
Abstract
BACKGROUND:
Current clinical guidelines recommend that a multidisciplinary team inclusive of allied healthcare practitioners deliver assessment and intervention for disorders of consciousness. Allied health professionals include music, occupational, physical, and speech therapists. These allied health clinicians are challenged to select interventions due to a lack of evidence-based recommendations regarding rehabilitation interventions that support recovery of consciousness. This umbrella review synthesizes available systematic reviews (SRs) that describe occupational, speech and language, physical and/or musical therapeutic interventions for people with disorders of consciousness.
OBJECTIVES:
Identify and summarize evidence from systematic reviews (SRs) that examine allied healthcare interventions for patients with disorders of consciousness. Additionally, this umbrella review aims to evaluate the impact of allied health interventions on recovery of consciousness, methodological quality and risk of bias for the included systematic reviews.
METHODS:
An umbrella review was completed. The review was reported according to the Preferred Reporting Items for Overview of Reviews (PRIOR) guidance. Five academic databases (PubMed, CINAHL, PsycInfo, Web of Science, and the Cochrane Library) were searched for SRs and/or meta-analyses of allied health (i.e., music, occupational, physical, and speech therapy) interventions for disorders of consciousness. For included studies, data were extracted and quality of the SRs appraised using the A Measurement Tool to Assess Systematic Reviews (AMSTAR) 2 checklist. Data extracted from each SR identified the authors and years of primary studies, interventions, comparators, and outcomes related to recovery of consciousness (i.e., neurobehavioral/cognitive), functional status, physiological response pain, and adverse events. Rehabilitation interventions were categorized and described.
RESULTS:
Fifteen SRs were included and three of these reviews conducted meta-analyses. Identified rehabilitation interventions included: 1) sensory stimulation, 2) median nerve stimulation, 3) communication/environmental control through assistive technology, 4) mobilization, and 5) music-based therapy. SRs were published between 2002 and 2022 and included 2286 participants. Using the AMSTAR 2, the quality of reviews was critically low (k = 6), low (k = 3), moderate (k = 4), and high (k = 2). SRs within this umbrella review demonstrated significant heterogeneity in research methods and use of outcome measures to evaluate the recovery of consciousness within the primary studies. These factors influenced the ability to conduct meta-analyses.
CONCLUSIONS:
Sensory stimulation, median nerve stimulation, music therapy and mobilization are all interventions that demonstrate some level of benefit, but current SRs fail to prove benefit through high-level quality evidence. There is an indisputable need for continued rehabilitation research to expand options for treatment modalities and to ensure that the interventions being applied to DoC rehabilitation are evidence-based to improve consciousness and recovery.
Introduction
Disorders of Consciousness (DoC) are a complex phenomenon that present in patients after severe brain injury. Clinical presentation of DoC at the bedside include behavioral phenotypes of coma, vegetative state/unresponsive wakefulness syndrome (VS/UWS), and the minimally conscious state (MCS) (Giacino, J. et al., 2022). DoC has been the focus of increased clinical and research efforts within brain injury medicine as more patients are surviving catastrophic neurological insults (Claassen, 2020). Large database outcome studies such as TRACK-TBI and Traumatic Brain Injury Model Systems have demonstrated a high percentage of patients with DoC, after severe traumatic brain injury, progress to achieve emergence into consciousness (Kowalski et al., 2021; McCrea et al., 2021). Additional outcome studies have demonstrated a large portion of those patients that achieve consciousness continue to improve their functional status as identified by functional outcome tools such as the Glasgow Outcome Scale Extended and Functional Independence Measure (FIM) (Hammond et al., 2019; Malone et al., 2019; Whyte & Nakase-Richardson, 2013).
Evidence supports the need for specialized rehabilitation to promote recovery and achievement of the aforementioned outcomes (Sattin et al., 2020; Seel et al., 2013). Early mobilization and rehabilitation interventions have been investigated with severe brain injury across the continuum of care, including early rehabilitation within the intensive care unit. Results of these studies identify the benefit of early mobilization and rehabilitation interventions in improving patient arousal, awareness and outcomes (Bartolo et al., 2017; Roth et al., 2013; Schaller et al., 2019). DoC Practice Guideline Recommendations, supported by the American Academy of Neurology, recommend patients experiencing DoC be referred to specialized post-acute rehabilitation after acute care once medically stable (Giacino, J. et al., 2018). Further rehabilitation recommendations include utilizing interventions focused on promoting progression of consciousness, mitigating secondary complications and engaging families in education and training in caring for their loved one within specialized DoC programs (Giacino, J. et al., 2020).
