
Abstract
BACKGROUND:
Virtual reality (VR) interventions have been increasingly used in the rehabilitation of a wide range of neurological and neuropsychological dysfunctions. Findings of previous reviews showed positive and promising effects of VR-based interventions. However, they summarized findings on VR-based intervention carried out through different VR systems and tasks.
OBJECTIVE:
We carried out a narrative review with the aim of qualitatively synthesising the results of previous studies that used specific VR systems, i.e. the Khymeia –Virtual Reality Rehabilitation System, for treatment purposes.
METHODS:
We searched the literature in various databases (i.e. EMBASE, Web of Science, SCOPUS, PubMed and PubMed Central) for studies published until November 23, 2023.
RESULTS:
30 studies were selected. The VRRS was used for neuromotor rehabilitation only in 13 studies, for cognitive rehabilitation in 11 studies, and for both neuromotor and cognitive rehabilitation in six studies. The study design was heterogeneous including 15 randomised controlled trials.
CONCLUSION:
After discussing each study according to the type of rehabilitation we concluded that the use and efficacy of VRRS rehabilitative intervention for increasing the neurological and neuropsychological functioning of patients are promising but more evidence is needed to make a comparison with conventional treatment. Future studies should also include long-term follow-up as well as cost-effectiveness analysis.
Background
Virtual reality (VR) artificially simulates life-like environments providing a sensation of being inside an artificial world (Riva et al., 2020). It has been conceptualized as “an advanced form of human-computer interface that allows the user to interact with and become immersed in a computer-generated environment in a naturalistic fashion” (Rizzo et al., 2002; Schultheis & Rizzo, 2001). VR technology may be used as a tool for the study, assessment, diagnosis, and treatment of several neurological and neuropsychological disorders (Rizzo et al., 2002; Weiss et al., 2006). The use of VR makes it also possible to implement interventions of telerehabilitation (TR), i.e. an application of telemedicine that concerns the remote delivery of a variety of rehabilitative services through telecommunication technology (Piron et al., 2009).
VR-based treatment may provide several advantages compared with traditional rehabilitation methods in neurological and neuropsychological rehabilitation (Morganti, 2004; Rizzo et al., 2002; Schultheis & Rizzo, 2001). One assumption for its use in rehabilitation is that VR treatment provides multisensory feedback that could enhance the neural plasticity underlying neurological and neuropsychological recovery (Hao et al., 2021; Leonardi et al., 2021). In addition, skills learned during VR intervention might transfer or generalize to the real world (Schultheis & Rizzo, 2001; Wang & Reid, 2011).
As a consequence,VR interventions have been applied in the treatment of a wide range of neurological and neuropsychological dysfunctions associated with several conditions, such as neurodegenerative disease (Oliveira et al., 2021; Serino et al., 2017), cerebral palsy (Bryanton et al., 2006; Golomb et al., 2010; Park et al., 2021), stroke (Gamito et al., 2017; Kim et al., 2019; You et al., 2005), and neurodevelopmental disorders (Rodrigo-Yanguas et al., 2021; Wang & Reid, 2011; Zhao et al., 2021). Recently, several research groups synthesised the available evidence on the efficacy of VR-based intervention(s) for neurological and neuropsychological rehabilitation in different conditions, for example, in post-stroke (Maier et al., 2019; Rintala et al., 2019; Tchero et al., 2018), multiple sclerosis (Nascimento et al., 2021), and aphasia (Cacciante et al., 2021).
The available reviews and meta-analyses mainly summarized findings on VR-based intervention carried out through different VR systems (i.e., different hardware, software, and devices) and tasks. From both clinical and research perspectives, it is also essential to address the use and the efficacy of specific VR system. Thus, we carried out a narrative review with the aim of qualitatively synthesising the results of previous studies that used a specific virtual reality system: the Khymeia –Virtual Reality Rehabilitation System (VRRS). The VRRS allows the implementation (also via TR) of both neuropsychological and neurological rehabilitation treatments based on immersive or non-immersive virtual reality (for a detailed description of the K-VRRS see https://khymeia.com). The aim of this work was to review how the VRRS has been used in previous studies summarizing the features (e.g., tasks, duration) of the VRRS treatment as well as studies’ findings.
