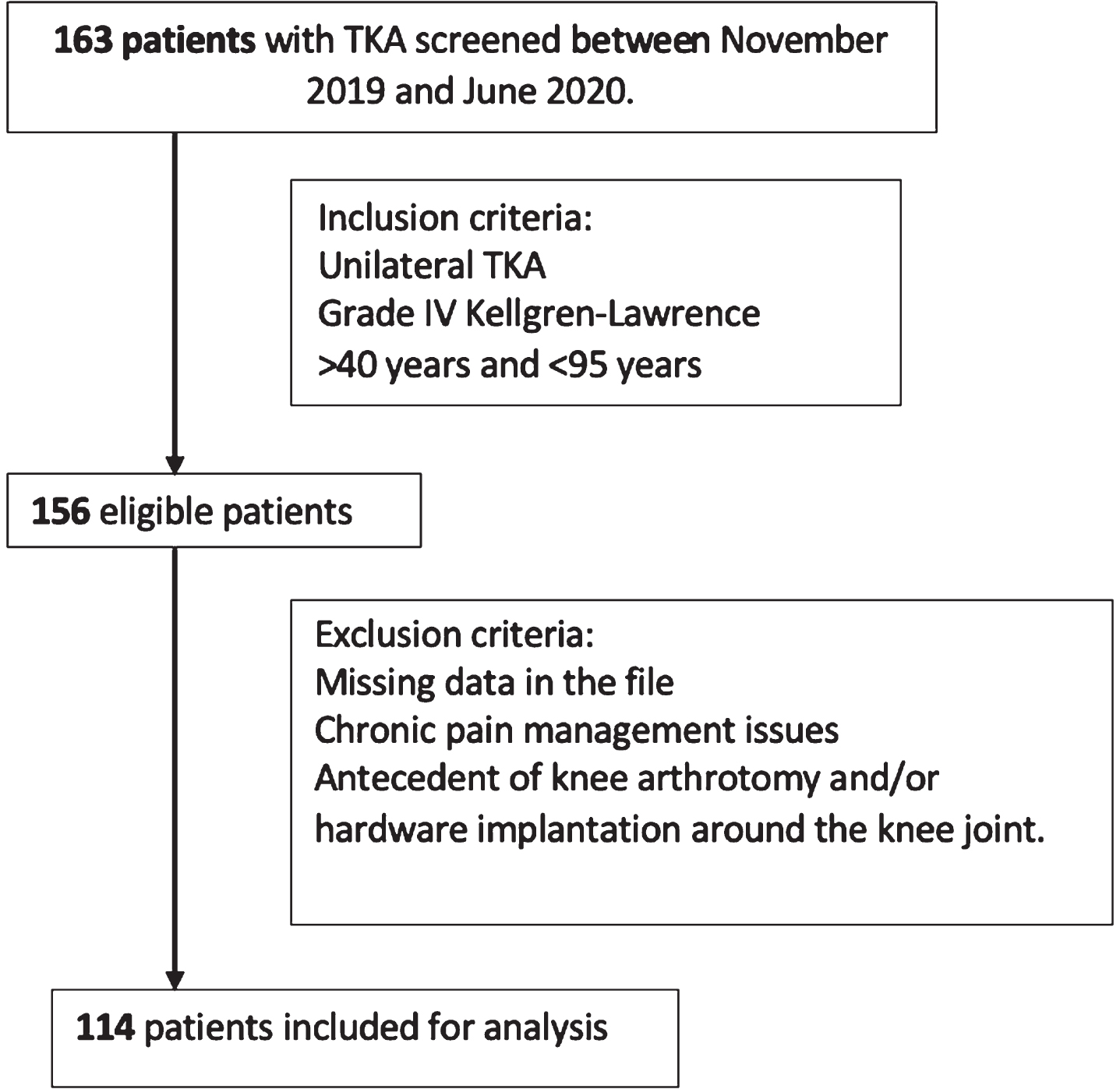
Study flowchart.