Despite the growth of empirical evidence demonstrating the efficacy of specialized rehabilitation for patients in DoC, across the care continuum, there continues to be a paucity of research identifying effective therapeutic interventions provided by allied health practitioners. For this paper, we defined allied health practitioners as those from either the physical therapy, occupational therapy, speech and language pathology and/or music therapy discipline. A qualitative study identified that allied health practitioners are “trying things” with patients in DoC likely due to the dearth of evidence-based information (Weaver, 2023). The objective of the umbrella review was to examine published systematic reviews (SRs) focused on allied health rehabilitation interventions for patients in DoC and investigate the efficacy of the interventions across the continuum of care. The core research questions were: (1) What types of rehabilitation interventions have been investigated through SRs and/or meta-analyses? (2) What extent were the rehabilitation interventions demonstrating an impact on recovery of consciousness? (3) What were the types of neurobehavioral, cognitive, and functional assessments utilized to examine improving consciousness? A secondary objective of this umbrella review study was to examine the quality and risk of bias of the SRs and the methodology of primary studies included in SRs.
Methods and materials
The umbrella review methodology is reported according to the PRIOR guidance (Gates et al., 2022). The umbrella reviews was pre-registered with the International Prospective Register of Systematic Reviews (PROSPERO: CRD42023407844). The authors identified a priori inclusion and exclusion criteria, search strategy, selection process, data abstraction process, risk of bias assessment, and synthesis methods.
Inclusion and exclusion criteria
Inclusion criteria for the umbrella review were: (1) met criteria for a SR or SR with meta-analysis; (2) rehabilitation interventions included in allied health scope of practice; (3) only included patients in DoC from brain injury etiology; (4) included pediatrics and adults; (5) English only publications; and (6) included DoC specific outcome measures measuring level of consciousness and/or function. A SR was defined as having conducted a search strategy using identified terms, identifying inclusion/exclusion criteria, reporting the flow of included studies, and synthesizing the results for the purposes of this study. The primary outcome measure of interest, agreed upon by authors, was change in level of consciousness. Level of conscious awareness explored the level of behavioral responsivity observed (measured using clinical neurobehavioral assessment).
Exclusion criteria were studies that were: (1) not a SR or meta-analysis; (2) did not exclusively focus on interventions that were not part of allied health’s scope of practice (e.g., deep brain stimulation, medications); (3) did not exclusively include patients in DoC; and (4) were not published in English. The authors chose to exclude SRs focused on non-invasive brain stimulation (e.g., transcranial Direct Current Stimulation) because they are not currently available as a reimbursable intervention for allied health practitioners in addressing consciousness with brain injury.
Search strategy
The search strategy was developed through consensus of authors (AMM, JAW, BM) and informed by current guidance in relation to umbrella review design (Aromataris et al., 2015). First, an initial search was completed on two databases (PubMed and EMBASE) to identify relevant systematic reviews in relation to the umbrella review question. Following the identification of initial key words, additional key words, found within the titles and abstracts of the systematic reviews were identified. Key words related to the condition (disorder of consciousness, vegetative, unresponsive wakefulness syndrome, minimally conscious state, severe brain injury), the nature of therapy under investigation (music, speech, language, occupation, physio, physical, cognitive, sensory, stimulation) and the types of studies sought (systematic, review, meta-analysis) were included in our search strategy. The search strategy was adapted for each of the five databases. The search was run in April 2023 across five databases: Web of Science (1980 to date), PsychInfo (1987 to date), PubMed (1980 to date), CINAHL (1980 to date) and the Cochrane Library. Repositories of SRs were also searched including the PROSPERO register, the JBI Database of Systematic Reviews and Implementation Reports and the Database of Abstracts of Reviews of Effects. The database searches included all studies published before March 31, 2023.
Selection process
Articles retrieved from each database were exported into Covidence (www.covidence.org). Screening of titles and abstracts was completed by reviewers (JAW, BM, SF, AMM, JR, HK) using our pre-determined inclusion and exclusion criteria. When there was a conflict between two authors on inclusion of a title/abstract, a third author provided the deciding vote to include or exclude SRs for full-text review and data extraction. Following screening of title and abstract, remaining studies underwent full text review by two independent reviewers.
Data abstraction
A detailed data extraction template was created based on expertise and Cochrane guidance (Higgins, 2022). Data extracted included the number of relevant primary studies included in the SR, years primary studies were published, number of study participants, study characteristics, SR methodology, SR outcome measures, SR results, SR risk of bias, conclusions and limitations. In cases where the SR did not explicitly report certain results or study characteristics, authors (BM, JAW, AMM, SF, JR, HK) attempted to extract from the primary studies included in the respective SRs.
For SR outcome measures, the primary outcome of interest was level of consciousness. Secondary outcomes related to functional status, physical status, pain, quality of life, and adverse events were abstracted. Physical status included measures of movement and strength. Pain levels were those measured according to visual scales or the nociceptive pain scale. Finally, not all meaningful outcomes for DoC can be demonstrated on a standardized assessment of consciousness.