Methods
The study design was specified as a non-systematic general narrative review on the applications of the VRRS for treatment purposes irrespective of study design. The narrative review was prepared in accordance to previous recommendations on standards for reporting of narrative reviews (Baethge et al., 2019; Byrne, 2016; Gasparyan et al., 2011; Green et al., 2006; Kable et al., 2012; Pautasso, 2013).
Literature search
Initially, we searched EMBASE, Web of Science, SCOPUS, PubMed and PubMed Central for studies published until January 31, 2022 using the following keywords: Khymeia or VRRS or “virtual reality rehabilitation system”. Moreover, we searched for other potential references the following: bibliographies and citations of included studies, bibliographies of recent systematic-reviews and meta-analyses. Finally, other resources (i.e., Khymeia website, Google and Google Scholar) were searched for gray literature. No language restriction was applied. To ensure timeliness, we carried out an update of the literature search on November 23, 2023, using the same procedure specified above.
Study selection and data extraction
Firstly, we examined the presence of possible duplicates in the obtained pool of records using Zotero 5.0 for Windows. Secondly, two investigators independently screened titles and abstracts. Subsequently, the same two investigators conducted the full-texts assessment. The screening occurred during February 2022. Any discrepancies were resolved by consensus and, if necessary, through arbitration by the lead investigator.
The eligibility criteria were single case and analytical studies that reported information on patients functioning assessed at both pre- and post-treatment and in which the VRRS was used as treatment intervention. We excluded review and studies in which the VRRS was not used for treatment (e.g., as a tool for the assessment of patients).
Two investigators performed the data extraction. A data extraction form was filled with all the relevant data, i.e., authors and year of publication, condition under treatment, study design, blinding procedure, total number of patients and their mean age in years, intervention aim, and treatment duration (with a focus on the VRRS).
Outcomes
The VRRS provides both neuromotor and cognitive modules (and tasks) for rehabilitation. Consequently, the main outcome(s) of this review was to analyze the improvement in the neuromotor and cognitive domains. We focused on primary outcome(s) of each original study that the use of VRRS was intended to treat/improve and, specifically, on results of randomized controlled trials when available. For easy of reporting, we grouped studies according to the outcome for which the VRRS module was used. Further, we structured the presentation and discussion of the studies’ findings according to study design.
Results
Search results and included studies
The literature search yielded 456 records. After the removal of 201 duplicates, 255 titles and abstracts were screened. Then, 168 records were excluded and 87 full text were assessed for eligibility. Sixty-eight articles were further excluded because they did not address the VRRS or its use for treatment purposes. Nineteen studies were retained. After screening references of published review, included studies, and other resources two additional studies were retrieved. During the literature search update, nine additional studies were found endorsing criteria for inclusion out of a total of 81 records. A final number of 30 studies were retained. The study selection process is shown in Fig. 1 whereas the studies characteristics are summarized in Table 1 and other features of VRRS treatments, i.e., specific tasks when reported, in Table 2.