Patients’ baseline characteristics were retrospectively collected from the electronic medical records: Demographics included age and gender. Comorbidities comprised body mass index (BMI), diabetes, hypertension, and rheumatoid arthritis. Laboratory values included pre- and post-operative hemoglobin (Hb) and hematocrit (Hc). Operative variables included laterality and type of anesthesia. All demographics and clinical characteristics are summarized in Table 1.
Demographic and clinical characteristics of the studied population
n, number; SD, standard deviation.
All operation were performed by two senior knee surgeons under general or spinal anesthesia. A cruciate retaining mobile bearing, fully cemented TKA (Attune knee CR RP system DePuy Synthes, Warsaw, IN, USA) without patellar resurfacing was implanted through a medial subvastus approach for all cases. All patients received 1 g of IV tranexamic acid (TXA) 30 minutes prior to the incision and intraoperative pericapsular local anesthetics injections.
No suction drains were used.
The primary endpoints of this study were the postoperative changes in KC and their correlation with pain, functional score and ROM.
The pain was assessed by patient-controlled analgesia (PCA) morphine pump consumption 24 hours after the surgery. Knee pain was also measured via a visual analogue scale (VAS) 2 days, and 6 months after the surgery. Passive ROM, was assessed manually with a goniometer preoperatively, at 2 days, and 6 months post-surgery. Functional outcomes were assessed using the Oxford Knee Score (OKS) at 6 months postoperatively and compared to the pre-operative OKS. KC was measured before, and 2 days and 6 months after TKA 1 cm above the patella with a non-stretchable band. Patients were positioned supine with their knees in an extended position and lower extremity musculature relaxed. The knee circumference change (KCC) (increase or decrease) expressed as a percentage of the preoperative KC was calculated for every patient.
The change in knee circumference was measured as a change (%) from the preoperative circumference.
The KCC on postoperative day 2 = (diameter on day 2 (cm) –preoperative diameter (cm))/preoperative diameter (cm).
The KCC at 6 month postoperatively = (diameter on month 6 (cm) –preoperative diameter (cm))/preoperative diameter (cm).
Two groups will be compared based on a cut-off of 10% increase in KC providing a target value for physiotherapists.
Statistical analyses
Descriptive statistics of the population are expressed as mean±standard deviation (SD) for continuous variables. The other parameters are expressed in number (n) of subjects or in ratio. The relationships between the different quantitative variables were analyzed by Pearson correlation coefficients (r). Group comparisons according to KCC cut-offs were performed by Student’s t-test. SPSS Statistics software (version 28.0.1.0; IBM Corp, Armonk, NY, USA) was used for our statistical analyses. A value of p < 0.05 is used as statistically significant.
Results
The mean preoperative joint circumference was 43.09 centimeters (cm) (±4.34) and increased to 47.02±4.43 cm (9.27%) on postoperative day 2. At 6 months, the mean perimeter decreased to 43.79±4.78 cm resulting in a 2.78% increase of KC compared to pre-operative values (Table 2). The mean flexion on day 2 is 74.8°±12.2, and extension is 8.1°±8.3. At 6 months, these values increase to 123.1°±8.1 and 0.2°±2, respectively. For pain VAS, the average value on day 2 is 3.8±2.2, dropping to 0.3±0.7 at 6 months. The mean KOS at 6 months is 45.1±4.8 (Table 2).
Mean joint perimeters±standard deviation
Mean joint perimeters±standard deviation
KC, knee circumference; cm, centimeters; VAS, visual analogue scale; OKS, Oxford Knee Score (worst 0; best 48).
Regarding the relationship between the parameters on postoperative day 2: The Pearson correlation coefficient (r) between KCC and pain was 0.020 (p = 0.853). Between KCC and PCA consumption, r = –0.119 (p = 0.265). The relationship between KCC and knee flexion and extension on postoperative day 2 were r = –0.037 (p = 0.729) and r = –0.150 (p = 0.157), respectively. At day 2, using a 10% KCC increase cut-off, there was no difference between the 2 groups regarding extension (p = 0.824).