Quality appraisal
The quality of each SR was evaluated using the AMSTAR 2 checklist (Shea et al., 2017). AMSTAR 2 was designed for healthcare professionals to facilitate rapid and reproducible assessment of the quality of SRs that include randomized and non-randomized studies. The AMSTAR 2 is one of the most utilized appraisal tools and the recent revision to the AMSTAR made it applicable to non-randomized studies (Shea et al., 2017). Users of the AMSTAR 2 apply constructs when evaluating the quality of a SR including inclusion and exclusion criteria and disseminating of that criteria, search and review methods, adequate description of included studies and assessment of risk of bias and report of potential biases. Authors rated seven of the AMSTAR 2’s 16 items because prior evidence identified that those particular items likely determine the overall quality rating (critically low, low, moderate, and high) (Pieper et al., 2021). A quality rating of critically low indicates there is more than one critical flaw and should not be relied on to provide an accurate review of the primary studies, a low quality rating indicates that there is one critical flaw, a moderate rating indicates there is more than one noncritical weakness, and a high rating indicates there is up to one noncritical weakness (Shea et al., 2017).
Overlap of primary studies
During the data abstraction, authors extracted the primary author and year of each relevant primary study within the 15 SRs and investigated which SRs had overlapping primary studies.
Synthesis of findings
The authors synthesize the data by categorizing each systematic review by the interventions presented to provide a detailed synthesis.
Results
Figure 1 summarizes the search results and study selection process. A total of 9665 studies were identified. After exclusion of 3357 duplicate publications, authors screened the titles and abstracts of 6308 for relevance and inclusion. 142 articles were retained for full-text review for eligibility. After completion of full-text reviews, 15 SRs were included and underwent data extraction by authors. The other 126 SRs were excluded as they did not adequately meet one or more of the umbrella review inclusion criteria. Details of the 15 SRs are included in Table 1. Many of the SRs explored more than one rehabilitation intervention. The SRs investigated allied health interventions of sensory stimulation (Cossu, 2014; G. E. Lancioni et al., 2010; J. Li et al., 2020a; Lombardi et al., 2002; Meyer et al., 2010; Weaver et al., 2023; Zuo et al., 2021), mobilization (Martens et al., 2017; Ng & King, 2021; Weaver et al., 2023), right median nerve stimulation (RMNS) (Feller et al., 2021; Meyer et al., 2010; Wang et al., 2022; Weaver et al., 2023), use of assistive technology for environmental control (Klingshirn et al., 2015; G. E. Lancioni et al., 2010) and music therapy (Grimm & Kreutz, 2018; Klingshirn et al., 2015; X. Li et al., 2020b; Meyer et al., 2010; Weaver et al., 2023). Additional rehabilitation interventions were not identified within the 15 SRs. SRs were published between 2002 and 2022 and included a total of 2286 participants and included both male and female.