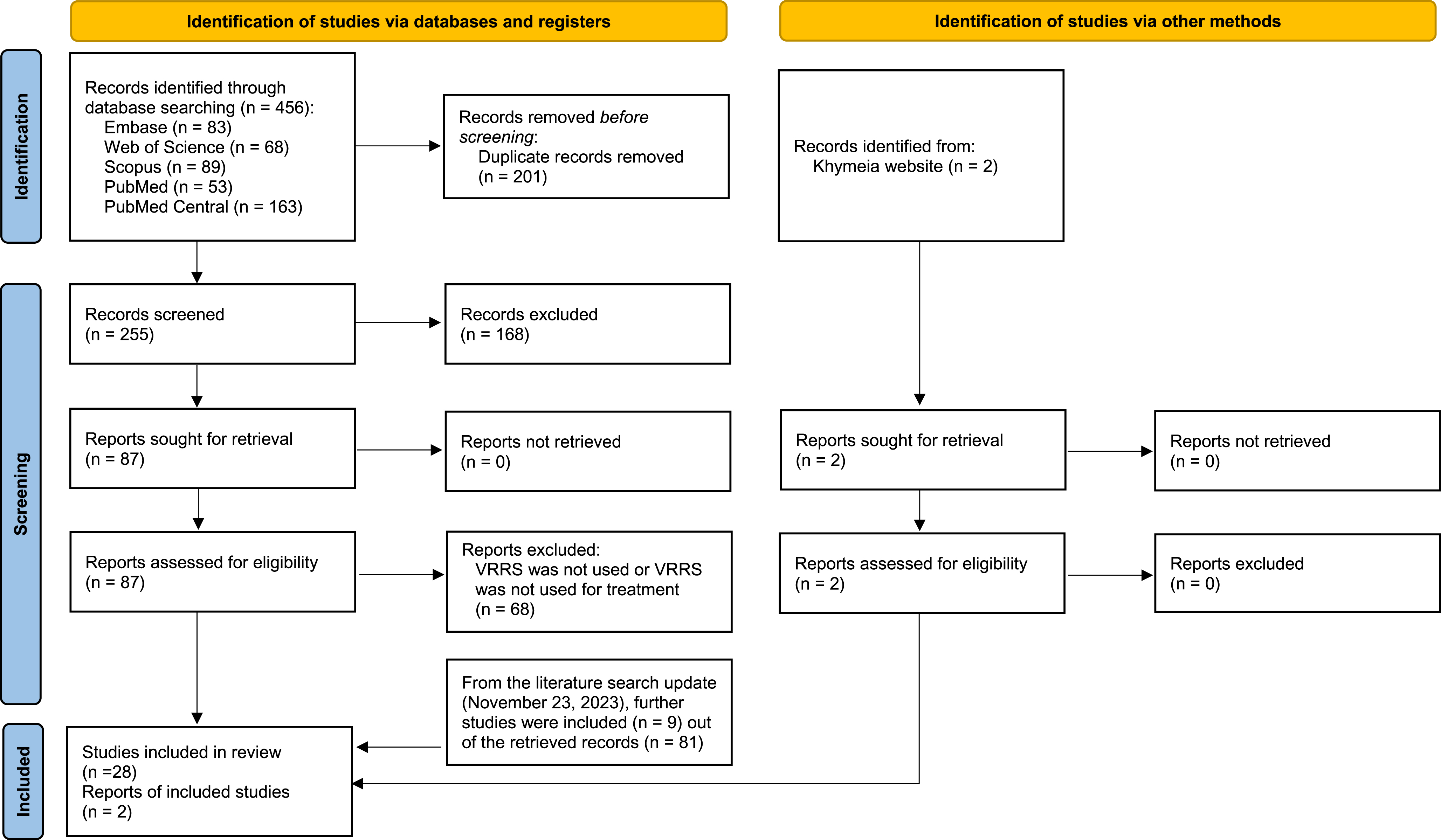
Adapted PRISMA flow diagram from Page et al. (2021).
Characteristics of included studies
Note. Randomization was considered “present” if the authors of the study specified the randomization procedure. VR: virtual reality treatment, CT: conventional therapy, w: weeks, d: days, h: hours, m: minutes, na: not applicable, ns: not specified.
Features of VRRS treatments (i.e., specific tasks)
Note. We report intervention and/or exercise descriptions provided in the original study. We had no access to the supplementary material from Maresca et al. (2020) that describes VRRS exercises.
The VRRS was used for neuromotor rehabilitation in 13 studies, for cognitive rehabilitation in 11 studies, and for both neuromotor and cognitive rehabilitation in six studies. Of all 30 studies, seven were single case reports, five uncontrolled trials, two non-randomised controlled trials, one quasi-randomised controlled trial, and 15 randomised controlled trials.
The VRRS was used for neuromotor rehabilitation in 19 studies: five case reports, four uncontrolled trials, two non-randomised controlled trials, and eight randomised controlled trials.