Regarding the relationship between the parameters at 6 months postoperatively: the Pearson correlation coefficient between KCC and pain is 0.012 (p = 0.909). The relationship between KCC and knee flexion and knee extension at 6 months post-op was r = –0.178 (p = 0.094) and r = 0.264 (p = 0.012) respectively.
At 6 months, knees with a KCC≥10% increase have a statistically higher extension deficit (p = 0.021) than the other group.
In addition, KCC at day 2 post-op was not correlated with the difference in Oxford Knee Score (6 months –pre-op) for which r = 0.158 (p = 0.137). Finally, the correlation between KCC on day 2 and 6-months post-op was r = 0.208 (p = 0.049).
The most important finding of this study is that in patients undergoing TKA, an increase in postoperative knee swelling does not correlate with elevated pain, reduced flexion or lower OKS. However, an extension deficit at 6 months is more likely if a KC increase of more than 10% was observed on postoperative day 2. This information allows us to reassure the patient and explain that acute postoperative swelling is a normal process that does not impede early functional rehabilitation. Notably, our patients often inquire about the potential impact of a swollen knee on their rehabilitation or an increase in postoperative pain. This study allows us to answer questions frequently asked by patients and to identify patients who might benefit from intensive postoperative physiotherapy.
Rehabilitation physiotherapy is a key element for surgical success and improves physical function after TKA [15]. The post-operative period is a crucial time during which physiotherapists and surgeons collaborate closely. However, the physiotherapist often serves as the primary point of contact for the patient, addressing their questions and concerns while alerting the surgeon to any complications that may arise. Postoperative swelling of the knee is normal after TKA. However, patients are often concerned about it. After TKA, studies report a 10% increase in KC, caused by intra-articular blood accumulation and quadriceps swelling [16, 17]. This study found a similar average KC increase of 9.27%. For some authors, increased postoperative KC is correlated with decreased ROM after TKA [18]. The correlation between the KC at 2 days and 6 months allow us to advise patients that if acute postoperative swelling occurs, it is normal to observe a significantly more swollen knee at 6 months. Another important parameter is the evolution of the KC over time. Patients whose knee remains swollen (>10%) should receive special attention from the physiotherapist and closer follow-up by their surgeon because they are at risk of having an extension deficit at 6 months. However, it does not affect pain score. Some studies found that stiffness (defined as flexion contracture >15 degree and/or flexion <75 degree) resulted in higher dissatisfaction [19]. In this study, the maximum extension deficit measured at 6 months postoperatively was 10 degrees.
This study has certain limitations. First, this is a monocentric retrospective study. Second, the COVID-19 pandemic made frequent data collection (once a month) impossible, and only one in person visit 6 months after the surgery was deemed appropriate in the absence of complications. Additionally, despite standardization, it’s possible to have some intra-evaluator variations in measuring KC.
Conclusion
Increased postoperative knee circumference is not an indicator of increased postoperative pain and morphine consumption, lower Oxford Knee Score and reduced flexion range of motion. However, swollen knees (>10% increase compared to preoperative values) deserve special attention because they are at increased risk of extension deficit at 6 months postoperatively. Knee swelling is expected to gradually decrease over the postoperative period. This study provides physiotherapists with valuable tools to address questions frequently asked by patients in the critical postoperative period.
Footnotes
Acknowledgments
We would like to acknowledge the essential collaboration of the physiotherapist involved in patient rehabilitation.
Conflict of interest
Bernard Geulette: Royalties from Bone and Joint research.
Eric Manche, David Mazy, and Gautier Beckers: None.
No benefits in any form have been received or will be received relating to this article. Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Ethical considerations
Ethics approval was obtained by the hospital’s ethics committee.
Author Contributions
Study design, B.G., E.M., and G.B.; Data collection, D.M. and G.B.; Data analysis, D.M. and G.B.; Writing of manuscript, G.B.; Edition of manuscript, B.G., E.M., D.M. and G.B.; Surgeons, B.G. and E.M.; Revision and Final approval of the manuscript B.G., E.M., D.M. and G.B.