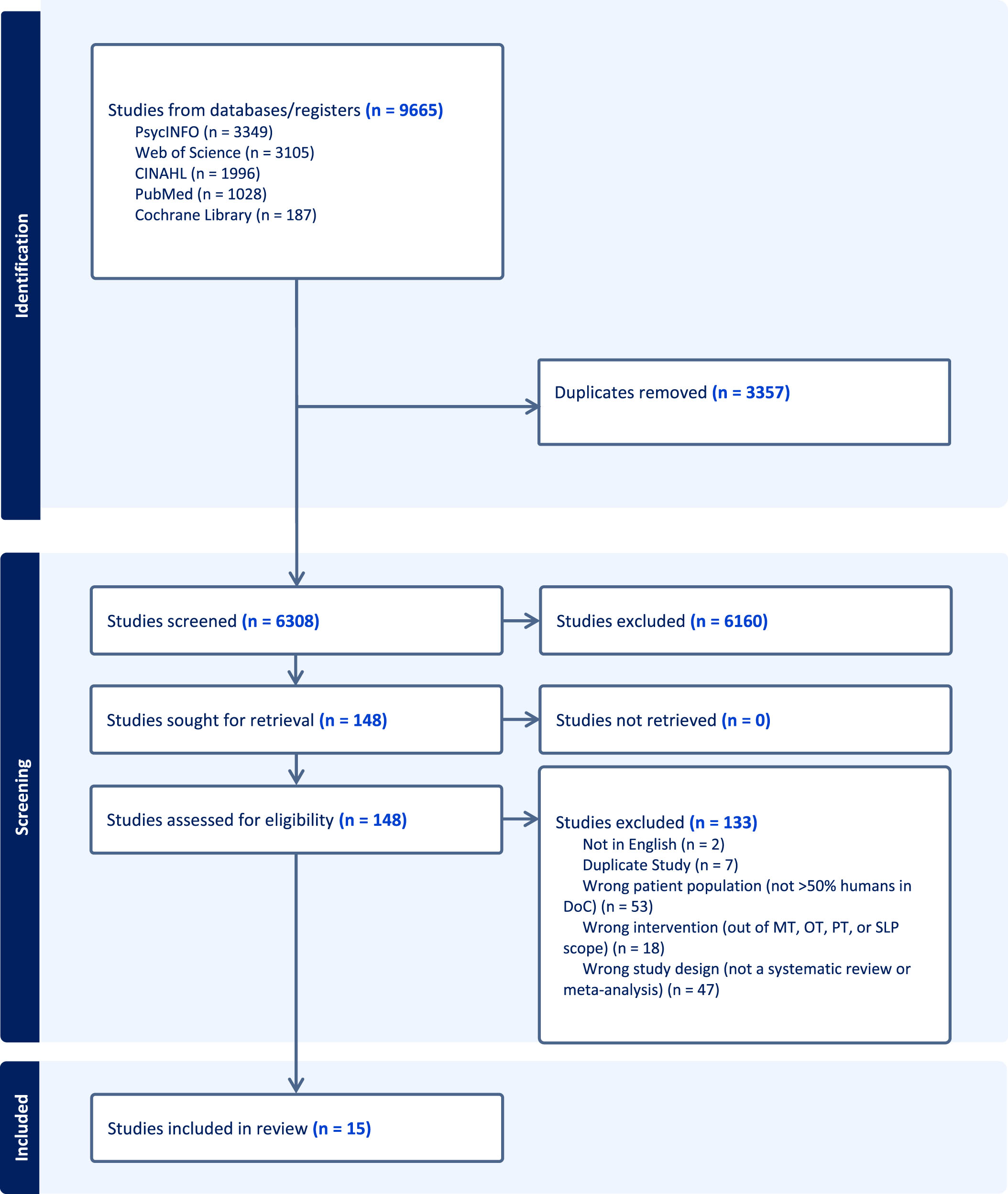
PRISMA flowchart.
Summary table of included 15 systematic reviews
The AMSTAR 2 tool (Shea et al., 2017) was used to appraise the quality of the 15 systematic reviews, of which only two reviews conducted a meta-analysis and two meta-analyses. AMSTAR items 2, 4, 7, 9, 11, 13 and 15 were applied to each SR (https://amstar.ca/AmstarChecklist.php). Two studies were rated as high quality (Padilla & Domina, 2016; Weaver et al., 2023), four as moderate quality (Feller et al., 2021; Grimm & Kreutz, 2018; Lombardi et al., 2002; Zuo et al., 2021), three were rated as low (X. Li et al., 2020; Ng & King, 2021; Wang et al., 2022) and six studies were rated as critically low in quality (Cossu, 2014; Klingshirn et al., 2015; G. E. Lancioni et al., 2010; J. Li et al., 2020; Martens et al., 2017; Meyer et al., 2010). See Table 2. Thus 60% of SRs included were of low or critically low methodological quality. See Table 2.
AMSTAR 2 results of eligible systematic reviews
AMSTAR 2 results of eligible systematic reviews
Acronyms: Y (Yes); N (No); PY (Partial yes); N/A (Not Applicable); H (High); M (Moderate); L (Low); CL (Critically Low).
The studies met or partially met AMSTAR 2 items two (n = 7) and four (n = 13) which appraised if the SRs explicitly stated the review methods established prior to conducting the review and included a comprehensive search strategy. Nine of the SRs met or partially met item 7 of AMSTAR regarding dissemination of exclusion criteria. Nine studies met or partially met item nine on assessing risk of bias (RoB). Only two studies met item 11 regarding meta-analyses of the data included within the SRs. Nine studies met or partially met item 13 accounting for RoB. Finally, item 15 regarding adequate investigation of publication bias, only one study met the criteria.
The 15 SRs include 110 primary studies that met criteria. Of these primary studies, overlap existed. The primary studies with over three citations across the systematic reviews included Cooper et al., 1999 (3), Johnson et al., 1993 (k = 4), Mitchell et al, 1990 (4), Davis et al., 2003 (4), Megha et al., 2013 (3), and Salmani et al., 2017 (3). These studies focused on sensory stimulation and median nerve stimulation. Nineteen primary studies were cited in two systematic reviews and the rest were singular citations across reviews. Table 3 illustrates the overlap of primary studies within the 15 SRs.