Nonexperimental design
Several studies examined whether neuromotor recovery may take advantage from adding VRRS training to standard treatments. Some case reports suggested the possibility of using the VRRS in combination with physiotherapy and/or other treatment to improve motor functions (Chillura et al., 2020; Luque-Moreno et al., 2016; Maresca et al., 2018). Luque-Moreno and colleagues (Luque-Moreno et al., 2016) described the use of the VRRS in addition to conventional physiotherapy programs in the treatment of post-stroke gait disorders in two patients. Menici and colleagues (Menici et al., 2021) reported on the VRRS based motor intervention via TR to improve posture and balance abilities in a 17-years-old female with a diagnosis of myopathy and moderate intellectual disability. Whereas Maresca et al. (2018) used both the VRRS based neuromotor and cognitive trainings to improve motor and cognitive functioning of a 60-years-old man with spinal cord injury showing good outcomes overall. Chillura et al. (2020) have described an intensive neuro-rehabilitation program lasting 6 months, carried out under hospitalization, aimed at the improving motor and muscle deficits in a patient with intensive care unit acquired weakness. The authors (Chillura et al., 2020) stressed that combining different rehabilitation strategy including conventional treatment (i.e. physiotherapy and occupational therapy), robotic-aided training, and sessions of neuromotor training based on VRRS, could provide more advantages than conventional treatment alone in improving motor functions. De Luca et al. (2022a) reported an improvement in head and trunk control in a patient with Nasu-Hakola disease (i.e., a rare neurodegenerative disorder) after a multimodal treatment including both VRRS and standard physiotherapy.
With respect to uncontrolled studies, Olivieri et al. (2013) showed a reduction of upper limb motor impairment in a group of children with congenital hemiplegia after traditional physiotherapy and VRRS interventions. Alemanno et al. (2019) conducted a 6 week-neurorehabilitative treatment using the VRRS with patients with chronic low-back pain. The treatment consisted on teaching patients to execute correct movements with the painful body part in order to reduce pain and to regain a correct body image. The results of the study showed a significant reduction in pain and improvement in quality of life. Another study (Maistrello et al., 2021) showed that, concomitantly to the use of the VRRS, post-stroke patients’ motor impairment of upper extremities improved. Finally, Contrada et al. (2022) assessed motor recovery after a TR intervention performed using VRRS in a group of chronic post-stroke patients. The authors found an improvement in motor functions of the upper paretic limb whereas no pre- post-difference was found in motor functions of the lower paretic limb.
All these findings certainly encourage further studies testing the efficacy of VRRS in neurological and neuromotor rehabilitation. Despite promising, as generally noted by the authors, evidence arise from single case and single group pre-and post-test research designs. As a consequence, findings suffer from low internal validity due to absence of comparison groups and implementation of other treatments in the original studies. For example, Olivieri and colleagues (2013) stressed that their study doesn’t provide evidence that the VRRS alone improves motor functions in children since physiotherapy was also provided. The authors highlighted the need of randomized controlled studies to adequately test the efficacy of VRRS based motor treatment.
Experimental design
Besides case reports and single-arm studies discussed above, ten studies adopted a controlled experimental approach with eight of these studies using randomization procedures. Four studies (Kiper et al., 2011, 2014; Luque-Moreno et al., 2021; Turolla et al., 2013) compared the VRRS based motor training, combined with conventional treatment (e.g., physiotherapy), with conventional treatment alone in improving motor impairment of upper or lower extremities in post-stroke patients. All these studies used the Fugl-Meyer Upper/Lower Extremity (FM) and the Functional Independence Measure (FIM) scales as outcome measures. Overall, these studies demonstrated that combined treatment (i.e., VRRS based training combined with conventional treatment) was associated with a larger improvement in motor functioning compared to the conventional treatment alone. In another randomized controlled trial, the efficacy of the VRRS based motor training and traditional rehabilitation (i.e., physiotherapy) in reducing pain intensity and knee disability, and improving quality of life, FIM scores and others measures, in patients with knee osteoarthritis after undergone orthopaedic surgery were tested (Gianola et al., 2020). The authors showed that the VRRS treatment was not superior to traditional rehabilitation in terms of pain relief and other functional outcomes. However, they concluded that it seems to improve the global proprioception despite this outcome was measured only after treatment and, as such, the difference could have been due to baseline differences between groups rather than to treatment itself.
Five studies evaluated the efficacy of VRRS based motor training deliver via TR. Like findings from Gianola et al. (2020), Fascio et al. (2022) found no difference between TR and traditional rehabilitation interventions for hip disability and functional independence in patients who underwent total hip arthroplasty. A multicenter randomized controlled study did not find any statistical differences in motor outcome between a group of patients with severe acquired brain injury that underwent a VRRS motor treatment delivered via TR and a group of patients with severe acquired brain injury that underwent a conventional face-to-face motor treatment performed at patients’ homes (Calabrò et al., 2023). Rather, both groups of patients showed improvements in global functional status and gross motor functions whereas no difference between baseline and follow-up measurements were noted for spasticity (Calabrò et al., 2023).
Piron et al. (2009) examined improvement in motor impairment of upper limb directly comparing VRRS based motor training delivered via TR, with conventional treatment, in post-stroke patients. The authors demonstrated significant improvement (as measured by FM and Ashworth Assessment Scale) in both groups. However, the VRRS treatment via TR group showed a higher score at the FM compared with that of the control group. Pagliari et al. (2021) showed that VRRS based motor training delivered via TR was more effective than conventional treatment carried out at home in improving balance (as measured by the Mini-BES Test) whereas no difference between interventions was demonstrated for unilateral gross manual dexterity (as measured by the Box and Block Test) in patients with multiple sclerosis. Finally, Goffredo et al. (2023) showed that VRRS treatment via TR improves static and dynamic balance and gait (as measured by the Mini-BES Test) more compared to at-home treatment without the use of any technological devices in patients with multiple sclerosis and Parkinson’s disease.
Neuropsychological rehabilitation
The VRRS was used for neuropsychological rehabilitation in 17 studies: four case reports, two uncontrolled trials, one quasi-randomised controlled trial, and ten randomised controlled trials.
Non-experimental design
Regarding case reports, no improvement in cognitive impairment (as indicated by a reliable change index equal to 1.3) after two months of VRRS based cognitive training was observed in an adult patient with neurocognitive and motor dysfunctions due to brain alterations linked to brain-stem radionecrosis (Tartamella et al., 2020). Similarly, no improvement in global cognition and executive functions was observed in a patient with neurodegenerative disease after VRRS training (De Luca et al., 2022a).
Maresca et al. (2018) reported improvement in general cognitive status, attention process and prefrontal cortex related executive functioning of a patient with spinal cord injury that underwent combined treatment including both standard treatment (i.e., psychological counselling, standard cognitive training, and physiotherapy) and VRRS cognitive training. Emedoli et al. (2021) implemented the “Action Observation Therapy” (AOT) via VRRS for the rehabilitation of buccofacial apraxia in an adult patient that underwent a neurosurgery resection of a right frontoparietal atypical meningioma. AOT is a relatively new rehabilitation approach that exploits mirror neuron mechanisms to treat neuromotor disorders (Buccino, 2014; De Stefani et al., 2021; Ertelt et al., 2007; Sgandurra et al., 2013). The patient was required to observe and subsequently reproduce different voluntary facial movements of an avatar projected on the VRRS. After the treatment, the patient showed an improvement in the quality and range of voluntary facial movements and gestures. This case report suggests that the application of AOT through VRRS could be a promising application of VRRS in the rehabilitation of buccofacial apraxia. Clearly, randomized controlled studies are needed to show the efficacy of AOT in combination with VRRS in the recovery of buccofacial apraxia.
Three single-arm studies were conducted with samples of patients with chronic low back pain (Alemanno et al., 2018, 2019) and myotonic dystrophy type 1 (Maresca et al., 2020). In patients with chronic low back pain, pain and cognitive functions improved during the VRRS based cognitive training (Alemanno et al., 2018, 2019). Similarly, patients with myotonic dystrophy type 1 showed improvement in neuropsychological functioning (Maresca et al., 2020). However, the absence of a control group is a relevant limitation of these studies since observed changes may be related to factors other than the VRRS treatment.