Matrix of primary study overlap within systematic reviews
Matrix of primary study overlap within systematic reviews
Level of conscious awareness
Due to the heterogeneity of outcome measurement, the predominant narrative analysis within the systematic reviews and the range of population characteristics, it was difficult to identify the effectiveness of interventions using outcomes for level of consciousness. All fifteen SRs reported use of some form of standardized neurobehavioral assessment in at least one of its primary studies. There was a wide range of standardized neurobehavioral assessment tools reported within and between SRs. Reported uses of a standardized neurobehavioral assessment across the primary studies within the systematic review ranged from one to eight. The Glasgow Coma Scale (GCS) was the most commonly reported outcome measure of awareness reported across twelve SRs inclusive of coma, UWS/VS and MCS. The Coma Recovery Scale-Revised (CRS-R) was reported across six of the systematic reviews. Other assessments reported included the Glasgow Outcome Scale, the Wessex Head Injury Matrix, the Western Neuro Sensory Stimulation Profile, the Disability Rating Scale, The Music Therapy Assessment Tool for Awareness in Disorders of Consciousness (MATADOC), the Sensory Modality Assessment and Rehabilitation Technique, Kings Outcome Scale, Rancho Los Amigos Scale, Sensory Stimulation Assessment Measure and the Functional Independence Measure (FIM). Frequency of observed behaviors was also listed as an assessment measure in two systematic reviews (Meyer et al., 2010; Ng & King, 2021). The heterogeneity of data analysis meant that there was not consistent reporting of findings in relation to each standardized assessment and thus it is difficult to draw conclusions on their role in capturing conscious awareness within research studies.
Physical status
Physical outcomes were not commonly reported. Outcomes related to movement and strength were reported in two systematic reviews (Martens et al., 2017; Ng & King, 2021). One systematic review investigating spasticity management for disorders of consciousness (Martens et al., 2017) had two relevant primary studies, which reported using the Modified Ashworth Scale, the Modified Tardieu Scale and range of motion to measure effectiveness of interventions on physical status. Ng and King (2021) reported narratively on three primary studies that also utilized the Modified Ashworth Scale.
Pain
Pain was not reported as an outcome in the fifteen SRs.
Clinically meaningful change and other measures
Clinically meaningful change outcome explored measurement for any meaningful change reported and which would be important clinically, but may not change scoring on a neurobehavioral assessment scale. This outcome had limited reporting across the SRs. Other measures such as the Richmond Agitation Sedation Scale (Ng & King, 2021), the FIM (Cossu, 2014; Padilla & Domina, 2016) and the Early Rehabilitation Barthel Index (Ng & King, 2021; Weaver et al., 2023) were reported in three of the reviews but their clinical utility in understanding of functional change was underexplored.
Findings of allied health interventions of included systematic reviews
Analysis of SRs found commonalities of allied health rehabilitation interventions investigated for efficacy in improving consciousness in patients with DoC. The most studied interventions were sensory stimulation and median nerve stimulation. Additional interventions identified within SRs were mobilization/verticalization, communication or environmental control with use of assistive technology, and music-based therapy. These interventions fell within the scope of practice for physical and occupational therapists, speech-language pathology and music therapists. A cohort of SRs included multiple interventions within a single SR (N = 7). Some SRs also included interventions that did not fall within the scope of allied health practitioners such pharmacotherapy, tDCS or deep brain stimulation (Cossu, 2014; G. E. Lancioni et al., 2010; Meyer et al., 2010). Authors only extracted and evaluated data included in SRs that focused on rehabilitation interventions that would fall within the scopes of the allied health practitioners.
Sensory stimulation
Sensory stimulation was the most studied rehabilitation intervention for patients with DoC (Cossu, 2014). The authors found similar results within the umbrella review. Sensory stimulation as an intervention for DoC was included in 60% of the SRs (n = 9). Most sensory stimulation protocols included stimulation of multiple sensory systems of auditory, visual, tactile, olfactory, gustatory, proprioceptive, kinesthetic and vestibular. Dosing of sensory stimulation was disseminated. Most sensory stimulation protocols reported within primary studies included short bursts of multimodal sensory stimulation for 5–15 minutes 2–5 times a day for a duration of one to four weeks (Davis & Gimenez, 2003; Johnson et al., 1993; Mitchell et al., 1990). There was significant heterogeneity between sensory stimulation protocol dosing and few RCTs were included. The most common outcome assessment to evaluate the effectiveness of sensory stimulation was the GCS.
Lombardi et al., (2002) conducted a Cochrane SR and included three randomized controlled trials (RCTs) focused on sensory stimulation with individuals with traumatic and non-traumatic coma and VS. 68 participants identified as DoC underwent multimodal sensory stimulation protocols. Variance was found in the sensory stimulation protocols as well as outcome measures. GCS was a common outcome measure; however, there was a lack of additional sensitive outcome measures to identify a change in function. Methodology and quality assessments demonstrated and lack of strength and methodological rigor to conclude results of studies to be valid. Consequently, this Cochrane review was unable to conclude that sensory stimulation was efficacious in improving level of consciousness in patients with DoC.