Experimental design
Eleven studies adopted a controlled experimental design with ten of these studies using randomization procedures. Two studies (Maresca et al., 2019; Torrisi et al., 2019) involved samples of post-stroke patients. Torrisi et al. (2019) evaluated the efficacy of VRRS cognitive training based on improving neuropsychological functions (including attention, memory, executive functions, and language skills) in post-stroke patients. The study lasted six months and included two phases: during the first one VRRS and standard cognitive treatments, respectively, were carried out at a rehabilitation centre; during the second phase the experimental group was treated with VRRS via TR modality, whereas the control group continued the traditional (paper and pencil) training at home. Before and after each phase, all participants underwent an extensive neuropsychological assessment. The authors observed significant improvement in the global cognitive level, as well as in the attentive, memory and linguistic skills in the VRRS. Moreover, significant differences between the VRRS group and the control group were shown in phonemic fluency, and learning and memory functioning, favouring the VRRS group only after the second phase (VRRS via TR) of the study. In another study, Maresca et al. (2019) investigated the efficacy of a linguistic treatment performed using VRRS and traditional linguistic treatment to treat language deficit in post-stroke patients with aphasia. The study lasted six months and included two phases: during the first one (implemented during hospitalization), the experimental group underwent linguistic treatment performed using VRRS, while the control group underwent the conventional speech therapy based on the same exercises as the experimental group, but using paper-pencil tools. In the second phase of the study, the experimental group continued linguistic treatment by means of VRRS via TR, while the control group continued the conventional speech therapy, which were provided by territorial services. The patients underwent an expansive neuropsychological assessment to assess several language skills, including naming, comprehension, repetition, reading, and calculation. The authors reported no between groups difference in comprehension, reading and calculation at baseline whereas at the end of the study (at the end of the TR) there were significant differences favouring the VRRS group. No differences were shown in repetition and naming.
The VRRS was used to improve language functions also in children with developmental language disorders (Cappadonna et al., 2023). The control group underwent conventional speech therapy, while the experimental group underwent a speech therapy program implemented via VRRS. Both groups improved in language functions after treatment. However, despite the authors stressed that the experimental group showed larger improvements compared to the control group, direct statistical comparisons between the two groups were not performed.
The VRRS was also used with children with dyslexia (Maresca et al., 2022). Maresca et al. (2022) found that VRRS cognitive intervention improved word-reading, homophonic writing and some index of the Wechsler Intelligence Scale for Children-IV (i.e., Full Scale IQ, Perceptual Reasoning Index, and Processing Speed Index) compared to conventional neuropsychological treatment in children with dyslexia.
Three studies, conducted from the same research group, involved patients with acquired/traumatic brain injury. De Luca and collaborators (De Luca et al., 2022b) showed that a neuropsychological attention training (i.e., Attention Process Training) implemented through VRRS is more effective than the same treatment based on paper and pencil exercises in improving attentive processes in patients with traumatic brain injury. In a further study, De Luca et al. (2023) evaluated the efficacy of VRRS cognitive training in improving executive functions of patients with traumatic brain injury. The experimental group underwent VRRS training for executive functions while the control group was provided with a conventional cognitive treatment. Comparing pre- and post-treatments scores, both the experimental and the control group improved. However, between-group post-treatment analysis showed significant differences only in some but not all measure of executive functions. Additionally, a multicenter study evaluated the efficacy of the VRRS based cognitive training implemented via TR in improving global cognitive functioning and executive functions in patients with severe acquire brain injury (Calabrò et al., 2023). Neuropsychological effects of the VRRS based treatment implemented via TR were compared with those of the conventional treatment performed at patients’ homes by a physiotherapist or a speech therapist. Again, between-group statistical analysis did not indicate any difference in cognitive outcomes between patients that underwent VRRS based treatment implemented via TR and patients that underwent the conventional treatment. Regarding these three studies with patients with acquired/traumatic brain injury, it is not clear whether they analysed independent data (participants were included only in one study) or dependent data (participants were included in more than one study).
Manenti et al. (2020) conducted a multicenter rater-blinded, controlled and randomized study to evaluate the efficacy of the VRRS based cognitive treatment compared to usual care treatment in enhancing cognitive functioning in patients with mild cognitive impairment. This study also tested the hypothesis that continuing the VRRS based cognitive treatment at home via TR may induce maintenance of the cognitive benefits obtained. Participants were assigned to one of three groups: 1) face to face cognitive VRRS treatment followed by VRRS via TR; 2) face to face cognitive VRRS treatment followed by at-home unstructured cognitive stimulation; and 3) those who received several conventional treatments in the clinical setting (e.g., reminiscence therapy and paper and pencil exercise) followed from no other treatment at home. The primary outcome was verbal episodic memory as measured by two different tasks (i.e., Free and Cued Selective Reminding Test and Rey Auditory Verbal Learning Test). Further, all participants underwent an extensive neuropsychological evaluation to assess other cognitive domains (i.e., language, attention, and visuoconstructional skills). Comparing the effects of face to face cognitive VRRS treatment with the conventional treatment on measures of verbal episodic memory (primary outcome) in the clinical setting, the authors showed that the VRRS treatment was more effective than the conventional treatment in improving some (but not all) sub-scores of verbal episodic memory as measure by the Free and Cued Selective Reminding Test, whereas no difference between treatments were observed for other measures of memory (i.e. Rey Auditory Verbal Learning Test). In addition, the VRRS treatment outperformed the conventional one on some secondary outcome measures (i.e., verbal fluency and visuoconstructional functions) whereas no between group difference was observed for others. Overall, these results support the efficacy of face-to-face VRRS treatment. Considering outcome measures at follow-up (after home treatment), overall the authors showed that cognitive VRRS-TR has comparable effects to the conventional rehabilitation treatment.
Two other studies (Leonardi et al., 2021; Pagliari et al., 2021) involved samples of patients with multiple sclerosis and compared the efficacy of conventional treatment rehabilitation with the VRRS rehabilitation in the clinical setting (Leonardi et al., 2021) and via TR (Pagliari et al., 2021). Leonardi et al. (2021) found that the VRRS based cognitive training improved global cognition, long term verbal memory, semantic verbal fluency and mental quality of life more than the conventional treatment. On the other hand, both treatments increased long term visuospatial memory and attention. Pagliari et al. (2021) found that VRRS cognitive training administered through TR had comparable effects to the conventional cognitive intervention. Finally, Goffredo et al. (2023) found that VRRS cognitive training administered through TR had comparable effects to an at-home self-administered treatment in improving global cognition of patients with multiple sclerosis and Parkinson’s disease.
Discussion
Overall, we found 30 studies using the VRRS in neuromotor and neuropsychological rehabilitation. Below we discuss only those studies that adopted an experimental approach.
We found 19 studies that report information on the use of the VRRS for neurological rehabilitation with ten studies including control group condition and/or randomization procedure (Kiper et al., 2011, 2014; Luque-Moreno et al., 2021; Pagliari et al., 2021; Piron et al., 2009; Gianola et al., 2020; Turolla et al., 2013; Calabrò et al., 2023; Goffredo et al., 2023; Fascio et al., 2022). Most of the studies suggest that VRRS based neuromotor training (alone or in combination with conventional interventions) may be more effective than the conventional treatment (Kiper et al., 2011, 2014; Luque-Moreno et al., 2021; Pagliari et al., 2021; Piron et al., 2009; Turolla et al., 2013; Goffredo et al., 2023).
Seventeen studies examined the use of the VRRS for neuropsychological rehabilitation with 11 studies including control group condition and/or randomization procedure (Maresca et al., 2019; 2022; Manenti et al., 2020; Torrisi et al., 2019; Cappadonna et al., 2023; De Luca et al., 2022b; 2023; Calabrò et al., 2023; Goffredo et al., 2023; Leonardi et al., 2021; Pagliari et al., 2021). Concerning face-to-face VRRS based cognitive training, most of the studies demonstrated the efficacy of the VRRS based cognitive in improving neuropsychological functions (Leonardi et al., 2021; Maresca et al., 2022; Manetti et al., 2020; De Luca et al., 2022b; 2023). Concerning the efficacy of the VRRS intervention via TR the majority of studies suggests that VRRS via TR could have a comparable effect to the conventional/control treatment (Calabrò et al., 2023; Manenti et al., 2020; Pagliari et al., 2021; Goffredo et al., 2023). However, two studies found that VRRS intervention via TR outperformed traditional treatment administered at home (Maresca et al., 2019; Torrisi et al., 2019).