Cossu (2014) included sensory stimulation with 93 participants within a SR investigating several rehabilitation interventions. There was a significant overlap in the sensory stimulation studies included with those of aforementioned Lombardi (2002). The reported dosing and sensory simulation protocols were heterogeneous in frequency, intensity and duration. The GCS was a consistent outcome measure utilized within the primary studies included in the systematic review. 50% of the studies analyzed found improvement in GCS scores after sensory stimulation. The other half of studies found no improvement or significant change. Only one of the primary studies investigated was RCT methodology and that study found no significant difference between the control and experimental groups (Cooper et al., 1999). Despite the inconsistent results of Cossu’s SR, the stated conclusion was sensory stimulation is promising intervention that demonstrates a level of efficacy, is feasible and safe for patients with DoC.
Meyer and colleagues (2010) utilized a similar approach to Cossu (2014) and examined multiple pharmacological and rehabilitation interventions for DoC to assess if interventions promoted emergence from DoC. Meyer et al (2010) included eight sensory stimulation studies with 187 participants. Only one study was RCT design. The primary studies demonstrated significant variance in outcome measures used. Certain studies utilized the GCS, while others applied physiologic response, Disability Rating Scale (DRS), eye and reflexive movements. There was also overlap identified in Meyer SR to the previous two SR. Similarly, there was inconclusive evidence that sensory stimulation was beneficial to improve emergence after DoC.
A large systematic review was conducted by Klingshern (2015) focused on rehabilitation interventions provided to patients with chronic DoC served in long-term care settings. 53 studies were included in this SR. However, similar to many of the SRs reviewed, this study focused on multiple rehabilitation interventions, which also included sensory stimulation, which was the most reported rehabilitation intervention. However, many of the primary studies including sensory stimulation also combined the intervention with assistive technology, thus impeding ability to compare results of this SR with others. Additionally, none of the 39 studies including sensory stimulation as an intervention or part of an intervention was RCT design. The majority were single or small cohort case studies. There was an absence of reporting of sensory stimulation dosing protocols to compare between studies. Additionally, there was a significant lack of application of outcome measures within this SR to assess efficacy of intervention. This SR reported the “what” of interventions as multimodal sensory stimulation being provided by rehabilitation at a long-term level of care. However, it failed the report “how” the interventions were prescribed and failed to report results of sensory stimulation. The strength and methodology of this large SR with multiple studies was substantially poor and AMSTAR 2 grade of critically low in quality and thus conclusion of benefit was unable to be reached based on the results of this SR even though a large number of studies were included within this SR.
Median nerve stimulation
Median nerve stimulation was primarily conducted to the right side, but one systematic review also included primary studies that provided median nerve stimulation to the left side or bilaterally (Wang et al., 2022). Across the five included systematic reviews, there were 27 unique primary studies. All primary studies included the Glasgow Coma Scale as an outcome measure except for one that utilized the Glasgow Outcome Scale (Peri et al., 2001). Other outcome measures included EEG, brain blood flow, Disability Rating Scale, and days in the intensive care unit. A few studies also included the functional independence measure. Only one systematic review included a meta-analysis (Wang et al., 2022) and although this systematic review and meta-analysis were identified to have low quality, they found that right median nerve stimulation facilitated better outcomes for recovery of consciousness. Bilateral median nerve stimulation was also found to have a positive outcome for recovery of consciousness, but the effect size was smaller than that of right median nerve stimulation (Wang et al., 2022). There is high heterogeneity in the dose, frequency, and duration. Only four of the five studies reported the median nerve stimulation dose. From those four studies, right median nerve stimulation was typically applied using 15 to 20 mA with pulse width of 200 to 300 us at 35 to 40 Hz. Median nerve stimulation was applied from one week to three months. When reported, adverse events were not statistically significant compared to a control group.
Mobilization
Tilt table
Verticalization using a tilt table with the purpose of increasing arousal and cognition was discussed in two systematic reviews (Ng & King, 2021; Weaver et al., 2023). Due to variability in methodologies and intervention protocols in the primary studies, there was inconclusive evidence on the effectiveness of this intervention. Positive trends in cognition and arousal were noted with the use of a title table, but long-term impact on emergence from DOC was unclear. The addition of robotic or passive stepping on top of a tilt function resulted in less syncopal events and longer duration tolerated in the right position (Luther et al., 2007). One study found the title table alone to result in better long-term outcomes than the addition of robotic stepping, so more research is needed to explore the effectiveness of this additional component (Krewer et al., 2015). This same study explored the impact of tilt table with and without passive stepping on spasticity, and no statistically significant differences were found between groups on the Modified Ashworth Scale (MAS), but these physical assessments were not compared to no intervention. The spasticity remained the same or improved in most muscle groups with tone increasing in only 19.7% of all muscle groups (Krewer et al., 2015).