It is important to consider a relevant aspect that might question the efficacy of the VRRS in the treatment of specific neuropsychological deficits. In some cases, there are inconsistent results of treatment effect on the same cognitive function both within the same study and between different studies. For example, the same study finds an improvement in some but not all measures of the same neuropsychological function (see e.g. memory measures in Manenti et al., 2020). Additionally, other studies report discordant results about the efficacy of VRRS in improving some cognitive functions (see for example phonetic fluency in Manenti et al., 2020; Torrisi et al., 2019; and TMT in De Luca et al., 2022b; 2023). Therefore, although studies generally agree in indicating the efficacy of VRRS in neuropsychological rehabilitation overall, the conflicting results concerning specific cognitive functions and tasks limit in some case the possibility of drawing firm conclusions on the efficacy of VRRS in addressing them. Therefore, future research needs to evaluate the efficacy of VRRS in the rehabilitation of specific neuropsychological functions in specific conditions and outcomes measures.
Recommendations for future research
Studies concerning the neurological and neuropsychological treatment using the VRRS in-person provide some evidence on its efficacy. However, VRRS was used for treating different dysfunctions and diseases for which a consistent body of evidence is lacking except for post-stroke conditions. Therefore, it is important to acknowledge that the discussed findings on the use of the VRRS for treatment are not generalizable across different populations of patients. Further studies are needed to examine and confirm the efficacy of the VRRS in specific populations. It is reasonable to assume that, based on quality of scientific evidence, the VRRS and VRRS via TR could be recommended for specific group of patients, and not others.
TR is particularly important for subjects with limited access to therapy due to geographical distance, transport difficulties or a lack of local services (Manenti et al., 2020). Our findings thus encourage future research to further test applications and efficacy of VRRS via TR.
VRRS was used for treating several dysfunctions and diseases. However, few studies investigated the use of the VRRS for neurological and neuropsychological rehabilitation of children and adolescents (Menici et al., 2021; Olivieri et al., 2013; Cappadonna et al., 2023; Maresca et al., 2022). Thus, controlled randomized studies are needed to test the efficacy of the VRRS and its TR application in the young population. Further, the analysed studies generally included short term follow-ups (i.e., evaluations soon after treatment).
Finally, detailed cost effectiveness and economic analyses should be performed to examine whether rehabilitation using the VRRS, during hospitalization and/or via the TR modality, reduces health care providers’ and patients’ costs compared with conventional (face to face) treatments or not.
Study limitations
The present study provides a recent and exhaustive literature review on research studies using the VRRS for rehabilitation. However, it has some limitations that should be kept in mind when interpreting its findings. First, as for all narrative/literature reviews, we did not provide an empirical synthesis of the findings of included studies. Second, as for all reviews, the quality of reported findings relies on the quality of statistical analysis of original studies and, as such, reported evidence are limited by original studies limitations (e.g., lack of control group and long-term follow-up, poor description and/or reporting of statistical analysis, lack of testing between group differences and between group analysis not controlling for important baseline covariates, multiple testing increasing the risk of false-positive findings, small sample size). Despite important initial efforts, more needs to be done to improve scientific evidence. Future systematic reviews with meta-analysis should address VRRS rehabilitation efficacy.
Conclusion
VRRS was widely used for treated several dysfunctions and diseases. The present study after narratively reviewing scientific evidence suggests that the use and efficacy of VRRS rehabilitative intervention for increasing neurological and neuropsychological functioning of patients is promising. However, further studies are needed in order to evaluate the efficacy of VRRS in the rehabilitation of specific neurological and neuropsychological functions. Moreover, the evidence is very limited for young patients. Future studies should also plan and analyse long-term follow-up as well as provide cost-effectiveness analyses.
Conflicts of interest
The authors have no conflicts of interest to declare.
Funding
This research was funded by the “5 per mille” 2021 – funds for biomedical research by Antonio Trabacca and by the Italian Ministry of Health (Ricerca Corrente funds).
Ethics statement
All procedures followed were in accordance with the ethical standards on human experimentation of the institutional Ethical and Scientific Committees and with the Helsinki Declaration of 1975.