Intervention protocols for verticalization consistently included a gradual progression to upright with maximal tilt height ranging from 60–90 degrees. Progression in protocols were based on medical stability utilizing vitals and monitoring of signs that align with a pre-syncope events. The majority of protocols targeted 20–30-minute treatment durations. Intervention frequency ranged from one visit to 24 visits delivered 3 times per week. Studies that included robotic stepping in addition to the tilt function, there was an absence of consensus on stepping rate with a range of 18-60 steps/minute reported.
Positioning and stretching
The impact of passive positioning of the upper extremity using a soft rolled resting hand splint and passive stretching were reviewed in one systematic review which focused on spasticity management in peopled with DOC (Martens et al., 2017). 13 out of 15 primary studies were excluded from this review due to their focus on medical management not delivered by rehabilitation professionals or it was a SR that was not specific to DOC. This SR also had weak methodology including only searching one database resulting in a high risk for missing relevant primary studies.
In the one primary study that focused on this treatment intervention, a significant decrease in spasticity was seen immediately following both splinting and passive stretching, but improvements at 60 minutes post-intervention were only maintained in the splinting group (Thibaut et al., 2015). Improvements in passive hand opening were only observed in the splinting group but these improvements were not maintained at the 60-minute follow up. Clients falling into the VS/UWS had greater responses to this intervention than those classified as in a MCS (Thibaut et al., 2015).
Environmental control and assistive technology
Klingshern’s SR (2015), which examined various rehabilitation interventions within multiple domains, also included a compendium of studies focusing on use of assistive technology to promote environmental control. These studies by Lancioni and colleagues were conducted between 2009–2012 and utilized micro-switch and voice output communication devices (VOCA) to allow the patients to active radios, TVs and call for the attention of caregivers to promote self-agency through a variety of motor responses. These studies were single-case or small cohort case series implementing the ABABCB methodology with a baseline, a B intervention phase with familiar or enjoyable stimulus with monitored response, and a C non-contingent stimulus phase. Multiple 5–10 minute sessions were completed with participants over unreported timeframes (days vs weeks vs months). These studies found that mass repetition in engaging with micro-switch technology allowed patients in DoC, to learn to engage and control their environment through use of assistive technology and could be applied clinically to improve patient participation and self-agency (G. Lancioni et al., 2009; G. E. Lancioni et al., 2010, 2012). However, the nine studies by Lancioni and colleagues utilizing the same ABABCB methodology with different cohorts of patients found varying results of responses and conclusions of the studies were inconsistent between one another.
Music therapy
Two quantitative SRs of music-based treatment for DoC were found and aid in providing recommendations for practice. Twenty primary studies across two SRs were identified, with the most recent publication date being 2018. Quality assessment of studies found high risk of bias in three studies, medium risk in 14 (one excluded from the present manuscript), and four with low risk. Three included studies were randomized controlled trials with Ns greater than 15. Eight were single cohort. Others included a variety of controls and or comparisons. Many studies indicated being exploratory in nature. Trends towards beneficial outcomes were found though heterogeneity across all aspects of studies existed in design, stage of disorder, setting, music intervention, dosing, and quality.
The SR by Grimm & Kreutz (2018) aimed to identify behavioral and physiological responses used with music-based intervention, evaluate study quality, and review contextual factors of the music interventions. Generally, positive results were found for behavioral and physiological responses. Examples of behavioral responses correlated with significant findings included body movements and facial expressions. Physiological parameters of interest were many with highlights from select studies being impact on heart rate and temperature increases. Different kinds of music were shown in a study to produce different physiological responses. Significant changes in brain activity were found in several studies, some of which corresponded to behavioral responses. Incorporation of verbal messages was a common theme across studies demonstrating benefits related to brain activity. Biographic music and interactive strategies were employed in studies demonstrating significant favorable outcomes (DoC status). More recently, Li et al. (2020b) sought to expand on Grimm & Kreutz’s (2018) narrative through systematic review and meta-analysis. Authors identified four categories of analysis: a) functional scales for example, GCS and PVS with findings from one study indicating a significant impact on PVS, b) physical (physiological) indices in which, music was found to have significant impacts were facial expression and systolic blood pressure, c) EEG with no significant findings, and d) favorable outcomes of brain activity showing significant increases for two studies. Respective interventions were vastly different. This study serves as a collection of quantitative research that has specifically looked at the impact of music on DoC, however, little specific recommendations can be taken from it.
The examined reviews provide support and promise for researchers to build on for future investigations into the impact of music-based treatment of DOC. Particularly, investigators might seek to delineate the impact of recorded verse live preferred music, improvisational techniques compared to existing preferred music, other music-based stimulation strategies (i.e. research selected classical music), and dosing. Recommended treatment strategies might include use of biographical music, verbal messages, and interactive strategies. Biographical (preference-based) music can be selected by close relatives, family, and or loved ones. Incorporated verbal messages may include the clients name and relative created and conducted narratives. Practitioners could consider using interactive music therapy approach strategies such as active, dialogic, and improvisational techniques involving real time music creation integrating bids for engagement with music adjusted in response to observation.
Discussion
SRs represent the highest level of evidence on the hierarchy of evidence pyramid and thus this umbrella review, through analysis of fifteen relevant SRs looked to examine and report on existing evidence for allied health rehabilitation interventions for individuals in DoC. While SRs are growing in number of publications in this field due to the increasing number of research studies being undertaken, they require much more rigorous reporting. Heterogeneity was found to be widespread within the SRs across population samples, nature of intervention, methods of analysis and outcome measured used. Further limitations of this umbrella review were the potential of missing data in non-English studies that were excluded as well as potentially neglecting studies that examined rehabilitation interventions not captured within the included allied health professions or were not reported within SR methodology. These multiple limitations make it difficult to draw conclusions to support clinical practice interventions included within the SRs. SRs identified various rehabilitation interventions that can be utilized for treatment of individuals in DoC. However, analysis of SRs found significant methodological and quality limitations that restricted ability to conclude the interventions examined are irrefutable in benefit to improve level of consciousness.
Overall, results found the most evidence for sensory stimulation, which showed a positive trend towards effectiveness, and limited adverse events were reported. It was also noted that the elicitation of purposeful behavioral responses occurred more frequently when family were involved. Thus, rehabilitation practitioners should incorporate a standardized sensory stimulation protocol that embeds the family to deliver some or all of the intervention. Although sensory stimulation was the most common intervention for individuals with DoC, the literature under-investigates senses such as gustatory, olfactory and vision. Most research is heavily concentrated on auditory and tactile sensory systems.
Right median nerve stimulation was also found to have a positive impact on improving level of consciousness through evaluation of SRs investigating efficacy of median nerve stimulation. Dosing and prescription of median nerve stimulation had a level of heterogeneity that requires continued investigation, stronger methodology and randomized controlled trials with a larger number of patient participants. Allied health interventions focused on mobilization, promoting vertical positioning and passive range of motion found strongest evidence for passive range of motion in improving spasticity. Mobilization studies focused on improving standing time or robotic stepping to facilitate improved consciousness were small and had mixed methodologies thus results supporting efficacy was inconclusive. Results of efficacy of music therapy were similar to the interventions mentions previously. There was an identified trend in benefit in improving consciousness, but the heterogeneity of methodologies hindered ability to make conclusive statement of efficacy.
Allied therapy professions have more widespread interventions that can be used with patients in DoC that were not explored or detailed within available SRs such as robotic gait technology to promote intensive mobilization. A narrative study of rehabilitation practitioners described treatments such as adapting the environment to create a calming space to an activity that positioned the patient in front of a television to watch a comedy show (Papadimitriou et al., 2022). There can be various reasons for a limited cadre of rehabilitation interventions that have undergone SRs including a lack of robust clinical research focused on additional modalities. Authors also posit the need for increased investigation of multi-modal rehabilitation such as sensory stimulation during vertical positioning. There is a considerable need for allied health practitioners to conduct future research that explores the efficacy of rehabilitation interventions facilitating improved consciousness.
Future rehabilitation research also requires critical appraisal of outcome measures used to assess benefit of the intervention. The GCS is the most common assessment of consciousness utilized in brain injury medicine and the GCS was the most utilized assessment tool within the primary studies of the SRs included. However, the GCS has inherent limitations in sensitivity to reveal change in consciousness and identify the nuances of behaviors to identify DoC phenotype progression (Bodien et al., 2021). Additional options for outcome measures that have proven validity, reliability and sensitivity to detect meaningful change is required as part of future methodology in rehabilitation research.
Conclusion
Allied health practitioners are crucial members of interdisciplinary care teams to support recovery for DoC. Sensory stimulation, median nerve stimulation, music therapy and mobilization are interventions that demonstrate some level of benefit, but current SRs fail to prove benefit through high-level quality evidence. There is an indisputable need for continued rehabilitation research to determine the effectiveness of existing and novel rehabilitation interventions that can be delivered by allied healthcare practitioners (i.e., music, occupational, physical, and speech therapists). It is imperative that the interventions being applied to DoC rehabilitation are evidence-based to facilitate consciousness and recovery.
Footnotes
Acknowledgments
The authors would like to acknowledge the efforts of the medical librarians who assisted in informing the search strategies for this umbrella review.
Conflict of interest
The authors have no conflicts of interest to declare related to the work and efforts related to this umbrella review.